NEW COMPETITION LICENSE APPLICATION All Applicants Must Be at Least 18 Years Old
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

RACING Focus on Performance
“EVEN MORE IMPORTANT THAN SAVING MONEY AND INCREASING UPTIME IS HOW OUR TIRE PRO GRAM POSITIVELY IMPACTS OUR PERFORMANCE COMMITMENT TO OUR SHIPPING CUSTOMERS.” The KKW fleet logo includes a checker flag and a “Performance In Transportation” tagline. The fleet’s 850 trailers proudly display that logo. The history behind the logo helps explain the fleet’s RACING focus on performance. KKW was founded in 1962. The Pomona, California, based carrier had nine tractors and ten trailers when TO SUCCESS Dennis Firestone purchased KKW in 1967. In California and ten of the other Western states, an TRACK SUCCESS attractive fleet of 300 trucks moves truckloads of After Dennis had spent several years getting KKW general commodities and LTL shipments of new home established and on track, he pursued a competitive hobby which turned out to be driving race cars. With a and office furniture. Those shipments move with a little luck and a lot of determination he became very focus on performance levels that exceed the shipping successful at his new hobby. At one point he had won customer’s expectations. 23 consecutive national open wheel races including the ’76 national championship in the amateur class Formula Ford. He then proceeded to win the profes- sional series ‘Indy Lights’ in ’79 winning 11 out of the 13 races in that series. His track success earned him the attention of the Indy Car community and garnered him a Championship Car ride for the Ontario 500 late in the ’79 season driving a Jim Hall/Roger Penske Indy Car. Dennis continued as an Indianapolis 500 driver from 1980, where he earned the honor of CART rookie of the year, through 1987. -

Cooper Tires Indy Lights Oval Challenge of St. Louis
Cooper Tir es Indy Lights Oval Challenge of St. Louis World Wide Technology Raceway – August 19 - 21 , 2021 – Rounds 1 3/14 Entry List 1.25 - mile oval as of August 9 , 20 21 Track Records: Qualifying – Juan Piedrahita 27.8890 = 161.354 mph August 26, 2017 Race – Zachary Claman 28.0370 = 160.502 mph August 26, 20 17 Two - lap qualifying run 55.962 = 160.823 mph August 26, 2017 N o. Driv er Hometown Residen ce T eam Sponsors 2 Sting Ray Robb (R ) Payette, ID Payette, ID J uncos Hollinger Racing Sekady Capital/Goodhea r t - Fire hou se Animal Cent ers 5 Alex Peroni (R) Hobart, Australia Tra nmere , Austral ia Carlin Blundstone /Tasmania/RDM F ast Ferries 7 Christi an Bogle (R) Covingto n, LA Covington, LA Carlin Pelican Energy 11 Antonio Serravalle (R) Toronto, Canada Unionv ille, Canada Pserra Racing / AS Promotions LedgeMark Homes LivGreen / T ycoon C apital Limited 17 Devlin DeFrances c o (R) Miami , FL Miami , FL A n dretti Stein brenner Auto sport PowerTap Dallara 24 Ben ja min Pedersen ( R) Copenhage n, Seattle, WA Global Raci ng Group w / Colibri Capital/Ameriprise Financial/Sabelt /DirtFish Denm ark HMD Motorspo rts 26 Linus Lundqvist ( R) Stockho l m, Sw e den Stockholm , Sweden/ Globa l Racing Gro up w/ Ut ah Airguns/ H PD/Global Racing Grou p/ FX Airguns/ Indianapolis, IN H MD Mo torspo rts Paytrim /JU LA 27 Robert Megennis New York, NY New York, NY Andretti Auto sport An d retti Autosport Dallara 28 Kyle Kirkwoo d (R) Jup iter, FL Jupiter, FL Andretti A uto sport Road to Indy / Cooper Ti r e s / Construc ti on Contractor s Club D allar a 51 T oby Sowery Ca mb ridge , Engl and Camb ri dge, England Juncos Hollinger Racing m - start/Kumpf 68 Danial Fr os t ( R) Si nga pore Miam i, FL Andre tti Au tosp or t DEN - JET Dal lara 79 Da vid Malukas Chicago, IL Chicago, IL HMD Motorsports H MD Tru c king R = Serie s Rooki e . -
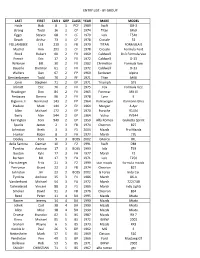
Entry List - by Group
ENTRY LIST - BY GROUP LAST FIRST CAR # GRP CLASS YEAR MAKE MODEL Hatle Bob 8 1 PCF 1989 Swift DB-3 Strong Todd 16 1 CF 1974 Titan Mk9 Egger Steven 68 1 CF 1979 Lola T540 Beach Arthur 73 1 CF 1978 Crossle 32 FOLLANSBEE LEE 210 1 FB 1970 TITAN FORMULA B Madrid Kim 291 1 CF 1978 Crossle Formula Ford Rinck Robert 00 2 FV 1969 Caldwell D13 Formula Vee French Eric 17 2 FV 1972 Caldwell D-13 Wilkman Bill 30 2 FV 1982 Chrimilton Formula Vee Bauerle Dietmar 61 2 FV 1972 Caldwell D-13 Walters Dan 67 2 FP 1960 Sunbeam Alpine Gerstenberger Todd 70 2 FF 1971 Titan MK6 Jones Stephen 71 2 EP 1971 Triumph GT6 Inkrott Eric 76 2 FV 1975 Fox Formula Vee Readinger Don 84 2 FV 1965 Formcar MK III Ambayec Dennis 96 2 FV 1978 Lynx B Biglione Jr Normand 143 2 FP 1964 Volkswagen Karmann Ghia Pladson Mark 144 2 EP 1964 Morgan 4-Apr Allen Michael 172 2 EP 1970 Porsche 914/4 Berry Alan 544 2 EP 1964 Volvo PV544 Farrington Tom 949 2 EP 1959 Alfa Romeo Giulietta Sprint Sparks James 2 3 FB 1974 Chevron B27 Johnston Brett 3 3 F1 2004 Mazda Pro Mazda Hunter Robin 8 3 FA 1977 March 77b Dooley Tom 9 3 BOSS 2002 GForce IRL della Santina Damian 10 3 F2 1991 Swift DB4 Tymkiw Andrew 17 3 BOSS 1993 lola T93 Buxton Kyle 17 3 FA 1977 March F2 Barham Bill 17 3 FA 1971 Lola T250 Harnsberger Fritz 21 3 F2 1999 star mazda formula mazda Perryman Grant 22 3 FB 1974 Chevron B27 Johnston Jim 23 3 BOSS 2002 G Force Indy Car Tymkiw Andrew 35 3 F1 1986 March 86-A Vanderhurst Michael 54 3 FA 1972 March 722/74B Tjelmelarad Vincent 88 3 F1 1986 March Indy Lights Smoker David 91 3 FB 1976 Chevron B34 Reed Peter 11 4 SM 1995 Mazda Miata Barnes Jeremy 14 4 SM 1990 Mazda Miata Johnk Carl 38 4 SM 1990 Mazda Miata Allen Mike 38 4 SM 1990 Mazda Miata Droese Brandon 02 5 BS 1987 Mazda RX 7 Kinna Michael 05 5 BS 1972 BMW 2002 Graham Wayne 6 5 BS 1973 Mazda RX3 Konkle Jr. -
Spotter Guide (PDF)
This year will mark the Firestone brand’s 67th Indy 500 victory. Firestone has more Indy 500 wins than all other tire manufacturers combined. CAN HINCH GO FROM THE POLE TO VICTORY LANE: James Hinchcliffe wrote the latest chapter of his comeback story when he scored the pole for the 100th Indianapolis 500 last weekend. History will be on his side this weekend as the Indy 500 pole has gone on to win the race 20 times. Forty-three times, the winner has come from the front row, the last time in 2010 with Dario Franchitti. Will Hinch covert his Verizon P1 Award into the Borg-Warner Trophy? Chris Jones/IMS Photo WHAT TO WATCH FOR THIS MONTH: IT’S NOT WHERE YOU START…: The last four Indianapolis 500 winners have started outside the top 10, including Juan Pablo Montoya, who came from 15th to win in 2015. With depth throughout the 33-car field for the Indy 500, including former winners Montoya, Scott Dixon and Tony Kanaan starting from the fifth row or further back, can another star drive through the field to win the race? SECOND-GENERATION STARS HOPE TO ADD TO FAMILY LEGACY: The latest generation from two of open-wheel racing’s most familiar families comes to Indianapolis in hopes of adding to the family legacy. Marco Andretti—the grandson of 1969 winner Mario Andretti and son of Michael Andretti—has finished in the top three at Indy three times in his nine previous starts. He hopes to give his father’s team its fourth Indianapolis 500 win. -

Than 27 Years of Helping Sick Children Through Motorsports
More than 27 Years of Helping Sick Children Through Motorsports The Program The Team Fast Facts Media Coverage Photos - Special Events www.racingforkids.org The Program Racing For Kids® is a unique national charity, which uses the popularity of motorsports to bring attention and funding to the health care needs of children and child health institutions. At the heart of the program are visits to Children’s Hospitals by the Racing For Kids drivers in the cities where they race. The drivers spend time with each sick child, sharing stories about their racing careers, signing autographs and giving out the popular Racing For Kids hats. For many hospitalized youngsters, these visits by the racers are the lone bright spot in what is often a rather gloomy experience. Attending physicians report that these visits play an important part in each child’s recovery therapy. Racing For Kids representatives have visited close to 30,000 sick children in more than 575 hospital visits in the United States, Canada, Mexico, Brazil, Japan and Australia. Another important aspect of the Racing For Kids program is the funding that has been raised for Children’s Hospitals across the country. Since its founding in Detroit in 1989, Racing For Kids has raised more than $6.5 million through donations, specific fund raising events and in-kind gifts. Major sponsors of Racing For Kids include Humana, Inc., Bridgestone Firestone Trust Fund, TranSystems, Meridian Health Plan of Michigan, Benson Ford, Jr. and Douglas E. Fregin. Toyota Motorsports and The Grand Prix Foundation of Long Beach have made Racing For Kids a major charity of The Toyota Grand Prix of Long Beach. -
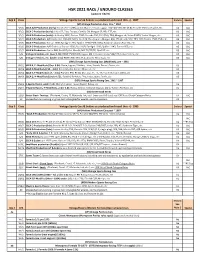
HSR 2021 RACE / ENDURO CLASSES (Updated 1/8/21)
HSR 2021 RACE / ENDURO CLASSES (updated 1/8/21) Grp 2 Class Vintage Sports Cars & Sedans as produced and raced thru +/- 1967 Enduro Special (VP) Vintage Production Cars, thru ~ 1967 VP/1 SCCA A/B-Production (early): Corvette C-1 (283); Aston Martin; Ferrari; Jaguar 120/140/150, XKE (3.8); Porsche 356 Carrera/GS, etc. V3 IAC VP/2 SCCA C-Production (early): Lotus S7, Elan, Europa; Ginetta G4; Morgan SS; Alfa GTZ, etc. V3 IAC VP/3 SCCA D-Production (early): A-Healey 3000; Datsun 2000; Porsche 356, 911 (FIA); TR4; Morgan +4; Volvo P1800; Yenko Stinger, etc. V4 IAC VP/4 SCCA E-Production: A/R Giulia; A-H 100-4/6; MGB; Fiat 124; Elva Courier; Morgan 4/4; 356 (drum), 912; TR3, GT6; Turner 1500; TVR, etc. V5 IAC VP/5 SCCA F-Production: Datsun 1600; Spridget 1275; Spitfire 1296/1500; MGA; Sunbeam Alpine; Fiat 124, etc. V5 IAC VP/6 SCCA G-Production: A/R Giulietta; Datsun 1500; Fiat X1/9; Spridget 1100; Spitfire 1147; Turner 950, etc. V5 IAC VP/7 SCCA H-Production: Sprite 948; Fiat 850; Fiat Abarth; MG TC/TD/TF; Opel GT, etc. V5 IAC S/5 Vintage B-Sedans, etc. (over 1.5L): BMW 1500/1600; Jaguar Mk II; Corvair; Volvo 544/122; Lotus Cortina, etc. V4 IAC S/6 Vintage C-Sedans, etc. (under 1.5L): BMW 700; Mini; Fiat; Abarth; NSU; Saab, etc. V5 IAC (VM) Vintage Sports Racing Cars (Modifieds), pre ~ 1961 VM/1 SCCA B, C -Modifieds (Over 3.0L): Devin, Jaguar; Echidna; Lister; Scarab; Ferrari; Bocar, etc. -

3/17/21 Barber Motorsports Park April 15-18, 2021
BARBER MOTORSPORTS PARK APRIL 15-18, 2021 TUESDAY, APRIL 13, 2021 9:00 AM RTI SERIES TRANSPORTERS LOAD-IN 2:00 PM MANUFACTURERS LOAD-IN WEDNESDAY, APRIL 14, 2021 8:00 AM - 3:00 PM REGISTRATION OPEN (HAMPTON INN, 310 REX LAKE RD. LEEDS, AL) 9:00 AM INDYCAR SERIES TRANSPORTER LOAD-IN 9:00 AM RTI TEAMS LOAD-IN 12:30 PM - 5:30 PM TECH OPEN (USF2000 & IP2) 2:30 PM - 5:30 PM TIRE SCANNING FOR USF2000 & IP2 (OPEN TEST TIRES) THURSDAY, APRIL 15, 2021 7:00 AM - 3:00 PM REGISTRATION OPEN (HAMPTON INN, 310 REX LAKE RD. LEEDS, AL) 7:00 AM - 5:00 PM TECH OPEN (USF2000 & IP2) CLOSED FOR LUNCH 1:00 PM – 2:00 PM 8:00 AM - 1:00 PM USF2000 & INDY PRO 2000 TESTING (TRACK RENTAL) 8:00 AM - 9:00 AM USF2000 T1 9:00 AM - 5:00 PM TECH OPEN (INDY LIGHTS) CLOSED FOR LUNCH 12:00 PM – 1:00 PM 9:15 AM - 10:15 AM INDY PRO 2000 T1 10:45 AM - 11:45 AM USF2000 T2 12:00 PM - 1:00 PM INDY PRO 2000 T2 12:00 PM - 2:00 PM TIRE SCANNING FOR USF2000 & IP2 (RACE EVENT TIRES) 1:00 PM - 2:00 PM TIRE SCANNING FOR INDY LIGHTS 1:15 PM - 1:45 PM RADICAL CUP P1 2:00 PM - 2:30 PM USF2000 P1 2:45 PM - 3:15 PM INDY PRO 2000 P1 3:00 PM INDYCAR TEAMS LOAD-IN 3:30 PM - 4:15 PM INDY LIGHTS P1 4:30 PM - 5:00 PM RADICAL CUP P2 FRIDAY, APRIL 16, 2021 7:30 AM - 4:00 PM REGISTRATION OPEN (HAMPTON INN, 310 REX LAKE RD. -

120417 Newsletter
© The Official Newsletter Of The American Auto Racing Writers and Broadcasters Association Nov / Dec 2017 Vol. 50 No. 11 Championship winning Furniture Row Racing team celebrates in victory lane. The Ford Championship weekend at the Homestead-Miami Speedway featured many storylines and crowned three new champions. Read Joe Jennings take on page 2 American Auto Racing Writers & Broadcasters Association, Inc. (www.aarwba.org) “Dedicated To Increasing Media Coverage Of Motor Sports” By Joe Jennings The Ford Championship weekend at the Homestead-Mi- eight wins, 19 top five's, 26 top 10s and three poles. For Bar- ami Speedway featured many storylines and crowned ney Visser's Furniture Row Racing team, it was the first cham- three new champions. pionship as it was for crew chief Cole Pearn. As usual, NASCAR closed out its long season with three exciting races that featured intense action with three new champions being crowned; namely Martin Truex Jr., Wil- liam Byron and Christopher Bell. Many storylines dotted the weekend with the biggest one focusing on the final Cup run by fan favorite Dale Earn- hardt Jr. The center ring spotlight focused on the four drivers at- tempting to win the lucrative Monster Energy NASCAR Cup Series championship. And the quartet of Martin Truex Jr., Kyle Busch, Kevin Harvick and Brad Keselows- ki gave it their all during the 267-lap season finale much to the delight of the sold-out grandstand and a national television audience. Earnhardt and his legion of fans enjoyed their day in the sun. Starting last due to an engine change, NASCAR's most popu- lar driver was never in contention, ending up 25th but accom- plishing his goal of finishing the race. -

NASCAR Slim Jim All Pro Series “Kentucky 150” Start Time: 9:00 P.M
ALL-TIME RECORDS Kentucky Speedway Firsts First Race: NASCAR Slim Jim All Pro Series “Kentucky 150” Start Time: 9:00 p.m. Attendance: 36,210 June 16, 2000 Time of Race: 1 hour, 22 minutes, 9 seconds Length: 150 miles, 100 laps First Champion: Billy Bigley, Jr., No. 28 Peerless Woodworking/Nevamar Decorative Services Chevrolet Monte Carlo NASCAR Slim Jim All Pro Series “The Kentucky 150” June 16, 2000 First Pole Sitter: Brian Smith, No. 20 Juba Glass Chevrolet Monte Carlo NASCAR Slim Jim All Pro Series Qualifying Time: 150.038 mph “The Kentucky 150” June 16, 2000 First Margin of Victory: 0.248 seconds - Billy Bigley, Jr. NASCAR Slim Jim All Pro Series “The Kentucky 150” June 16, 2000 First Winner’s Average 111.747 mph – Bill Bigley, Jr. Speed: NASCAR Slim Jim All-Pro Series “The Kentucky 150” June 16, 2000 First Lap Led: Jeff Fultz, No. 54 Cleaver Brooks/C&C Boilers/Honeywell Chevrolet Monte Carlo NASCAR Slim Jim All Pro Series Time: 150.538 mph “The Kentucky 150” June 16, 2000 First Purse: $95,050 NASCAR Slim Jim All Pro Series “The Kentucky 150” June 16, 2000 First Winning Crew Chief: Bill Bigley, Sr. NASCAR Slim Jim All Pro Series “Kentucky 150” June 16, 2000 Kentucky Speedway Single Race Records 1.5-mile Tri-Oval KENTUCKY SPEEDWAY RECORDS / 2 Overall Records ARCA Racing Series (ARS); ASA (American Speed Association National Tour); FIL (Firestone Indy Lights); IICS (IZOD IndyCar Series); NCWTS (NASCAR Camping World Truck Series); NEDSS (NASCAR Elite Division Southeast Series); NGDS (NASCAR Goody’s Dash Series); NNS (NASCAR XFINITY Series); NSCS (NASCAR Sprint Cup Series); USCS (USAC Silver Crown Series). -

SVRA Cars and Classes
General Outline of Groups and Classes for The WeatherTech® International Challenge with Brian Redman presented by HAWK at Road America ~ 2020 (revised 11/11/19) (1) Can-Am (1965 ~ 1974) Class CA1 Unlimited (including all turbocharged) Class CA2 Small block (over 5.9L) Class CA3 Monocoque (under 5.9L) Class CA4 Tube frame (unlimited) Class CA5 USRRC (1962-1968) Treaded tires (2) (a) Vintage Production Class VAP Vintage A-Production Class VBP Vintage B-Production Class VCP Vintage C-Production Class VDP Vintage D-Production Class VEP Vintage E-Production Class VFP Vintage F-Production Class VHP Vintage G/H-Production Class VBS Vintage B/Sedans (1.5 ~ 1.8L) Class VCS Vintage C/D Sedans (under 1.5L) (b) Vintage Sports Racing Cars Class VCM Vintage C Modified ~ Specials, Sports Racers & Modifieds (over 3000cc) Class VEM Vintage D/E Modified ~ Specials, Sports Racers & Modifieds (1600-3000cc) Class VFM Vintage F Modified ~ Specials, Sports Racers & Modifieds (1100-1500cc) Class VGM Vintage G Modified ~ Specials, Sports Racers & Modifieds (850-1100cc) Class VHM Vintage H Modified ~ Specials, Sports Racers & Modifieds (under 850cc) Class VDSR Vintage D Sports Racers (under 1.0L) (c) Post Historic Street Stock Class SSD Post Historic Street Stock; Firehawk, Escort Series, IT, etc. as appropriate (4) (a) Monoposto Classic Formula Cars (thru ~ 1972) Class VFA Formula 2 & pre 1966 Formula 1 Class VFB Formula B Class VFC Formula C & Later Formula Junior Class VFF Pre-1973 Formula Ford (Dunlop/Avon/Hoosier spec tires, steel wheels only) Class VFJ Formula Junior (Dunlop L tires) Class VFV Formula V, Front Engine Formula Junior (b) Monoposto Formula 70, post 1972, etc. -

The Road to Indy Creates That Structure for Someone Like a Young Kid Who Races Karts and Wants to Be an Indycar Driver.”
2021 ROAD TO INDY – PROVEN FORMULA 286 DRIVERS have participated in the Road to Indy since its inception 31 CHAMPIONS 11 SEASONS have been crowned on the Road to Indy 23 ROAD TO INDY 34 ALUMNI DRIVERS have been NTT INDYCAR SERIES were on the NTT INDYCAR SERIES race winners starting grids in 2020 23 OF THE 33 INDY 500 $17,413,500 STARTERS IN 2020 value of prizes and awards distributed were Indy Lights graduates, including eight to date since the inception of the Road to Indy Indy Lights champions THE PROGRESSION STEPSSTEPS The Road to Indy Presented by Sanctioned by INDYCAR, the Cooper Tires is where tomorrow’s stars Road to Indy was introduced race today, and its success as a in 2010 and has become the most successful driver springboard to the NTT INDYCAR development program in the SERIES has never been more world, providing a unique, apparent. scholarship - funded path to reach the NTT INDYCAR SERIES and the Indianapolis 500. Scholarship valued at $1,289,425 Includes entry into at least three Scholarship NTT INDYCAR SERIES valued at events for 2022 including the $ 718,065 Indianapolis 500 Scholarship valued at $ 401,305 THE MOST EFFECTIVE DRIVER DEVELOPMENT PLATFORM IN THE WORLD EXPOSURE • Premier venues with all events in support of NTT INDYCAR SERIES race weekends • Full Indy Lights race coverage on NBC Sports Gold in the U.S. and REV TV in Canada; worldwide live streaming of all on - track activity; dedicated broadcast channels on Apple TV, Amazon Fire, Roku and the Xbox One Official App; global coverage and original content on RoadToIndy.TV; full coverage on the Pennzoil INDYCAR Radio Network. -

CHRIS BELLOMO Started His Racing Career in 2017
VIP MOTORSPORTS EXPERIENCE CALIFORNIA 8 HOURS PRESENTED BY PIRELLI WORLD CHALLENGE WeatherTech Raceway Laguna Seca October 26-28, 2018 POINT OF CONTACT : VIP CONCIERGE Alicia busch (707) 478-3333 [email protected] Hospitality Coordinator “We are so happy you could join us for what is sure to be an epic event. Please feel free to contact me with questions and concierge inquiries.” Olivia Camilleri (415) 816-0412 [email protected] Executive Assistant to Kevin Buckler, CEO POINT OF CONTACT : MARKETING & PR Kristine Youngberg (707) 478-3333 [email protected] Brand & Communications Director (707) 935-3999 (707) 939-7967 theracersgroup.com adoberoadwines.com @theracersgroup @adoberoadwines 1995 S. McDowell Blvd. Petaluma, CA 94954 | (707)935-3999 REGESTRATION & RACE DAY ARRIVAL Credentials, long pants, covered shoulders and closed-toe shoes are required for entry into the pits. REGISTRATION OFFICES FOR RACE EVENT CREDENTIALS Hyatt Regency Monterey 1 Old Golf Course Rd Monterey, CA 93940 +1 831-657-6560 Thursday, October 25: 9:00AM – 5:00PM Hyatt Regency Friday, October 26: 8:00AM – 4:00PM Hyatt Regency Saturday, October 27: 8:00AM – 4:00PM Hyatt Regency Sunday, October 28: 7:00AM – 11:00AM Hyatt Regency Map to WeatherTech Laguna Seca Raceway SCHEDULE #67 PORSCHE GT4 CLUBSPORT MR CHRIS BELLOMO started his racing career in 2017. After a few local track days with a good friend he was hooked. A 3 day SCCA school sealed the deal. That led to several SCCA races in a Spec Miata, which then led to his coach introducing him to TRG and his current Porsche Cayman Clubsport MR. Chris started racing his Porsche when he joined the Pirelli Trophy West USA Series at the start of 2018.