A Population-Based Study on Radical Prostatectomy in France
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2270 B.C. Lacaunes Series, Tarn
{RADIOCARBON, VoL. 15, No. 3, 1973, P. 514-533] LYON NATURAL RADIOCARBON MEASUREMENTS IV J. EVIN, G. MARTEN, and Ch. PACHTAUDT Radiocarbon Laboratory, Geology Department, University of Lyon I, Nuclear Physics Institute, 69, Villeurbanne, France INTRODUCTION This list includes most of the samples measured from June 1970 to June 1972 and some other results not yet published in previous date lists. Chemical treatment of samples and counting technique remain as described previously (R., 1969, v. 11, p.112-113; R., 1973, v. 15, p. 134-155). See also Longin (1971) for bone preparations performed by solubilization of collagen in acid hot water. Ages are calculated using the half-life value 5570 with 1950 as refer- ence year. The statistical errors, corresponding to one standard deviation, include contemporary standard, background, and sample counts. ACKNOWLEDGMENTS We thank Yvette Chiarlone for chemical preparations and most rou- tine operations. We are grateful to J. Flandrin and P. Elouard, Dept. of Geology, for their continuous support, and to A. Sarazin and the staff of the Nuclear Physics Institute for their help and technical assistance. SAMPLE DESCRIPTIONS I. GEOLOGIC SAMPLES 4220 ± 130 Ly-503. Roudil, Tarn 2270 B.C. Clayey peat from 47 to 55cm depth in Roudil peat bog, near Arfous, Tarn (43° 26' N Lat, 2° 31' E Long.) Coll. and subm. 1971 by J. L. de Beaulieu, Lab. Bot. Hist., Univ. Provence, Marseille. Level marks begin- ning of Fagus increase in pollen diagram. Comment (J. L. de B.): low alt. of site might suggest a Sub-Atlantic age for Fagus increase, as in Malarou- met peat bog, Dordogne: Lv-387: 1570 ± 80 B.P. -

Cordes-Sur-Ciel OCCITANIE, FRANCE
Cordes-sur-Ciel OCCITANIE, FRANCE Photographed by Jon Davison First published in 2018 by Eye in the Sky 9 Rue des Mitons 81170 Cordes-sur-Ciel Occitanie France All photographs, design and production © Jon Davison 2018 Text by Jon Davison & Jude Brazendale Edited by Jude Brazendale French translation and editing by David Cassard. The publishers wish to thank Marie-Christine Lassery, Véronique Lanas and Quentin Palaffre at the Office de Tourisme du Pays Cordais du Pays de Vaour, for their valuable help in the production of this book. Page 39 (and right): Thanks to TomKr, designer of the heraldic crests The heraldic crest of for Wikipédia and their ‘Projet Blasons’. Cordes-sur-Ciel. The slightly flattened version of the Printed by Balto Print, Kaunas, Lithuania. Occitanie cross refers to the longer east west axis of the town, compared to the All photographs in the publication are available to purchase as prints shorter north south axis. or digital files. Please contact the author; [email protected] Images and text © Jon Davison /Eye in the Sky 2018 ISBN: © Eye in the Sky Productions 2018. Every attempt has been made to record accurate information and facts, but bearing in mind the age of Cordes, some ‘facts’ may be based on or sourced from differing views. The publishers can not be held responsible for recording the accuracy of information they have been given. All photographs are © Jon Davison 2018 and the images are accurate depictions of what was recorded. CORDES | two CONTENTS CONTENTS 3 INTRODUCTION 4 THE TOWN 12 Le Planol / Les Remparts 22 Porte de la Jane 26 Porte des Ormeaux 28 Rue Saint Michel 32 Grand Rue Raymond 34 24 La Halle 38 Place de la Bride 44 Portal Peint 48 Porte du Vainqueur 54 Rue de la Barbacane 56 Porte de l’Horloge 60 Cordes du bas 62 THE LANDSCAPE 64 NEARBY 94 RIGHT: Grand Rue Raymond VII on New Years Eve, looking west. -

Les ARTS En FÊTE Au VILLAGE À SOUAL (81 – TARN) « Les Arts Dans Tous Les Sens »
Les ARTS en FÊTE au VILLAGE à SOUAL (81 – TARN) « Les Arts dans Tous les Sens » 9 h – Petit Déjeuner des Randonneurs, avec mignardises, offert Par la Municipalité de SOUAL. 9 ½ h – Départ de la Randonnée. A) RANDONNEE PEDESTRE. ** Petite Boucle des Pigeonniers. Départ : Devant La Statue de la Vierge des Promenades de SOUAL. Un peu d’Histoire : Sainte – Vierge couronnée, car elle est « Reine de la Paix », avec une Longue tunique plissée à l’Antique, et cheveux longs dénudés. Présence, à SOUAL, de l’enfant Jésus, âgé de 01 à 02 ans, porté soit Sur le bras droit, soit à gauche comme ici, soit les deux mains tendues En adoration - C’est la famille du Docteur ALBERGUE-SERMET qui fût à l’origine de la Statue de la Vierge en cédant en 1869, une parcelle de terre de 530 m2 pour édifier la Statue - Une souscription de la population de la Paroisse de SOUAL permit d’ériger la Statue de la Vierge dont on peut la dater de 1896 (Pas de plaque sur le socle) Socle en pierre sablée de NAVES et Statue en métal –Elle présente sur son socle circulaire, Dans un blason en cœur, un Hymne à La Vierge « L’AVE MARIS STELLA » 4ème Strophe, ainsi traduit « Montre Toi notre Mère, Que par Toi reçoive nos prières, Celui qui pour nous a bien voulu être Votre Fils » Sur le sommet du socle, en couronne, il existe des lettres séparées, un peu effacées et surtout peu compréhensibles « AVE PRONOBIS TERA DAE » « Salut pour nous, Toi Reine » Sur la base du socle, on retrouve les Têtes des animaux symboliques des QUATRE Évangélistes, l’Aigle (Pour JEAN) – Le Lion (Pour MARC) – Le Taureau (Pour LUC) et le Bélier (Pour MATHIEU). -

Commune De Brassac Dossier Communal Synthétique Des Risques
PRÉFECTURE DU TARN Commune de Brassac Dossier Communal Synthétique des risques majeurs Information des populations © PRÉFECTURE DU TARN / SIDPC PRÉFECTURE DU TARN DOSSIER COMMUNAL SYNTHÉTIQUE COMMUNE DE BRASSAC - 2 - PRÉFECTURE DU TARN DOSSIER COMMUNAL SYNTHÉTIQUE COMMUNE DE BRASSAC Commune de Brassac Dossier Communal Synthétique des Risques Majeurs Arrondissement de : CASTRES Ministère de l’écologie Canton de : BRASSSAC et du développement durable N° INSEE : 81037 Préfecture du Tarn Population : 1 462 habitants Service interministériel de défense et de protection civile - 3 - PRÉFECTURE DU TARN DOSSIER COMMUNAL SYNTHÉTIQUE COMMUNE DE BRASSAC Ce dossier a été réalisé en collaboration avec le Service interministériel de défense et de protection civile de la Préfecture du Tarn, les services de l’État et du département. Préfecture du Tarn Service interministériel de défense et de protection civile Direction départementale de l’agriculture et de la forêt Direction départementale de l’équipement Direction régionale de l’industrie, de la recherche et de l’environnement Services départementaux de l’éducation nationale Service départemental d’incendie et de secours Ce dossier a été réalisé par : Magali PONS Docteur en Géographie Expert Consultant 8, rue Jugan F-34090 MONTPELLIER Tél. / Fax. : 04 67 72 02 67 [email protected] - 4 - PRÉFECTURE DU TARN DOSSIER COMMUNAL SYNTHÉTIQUE COMMUNE DE BRASSAC SOMMAIRE page • Préambule ………………………………………………………………………………………………………… 7 • Arrêté préfectoral …………………………………………………………………………………………… 8 • Risque majeur et information préventive ………………………………………………… 9 • Carte des zones à risque établie par les services de l'État …………………… 12 • Le risque INONDATION ………………………………………………………………………………… 15 1. Qu'est-ce qu'une inondation ? …………………………………………………………………… 15 2. Quels sont les risques d'inondation dans la commune ? ………………………… 16 3. Cartographie ……………………………………………………………………………………………… 20 4. -
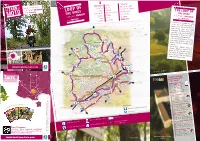
Loop of the Vines Couffouleux St
THETARN BY Loop of the vines i n between vineyard and forests MOTO Rabastens Mauriac Campagnac LOOP OF Couffouleux Broze Forêt de la Grésigne THE VINES Loupiac Montels St. Martin de l’Espinas in between vineyard Lisle-sur-Tarn Cahuzac-sur-Vère Forêt de Sivens Montans Andillac Les Barrières and forests w Gaillac Vieux Salvagnac THE LOOP OF Senouillac Le Verdier Rabastens THE VINES in between vineyard and forests In between the lowland, the valley of the Tarn and the vineyard of Gaillac on the side of the hills, this loop crosses some very varied landscapes. It follows mainly some calm little roads and it will enlight the tourists of bikers who like to alternate visits and wild nature. Lots of sites invite to a break : browse in the historic heart of a town in red bricks, to admire an old church, visit a winery… env. 140 km Among these multiple places to discover : Rabastens, Lisle-sur-Tarn, www.tourisme-tarn.com Gaillac and the vineyard of Gaillac, the forests of Grésigne and Sivens who in Autumn offer the surprising show of the Roaring Stags. Vineyard - Andillac TOURIST OFFICES & information desk on the circuit Bastides & Vignoble du Gaillac - 81600 ( catégorie II ) Office de tourisme de Pays Abbaye Saint-Michel - Gaillac in local tourist offi e circuits ces : Tel.: +33 (0)5 63 57 14 65 all th Find [email protected] www.tourisme-vignoble-bastides.com Avec Créations,Vent d’Autan - Phovoir. / Office of Rabastens - 81800 Hôtel de la Fite TM 2, rue Amédée de Clausade Tel.: +33 (0)5 63 40 65 65 Follow us : [email protected] www.tourisme-vignoble-bastides.com www.facebook.com/tarntourisme.sudouest Office of Lisle-sur-tarn - 81310 TM RoadTrip, D.Viet / CRTMP, J.L. -

Suivez Le Coq Suivez Le
Suivez le Coq Commune de Gaillac Promenade urbaine Ce sentier offre au promeneur différents aspects de la ville et permet l’évocation du 5 riche passé historique de la cité gaillacoise. De l’abbaye Saint-Michel, il descend vers km 1h40 la rivière pour suivre les berges du Tarn, la ville paraît alors bien loin ! Le quartier de l’Hortalisse et son dédale de sentes qui cheminent de jardins en jardins, raconte l’histoire des maraîchers qui, 140 m jusqu’à la moitié du XXe, alimentaient les marchés alentours. Après la traverse 128 m du centre historique, le sentier se dirige vers les rives Thomas (ancien ravin Itinéraire agréé par la Fédération française de la comblé et aménagé au XIXe), randonnée pédestre. pour redescendre vers le Tarn et son ancien port, très prospère jusqu’à l’avène- ment du chemin de fer. Abbatiale de Gaillac © Mairie de Gaillac Code de balisage Vous pouvez rencontrer d’autres Bonne direction couleurs de balisage sur le terrain. Changement de direction Elles sont indiquées à l’intérieur de Mauvaise direction cette fiche. : JOUVE, Mayenne. Info-Plus : Info-Culture : Office du tourisme de Gaillac Abbaye Saint-Michel – 81600 Gaillac Dès le Moyen Âge, la figure du coq Tél. 05 63 57 14 65 est associée aux actes importants [email protected] ou au grands évènements de la vie, à Gaillac : sceau des consuls, poids de Mairie de Gaillac – Place d’Hautpoul la ville, blason, etc. Les vins de Tél. 05 63 81 20 20 Gaillac étaient aussi connus sous le www.ville-gaillac.fr nom « vins du coq », en référence à la marque à feu qui était apposée sur les tonneaux. -

TRIENNALE INTERNATIONALE DE GRAVURE EN TAILLE-DOUCE DE LISLE-SUR-TARN NOIR ET BLANC OU COULEUR 5Ème Édition
TRIENNALE INTERNATIONALE DE GRAVURE EN TAILLE-DOUCE DE LISLE-SUR-TARN NOIR ET BLANC OU COULEUR 5ème édition RÈGLEMENT La Triennale de Gravure en taille-douce de LISLE-SUR-TARN se déroulera de mars à juin 2022 au Musée Raymond LAFAGE de LISLE-SUR-TARN · Adresse de l’exposition : Triennale de Gravure en taille-douce de LISLE-SUR-TARN Musée Raymond LAFAGE 8, Place Paul Saissac 81310 LISLE-SUR-TARN · accès : autoroute A 68, sortie 8 ou Nationale N88, entre Albi et Toulouse 1. Chaque participant devra présenter cinq estampes originales dans les techniques de la taille- douce : burin, pointe sèche, manière noire, eau-forte, aquatinte, vernis mou, sucre… Les œuvres seront encadrées par nos soins dans des cadres en alu de formats : 24x30cm – 30x30cm- 30x40cm - 40x40cm - 40x50cm - 50x50cm - 50x60cm - 50x70cm 2. Les œuvres présentées devront avoir été réalisées au cours des trois dernières années. 3. La sélection a) Sélection des artistes : Une présélection se fera par voie dématérialisée, les participants enverront une version numérique de leurs gravures, + curriculum vitae, + le bulletin de participation avec mentions obligatoires avant le 30 septembre 2021 à l’adresse internet suivante : [email protected] Si le participant est sélectionné, il recevra une notification sur son adresse internet personnelle fin octobre ou mi-novembre 2021. Le jury sélectionnera 3 estampes par artiste. Réunion du jury qui sélectionne les participants à l’exposition b) Sélection dématérialisée : Les images que vous nous envoyez doivent pouvoir être utilisées pour l’édition d’un catalogue. Elles doivent donc être d’une qualité suffisante pour l’édition d’un beau livre. -

Welcome to Your Volunteering Project with Les Ateliers Castres, France Who Are We
Welcome to your Volunteering project with Les Ateliers Castres, France Who are we ? The center "Les Ateliers " is located in a renovated factory of 4000m² . It combines: offices, co-working space, a restaurant, a upcycling/ recycling workshop and organise some events. This gathering of structures within this same site reinforces the possible synergies and their visibility. On a daily basis around a 100 of people evolve in Les Ateliers, in between the people working in the co working or the offices spaces, their targets ( for the trainings, activities,etc..), the restaurant and shop costumers. We also host various workshops: yoga, tap dancing,meditation, etc... The cooperative " Les Ateliers" has 2 main activities: 1- federate and promote the economic development of structures with a social, environmental or territorial purpose: animation of membership, professional animation and organization of working groups by sector, 2- generate new activities and new sustainable jobs: development of a restaurant of local products (45 covers per service and 7 services per week), development of recycling of furniture offer, and weekly cultural programming (work in progress). The team of Les Ateliers Marcin Wolak ( your tutor for the missions in the Recyclerie) Mathilde Nouvel ( your tutor for the missions related to the restaurant) Sabiane Douheret ( the coordinator) Laetitia Barbry( Your mentor – not a staff from Les Ateliers) Les Ateliers and the city of Castres Castres is a city of about 4000m2 in Tarn, Occitanie, and about 40000 inhabitants south of France. If you ask french people about Castres they would probably mention the rugby team, Castres Olympique, the cute center known as the “Venise of Tarn”, and the implantation of a big french pharmaceutical company: Fabre. -

Tarn (81) Bassins De Sante
JOUQUEVIEL MONTIRAT LE RIOLS MIRANDOL-BOURGNOUNAC SAINT-CHRISTOPHE TARN (81) SAINT-MARTIN-LAGUEPIE MONTROSIER LE RIOLS MILHARS LAPARROUQUIAL LACAPELLE-SEGALAR LE SEGUR SAINT-MICHEL-DE-VAX PAMPELONNE MOUZIEYS-PANENS TREVIEN TANUS BOURNAZEL ALMAYRAC ROUSSAYROLLESMARNAVES TREBAN PENNE LABARTHE-BLEYS SAINT-MARCEL-CAMPES SAINTE-GEMME MONTAURIOL LEDAS-ET-PENTHIES LES CABANNES SALLES MONESTIES MOULARES VAOUR TONNAC CORDES-SUR-CIEL LACAPELLE-PINET BASSINS DE SANTE VINDRAC-ALAYRAC SAINT-BENOIT-DE-CARMAUX SAINT-JEAN-DE-MARCEL ITZAC CARMAUX ALBI LIVERS-CAZELLES COMBEFA AMARENS VIRAC CRESPIN PADIES ROSIERES LOUBERS FAUSSERGUES CAMPAGNAC SOUEL MILHAVET LABASTIDE-GABAUSSEBLAYE-LES-MINES SAINT-BEAUZILE FRAUSSEILLES VALENCE-D'ALBIGEOIS ALOS VALDERIES DONNAZAC NOAILLES LE DOURN TAIX ANDILLAC VILLENEUVE-SUR-VERE ANDOUQUE SAINT-MICHEL-LABADIE LARROQUE SAINTE-CECILE-DU-CAYROU MAILHOC LE GARRIC VIEUX SAINT-JULIEN-GAULENE LE VERDIER SAUSSENAC CAHUZAC-SUR-VERE CESTAYROLS CAGNAC-LES-MINES PUYCELCI CASTELNAU-DE-MONTMIRAL ASSAC CADIX CASTANET FRAISSINES LA SAUZIERE-SAINT-JEAN SAINTE-CROIX SAINT-CIRGUE MONTELS LESCURE-D'ALBIGEOISARTHES SERENAC FAYSSAC CRESPINET MONTDURAUSSE BROZE COURRIS TREBAS SENOUILLAC BERNAC SAINT-GREGOIRE ³ CASTELNAU-DE-LEVIS SAINT-JUERY SAINT-URCISSE LABASTIDE-DE-LEVIS ALBI SAINT-ANDRE CUNAC MARSAL AMBIALET SALVAGNAC TERSSAC GAILLAC RIVIERES MONTGAILLARD MARSSAC-SUR-TARN LE SEQUESTRE CAMBON CURVALLE LE FRAYSSE BELLEGARDE BEAUVAIS-SUR-TESCOU LISLE-SUR-TARN LAGRAVE VILLEFRANCHE-D'ALBIGEOIS BRENS CARLUS PUYGOUZON FLORENTIN ROUFFIAC SALIES TAURIAC -

TARN RÉSERVATION TOURISME DAY at the HEART of the TARN Castres and Albi… Monday 04 July 2016
TARN RÉSERVATION TOURISME DAY AT THE HEART OF THE TARN Castres and Albi… Monday 04 July 2016 10h00 : Welcome in the tourism bus’s parking lot. Welcome by your tour. Guided walk visit of the historic centre of the city : The bishopric and the garden designed by Le Nôtre, the old houses on the Agout river, Jean-Jaurès square, the facades of the 17th century mansions,… Lunch in a restaurant in the historic center of the city.. Sample menu : Kir de bienvenue et feuilletés Muffin de rouget et sa sauce cocktail Suprême de pintade, jus aux morilles Tarte aux poires sauce à l’orange Vin rouge OU rosé - café In the afternoon, departure for ALbi. The Episcopal City was classified World Heritage by the UNESCO in August 2010. "Crucible of brick", "fortress of faith", "Italian city", Albi has stimulated the imagination of those seeking an epithet to describe its appeal. With the trilogy of the Sainte Cécile cathedral, the Palais Berbie (which houses the Toulouse-Lautrec museum) and the “pont vieux”, not forgetting the charm of the old streets. Bright red in the morning sunlight, sombre red at dusk, deserted in the heat of the afternoon. Half-timbered corbelled houses, narrow passages, cobbled streets... medieval buildings with the colours of the south. Stroll around, follow your instincts; the slightest opening may reveal hidden treasures: the Hotel Reynes with its extraordinary loggia, built by a rich pastel merchant in 1530, the cloisters of Saint Salvy (13th century) with their triangular lawn and twinned columns... Beyond the obvious and the well-known, Albi likes to surprise its visitors, particularly rewarding for those who are not in a hurry. -

37 % Des Ménages Auraient Plus De 65 Ans Dans L'aire Urbaine De Castres
AIRE URBAINE DE CASTRES 37 % des ménages auraient plus de 65 ans dans l’aire urbaine de Castres En 2009, 67 400 personnes vivent dans l’aire urbaine de Castres, ce qui représente 18 % de la population du Tarn. La quasi-totalité vit au sein de ménages, unité désignant l’ensemble des personnes qui partagent la même résidence principale. L’aire urbaine de Castres compte 29 350 ménages en 2009 et ils seraient 34 500 en 2030, si les tendances démographiques récentes ainsi que les comportements de cohabitation se maintenaient. Le nombre de ménages progresserait de 17,4 %, soit en moyenne de 0,8 % par an. La croissance serait moins importante que celle de l’ensemble du Tarn où, sous les mêmes hypothèses, le nombre de ménages augmenterait de 24,6 % entre 2009 et 2030 (+ 1,1 % par an). Les ménages de l’aire urbaine de Castres ne représenteraient plus que 17 % des ménages tarnais en 2030, alors qu’ils en regroupent 18 % en 2009. La croissance du nombre de ménages de l’aire urbaine de Castres serait un peu moins importante qu’entre 1990 et 2009. Durant cette période, le nombre de ménages a progressé de 1,0 % par an, rythme inférieur à celui observé dans l’ensemble du Tarn (+ 1,3 %). La croissance démographique serait bien moins soutenue Le poids des couples resterait toujours important que dans le Tarn La diminution de la part des couples au profit des personnes L’évolution démographique serait le principal déterminant de la seules ne serait pas seulement due au vieillissement de la popula- croissance du nombre de ménages. -

Lisle-Sur-Tarn by the Duke of Través De Los Dibujos Barrocos Y Escenas Mitológicas Que Tanto Le Gustaban
3 LE SQUARE RAYMOND LAFAGE jouxtant l’église Notre Dame de la Bastides et Jonquière est dédié à l’artiste peintre Raymond Lafage. Sa brève carrière montre tout son caractère épicurien, à travers les dessins baroques et les scènes mythologiques qu’il affectionnait. Vignoble du Gaillac The area next to the church is dedicated to Raymond Lafage, his brief career shows his epicurean character though his baroques drawings and mythological scenes which he produced. La plaza adyacente a la iglesia de Notre Dame de la Jonquière está dedicada Vue des vestiges du port a Raymond Lafage, cuya breve carrera muestra todo su carácter epicúreo, a The Languedoc chambers were installed in Lisle-sur-Tarn by the Duke of través de los dibujos barrocos y escenas mitológicas que tanto le gustaban. Montmorency and served just till 1585, to judge the religions affairs between the Catholics and Protestants. King Henry the fourth re-established by verdict of Edict 4 L’ÉGLISE NOTRE DAME DE LA JONQUIÈRE conserve de sa construction primitive un portail latéral de style roman. Sa tour-porche datant of Nantes and it became the «Chambers of Edit». The Edict building also housed the des XIVe et XVe siècles s’achève en clocher à 2 étages. Son style est souvent port captian. appelé gothique méridional ou «Tolosano-Albigeois» un riche mobilier intérieur, El Duque de Montmorency estableció la “Chambre du Languedoc” (Cámara de provenant en partie de l’ancienne église des augustins, orne les chapelles. Languedoc) en Lisle sur Tarn en 1579, donde permanecería hasta 1585 para The Church «Notre-Dame of Jonquiere» has retained a lynch gate of roman style juzgar casos entre católicos y protestantes.