Click This Link
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

BOY SCOUTS of AMERICA and DELAWARE BSA, LLC,1 Debtors
Case 20-10343-LSS Doc 1295 Filed 09/09/20 Page 1 of 2 IN THE UNITED STATES BANKRUPTCY COURT FOR THE DISTRICT OF DELAWARE Chapter 11 In re: Case No. 20-10343 (LSS) BOY SCOUTS OF AMERICA AND (Jointly Administered) DELAWARE BSA, LLC,1 Debtors. Ref. Docket Nos. 1258 NOTICE OF FILING OF CORRECTED DECLARATION OF DISINTERESTEDNESS BY JUSTIN H. RUCKI OF RUCKI FEE REVIEW, LLC PLEASE TAKE NOTICE that, on September 4, 2020, the Debtors filed the Certification of Counsel Regarding Appointment of Fee Examiner (D.I. 1258) (the “Fee Examiner COC”). PLEASE TAKE FURTHE NOTICE that attached as Exhibit A to the Fee Examiner COC was a proposed order (the “Proposed Order”) appointing Rucki Fee Review, LLC as the Fee Examiner in these chapter 11 cases. PLEASE TAKE FURTHER NOTICE that attached as Exhibit 1 to the Proposed Order was the Declaration of Disinterestedness by Justin H. Rucki of Rucki Fee Review, LLC (the “Rucki Declaration”). PLEASE TAKE FURTHER NOTICE that the Debtors inadvertently omitted the Potential Parties in Interest List from the Rucki Declaration. PLEASE TAKE FURTHER NOTICE that attached hereto as Exhibit 1 is a corrected Rucki Declaration with the inclusion of Potential Parties in Interest List. [Remainder of Page Intentionally Left Blank] 1 The Debtors in these chapter 11 cases, together with the last four digits of each Debtor’s federal tax identification number, are as follows: Boy Scouts of America (6300) and Delaware BSA, LLC (4311). The Debtors’ mailing address is 1325 West Walnut Hill Lane, Irving, Texas 75038. Case 20-10343-LSS Doc 1295 Filed 09/09/20 Page 2 of 2 Dated: September 9, 2020 MORRIS, NICHOLS, ARSHT & TUNNELL LLP Wilmington, Delaware /s/ Eric W. -

Reaching for the Stars When You Participate in the 2007 Csecc You Become a Star!
Donor Resource Guide Reaching for the Stars when you participate in the 2007 csecc you become a star! california state employees charitable campaign www.csecc.org “Every contribution is a step toward making someone’s life a little bit brighter. You have the chance to become someone’s star when you join Maria and me during the 2007 California State Employees Charitable Campaign and donate to your favorite charity.” Arnold Schwarzenegger Governor of California 2007 California State Employees Charitable Campaign Chair Fifty Years California State Employees Charitable Campaign 1957 Chair’sChair’s MessageMessage Dear Fellow State Employees, I am excited and honored to be chairman of the 2007 California State Employees Charitable Campaign. We raised more than $7.7 million for thousands of fantastic charities last year, and all of our volunteers and donors did a wonderful job. This year, I’m looking forward to an even bigger total. California has always been a leader in generosity and compassion, and now is our chance to show our support for all the charities that need our help. By fi lling out a simple form, we can give to worthwhile causes that do great work in our communities and around the world. When I came to America many years ago, I was impressed with the kindness of the people here in California. This campaign has been a huge success since 1957, so please join me as we continue to celebrate our 50-year tradition of making a difference. Arnold Schwarzenegger Governor 2007 CSECC Chair 2 TableTable ofof ContentsContents United Way Organizations (PCFDs) ............. -

Destination Montana BSA Camping Guide 2019
DESTINATION MONTANA P ING GUI CAM DE BIG SKY COUNTRY UNMATCHED SCOUTING SPIRIT ENDLESS POSSIBILITIES WWW.MONTANABSA.ORG BROUGHT TO YOU BY THE ORDER OF THE ARROW APOXKY AIO LODGE DESTINATION MONTANA It has been said that you cannot have Scouting without the Montana's pristine waters of Flathead Lake boast a 64-acre “outing.” In Montana, we take the “outing” part seriously. aquatics paradise known as Melita Island. Both resident There is no better place to access all that Mother Nature camps offer unique access to the wonders of the great offers than at a Montana Council summer camp. Oppor- outdoors. Near the Anaconda-Pintler Wilderness is Camp tunities abound to develop new skills or master previously Arcola, a perfect place for those who have mastered the learned skills in a controlled and supervised environment. basics and are looking for more rugged, independent Whether you’re a first-time camper or a seasoned outdoor adventure. On the eastern edge of the Flathead Valley veteran, our camps have something for you. near Bigfork is Grizzly Base, which serves as our training base and offers a week of summer camp adventures for The Boy Scouts of America, Montana Council is proud to Webelos Scouts. The Montana Outdoor High Adventure offer four camp locations and one high-adventure base in Base (MOHAB) offers a second-to-none atmosphere in the state. Our traditional summer camps are two of the a setting linked to the Bob Marshall Wilderness. Live out- “Best Camps in the West,”—Scouting magazine. Nestled doors for a week in the mountains and experience all that between the peaks of the Moccasin Mountains in the heart Montana has to offer! of central Montana lies K-M Scout Ranch, while western For more information, promotional videos, or to book your summer adventure, please visit www.montanabsa.org/camping or call 406.761.6000. -

April 2008 Inside This Issue
APRIL 2008 SMOKE SIGNALS Mt. Diablo Silverado Council Issue # 2008/04 Boy Scouts of America MDSC WELCOMES NEW COUNCIL PRESIDENT INSIDE Tom Edwards was named as the Council President of the Mt. Diablo THIS ISSUE Silverado Council at the Annual Business Meeting held on February 11th. Tom is currently Chairman of the Board of Wentworth, Hauser ENTER OUR Important Dates 2 and Violich and resides in Lafayette with his wife, Libby. Tom “VENTURING 10TH previously chaired the council’s audit committee and most recently ANNIVERSARY” Memorials/Tributes 2 the updating of the Strategic Plan. Council officers elected are: PHOTO CONTEST What images do you think best Training 3 President Tom Edwards reflect the essence of Venturing? Aklan 7 Commissioner Richard Utter Capture them with your camera Treasurer William Collett and then enter your favorite Black Diamond 8 Legal Service Rich McNeely photographs in the “Venturing 10th Chief Solano 9 Vice President of Finance Lynn Cannady Anniversary” photo contest. Vice President Administration Anne O’Neal Herms 10 The contest is open to all Vice President Membership/ Relationships William Dorband Iron Horse 11 Vice President Operations John April registered youth members of the Vice President Program Steve Phillips Venturing program. Photos will Lake 12 Immediate Past President Robert Carns be judged in four categories: Marsh Creek 13 1. Wildlife 2. People Meridian 14 3. The Spirit of Venturing Muir 15 4. Spirit of Patriotism LAS AGUILAS DE DIABLO TO HOST Napa Valley 16 Our judges will be looking for ANNUAL EAGLE DINNER MAY 7, 2008 Silver Gate 17 Bob Slyker, president of Las Aguilas de Diablo has announced that the photographs that best exhibit preparations are underway for the annual Eagle Dinner to be held creativity, originality, and visual Ut-In Selica Lodge 18 May 7, 2008. -

Epp SF Booklet 2004 9/4/04 5:39 AM Page A1 Epp SF Booklet 2004 9/4/04 5:39 AM Page A2
epp_SF_Booklet_2004 9/4/04 5:39 AM Page a1 epp_SF_Booklet_2004 9/4/04 5:39 AM Page a2 Message From The Chair Dear fellow Federal Employees and Military Personnel, This year’s theme for the Combined Federal Campaign (CFC), “The Power of Giving,” underscores the important role you can play by supporting our charitable organizations. The need is so great right now. More than ever, nonprofit agencies depend upon us, not just for the services we provide to the public, but for our generosity through the local CFC. Our goal is to contact 100% of Federal employees and Military personnel in our region with this message, to motivate 35% of us to participate in the CFC, and to raise $4 million for these worthy causes. Your goal can be to make a difference in the lives of people living in your community, the State of California and even the nation: please consider donating one hour of pay per month. You may have heard that some nonprofits, including the American Civil Liberties Union, the Sierra Club and Amnesty International USA, have removed themselves from the CFC. If you wish to support them, you can do so directly. However, I encourage you to also continue your support for the many deserving organizations that benefit from CFC. Please join us this year and affirm your power to give something back to our community. Sincerely, H. Joan Ehrlich U.S. Equal Employment Opportunity Commission Chair, Combined Federal Campaign ★ a2 epp_SF_Booklet_2004 9/4/04 5:39 AM Page 1 Table of Contents DONOR APPRECIATION & LEADERSHIP GIFTS...........2 2003 EAGLE CLUB -
Do No R Resource G Uide
H donor resource guide H H Table of Contents H United Way Organizations (PCFDs) .....................8 Asian Pacific Community Fund of Southern California ......... 34 Arrowhead United Way ........................................................ 8 Bay Area Black United Fund, Inc. ....................................... 34 United Way of the Bay Area ................................................. 8 Cancer Cure of America- Care, Understand, Research United Way of Butte and Glenn Counties ............................. 11 & End ............................................................................35 United Way California Capital Region .................................. 11 Children’s Charitable Alliance ............................................35 Central County United Way .................................................14 Children’s Charities of America ..........................................35 United Way of the Desert ....................................................14 Children’s Medical Charities of America ............................. 36 Desert Communities United Way.........................................14 Christian Charities USA ......................................................37 United Way of the East Valley .............................................14 Christian Community Charities ...........................................37 United Way of Fresno County ..............................................15 Combined Health Appeal of Central California .....................37 United Way of Greater Los Angeles .....................................16 -

Guide to Council Camps National Parks California
GUIDE TO COUNCIL CAMPS NATIONAL PARKS CALIFORNIA PARKS ORANGE COUNTY PARKS SAN BERNARDINO PARKS 1 A Few Basics. As all American, I will do my best to . Be clean in my outdoor manners, Be careful with fire, Be considerate ill the outdoors, and Be conservation minded. -The Outdoor Code, The Boy Scout Handbook, 1993 Edition, Page 55 The Outdoor Code is perhaps the most well-known and shortest statement of BSA outdoor policy. It can be expanded into six points that cover how your unit can have a 'low-impact' on your weekend car camping and backpacking outings: Pretrip Plans Wear Scout uniforms or other clothes that will blend into the surroundings. When picking camping equipment, such as tents, try to abide by the same rule. Pack food in containers that you'll carry home at the end of a trip. Take along (and use) trash bags. Plan to have 12 or fewer people staying in an individual campsite. Pick areas that are suited to the type of activity that you are planning. Using Trails Stay on the trail. Don't cut across switchbacks. Campsites Choose sites free of fragile plants. Camp out of sight of trails, streams, and lakes. Don't dig trenches around your tents or make any other unneeded holes. Fires Build fires only where appropriate and allowed. Try to get by with just propane stoves. Use existing fire rings instead of making new ones. Bring your own wood supply with you whenever possible. Open gathering may be prohibited. If you gather firewood, make sure you only burn small wood gathered from the ground. -
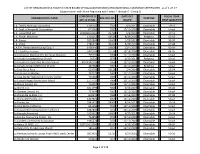
(BOE) Organizational Clearance Certificates- As of 1-27-17
LIST OF ORGANIZATIONS HOLDING STATE BOARD OF EQUALIZATION (BOE) ORGANIZATIONAL CLEARANCE CERTIFICATES - as of 1-27-17 (Organizations with Name Beginning with Letters L through R - Group 3) CORPORATE D DATE OCC FISCAL YEAR ORGANIZATION NAME BOE OCC NO. PURPOSE OR LLC ID NO. ISSUED FIRST QUALIFIED L.A. Family Housing Corporation 1205147 7561 6/1/2015 Charitable 10-11 L.A. Goal, a Nonprofit Corporation 674369 7050 12/11/2003 Charitable Unavl L.A. Lucas MGP LLC 200914010165 21796 6/9/2010 Charitable 10-11 L.A. Prayer Mountain 1318153 18516 8/19/2005 Religious 02-03 L.A. Shares 1852968 23407 1/23/2013 Charitable 96-97 L.A. Voice 2186515 20462 5/26/2010 Charitable 07-08 L.A.F.H. Permanent Housing Corp. I 1406440 19668 10/4/2007 Charitable 03-04 L.C. Hotchkiss Terrace 2476704 17574 10/19/2004 Charitable 04-05 La Asociacion Nacional Pro Personas Mayores 735192 7054 12/11/2003 Charitable Unavl La Canada Congregational Church 26628 2873 6/13/2011 Religious 09-10 La Canada Co-Operative Nursery School ASSOCIATION 7056 12/11/2003 Charitable Unavl La Canada United Methodist Church 487588 7057 12/11/2003 Religious Unavl La Casa De La Raza 623708 22128 2/4/2014 Charitable 03-04 La Casa de Las Madres 767175 7061 12/11/2003 Charitable Unavl La Casa De San Gabriel Community Center 764368 7063 12/11/2003 Charitable Unavl La Casita Bilingue Montessori School 1517735 7064 12/11/2003 Charitable Unavl La Cheim School, Inc. 724007 7066 12/11/2003 Charitable Unavl La Cheim, Inc. -

February 2021
Council Management Support Boy Scouts of America Unit Contacts for Katahdin Area Council #216 - Bangor, ME (Area 1) Through Month of February, 2021 Dist. Unit Commissioners Unit Contacts Recorded in Commissioner Tools *Units Percent Contacted Contacted No. District Name Units Comm Ratio Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total 01 Hancock 3 2 5.0 2 1 3 0.0% 04 Washington 4 999.0 0.0% 05 North Star 8 1 17.0 0.0% 06 Penobscot Valley 16 4 7.0 5 5 0.0% 07 Penquis 5 2 6.0 0.0% 09 Waldo 7 999.0 18 18 0.0% 216 Council Totals** 43 9 4.8 2 24 26 0.0% * The Units Contacted column reflects the number of units that have had sufficient contacts recorded year-to-date. In order to show progress, a unit is counted if it has been contacted at least once by January/February, two times by March/April, three times by May/June, four times by July/August, five times by September/October and six times by November/December. For example, a unit that was not contacted until March will not be counted in January or February, but will count in March, if it receives two contacts that month. At the end of the year a unit needs at least six total contacts to be counted. Contacts are counted by the date they are entered into Commissioner Tools, not by the actual date of the contact or visit. Posts are included in 2017 and beyond; however, Exploring only districts may not be included. -
BAS May 2010.Indd
2010 Vol 2 May-July 2010 Wente Scout In this issue: New Cub Scout Reservation’s Focus on Finance - page 2 Program and Memorial Weekend Whitney M. Young, Materials Family Vacation Camp Jr. Awards Dinner - page 3 Information Where can you get camping, hiking, boating, swimming, Friends of Scouting Victory -- see page 17-18 horseback riding, campfi res, ice Celebration cream, great food and usually, great - page 3 weather, all for little more than it costs to stay home? At Family 100th Anniver- th sary Jamboree and 100 Anniversary of Scouting Vacation Camp of course! Camp Commemorative 2010 Eagle Scout is a great place to let your kids have Patches - page 5-6 fun without worrying about them 100th Recognition Dinner tracking in dirt or dripping water. Anniversary Honoring the Rick K. Pickering They can shoot archery, BB guns, Awards - page 6 rifl e, make handicrafts, swim, fi sh Eagle Scout Class (bring your fi shing gear!), go for World Jamboree Sweden - page 7 Wednesday June 2, 2010 hikes, ride horses*, and even take Hilton Oakland Airport a drive to many of the local scenic Membership One Hegenberger Road, Oakland landmarks. - page 8 Memorial Weekend is a Rick K. Pickering, Chief Executive great place to be. It’s inexpensive. From Your Registrar - page 9 Offi cer, Alameda County Agricultural It’s fun! That adds up to a fabulous Fair Association will be receiving the vacation weekend. You can cook Distinguished Eagle Scout Award at the Cub Scout your own food or for a small amount Adventures th San Francisco Bay Area Council’s 100 choose camp meals which include - page 10 Anniversary of Scouting – Eagle Scout breakfast, lunch and dinner on Recognition Dinner. -

Certified Nonprofits
2017 CERTIFIED NONPROFITS 1957 • • 2017 Every Day. All Year. 2017 CERTIFIED NONPROFITS The following is a list of all the nonprofit organizations represented in the 2017 Our Promise campaign that are certified by the Department of Justice. WHAT'S INCLUDED IN EACH LISTING: When filling out your pledge Nonprofit Code # form, please use this nonprofit Nonprofit Name code in Step 3. Alternate Name (if any) Nonprofit name(s) TaxID# and general information. Mailing Address City, State, Zip You can click on any website to www.website.org access it directly from the PDF. If you do not see your nonprofit listed here, you may still give to them: simply provide their information in the write-in section of Step 3 on the pledge form. THANK YOU FOR CARING FOR CALIFORNIA! 10389 Old Placerville Road Sacramento, CA 95827 DONOR HOTLINE (888) 863-6466 www.OurPromiseCA.org 2 28880 24866 11761 A 10,000 Degrees A Community Of Friends ABS-CBN Foundation Inc. TaxID# 95-3667812 TaxID# 95-4203106 ABS-CBN Foundation International B 1650 Los Gamos Drive, Suite 110 3701 Wlshre Blvd Ste 700 TaxID# 94-3292281 San Rafael, CA 94903 Los Angeles, CA 90010 2001 Junipero Serra Blvd., 2nd Floor www.10000degrees.org www.acof.org Daly, CA 95126 C www.abscbnfoundation.org 13830 887 D 1736 Family Crisis Center A Place Called Home 25567 TaxID# 95-3989251 TaxID# 95-4427291 Abused Children's Fund, Inc. E 2116 Arlington Ave., Suite 200 2830 South Central Avenue TaxID# 59-3254371 Los Angeles, CA 90018 Los Angeles, CA 90011 1535 Farmers Lane, #200 www.1736fcc.org www.apch.org Santa Rosa, CA 95405 F www.abusedchildrensfund.org 17684 13507 G 2-1-1 Orange County A Safe Place 13439 TaxID# 33-0063532 TaxID# 94-2491881 Acacia Adult Day Services H 1505 E. -

BOY SCOUTS of AMERICA and DELAWARE BSA, LLC, Debtors
Case 20-10343-LSS Doc 206 Filed 03/17/20 Page 1 of 15 IN THE UNITED STATES BANKRUPTCY COURT FOR THE DISTRICT OF DELAWARE In re: Chapter 11 BOY SCOUTS OF AMERICA AND Case No. 20-10343 (LSS) DELAWARE BSA, LLC,1 (Jointly Administered) Debtors. Hearing Date: April 15, 2020 at 10:00 a.m. (ET) Objection Deadline: March 31, 2020 at 4:00 p.m. (ET) DEBTORS’ APPLICATION FOR ENTRY OF AN ORDER AUTHORIZING THE RETENTION AND EMPLOYMENT OF ALVAREZ & MARSAL NORTH AMERICA, LLC AS FINANCIAL ADVISOR FOR THE DEBTORS AND DEBTORS IN POSSESSION, NUNC PRO TUNC TO THE PETITION DATE The Boy Scouts of America (the “BSA”) and Delaware BSA, LLC, the non-profit corporations that are debtors and debtors in possession in the above-captioned chapter 11 cases (together, the “Debtors”), submit this application (this “Application”), pursuant to section 327(a) of title 11 of the United States Code, 11 U.S.C. §§ 101–1532 (the “Bankruptcy Code”), rules 2014 and 2016 of the Federal Rules of Bankruptcy Procedure (the “Bankruptcy Rules”), and rules 2014-1 and 2016-2 of the Local Rules of Bankruptcy Practice and Procedure of the United States Bankruptcy Court for the District of Delaware (the “Local Rules”), for entry of an order, substantially in the form attached hereto as Exhibit A (the “Proposed Order”), (i) authorizing the Debtors to retain and employ Alvarez & Marsal North America, LLC, together with employees of its affiliates (all of which are wholly-owned by its parent company and employees), its wholly owned subsidiaries, and independent contractors (collectively, “A&M”), as their financial advisor nunc pro tunc to February 18, 2020 (the “Petition Date”) pursuant to the terms of the 1 The Debtors in these chapter 11 cases, together with the last four digits of each Debtor’s federal tax identification number, are as follows: Boy Scouts of America (6300) and Delaware BSA, LLC (4311).