Antrochoanal Polyp
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Foley Catheter Action in the Nasopharynx a Cadaveric Study
ORIGINAL ARTICLE Foley Catheter Action in the Nasopharynx A Cadaveric Study Wai Chung Lee, FRCS(ORL); Peter Ka Ming Ku, FRCSEd; Charles Andrew van Hasselt, FRCS Objectives: To determine the action of the Foley cath- eral side at appropriate inflation volumes in 17 (85%) of eter in the posterior nasal cavity in relation to balloon 20 nasal fossae. Complete sealing between volumes of 12 volume, and to deduce its implications in the treatment and 15 mL was achieved in 13 fossae (65%), between 11 of posterior epistaxis. and 15 mL in 10 nasal fossae (50%), and between 5 and 15 mL in 3 nasal fossae (15%). Failure to seal at any vol- Design: Human cadaveric study. ume occurred in 3 nasal fossae (15%). Bimodal seal (ie, complete seal at high [15 mL] and low volumes [4-7 mL], Materials: Twenty nasal fossae of 10 adult cadavers. but leakage in intermediate volumes) occurred in 3 na- sal fossae (15%). The balloon remained in the nasopha- Interventions: A Foley catheter (size 14) was inserted rynx under traction and did not slip past the choanal rim into the nasopharynx via each nostril. The catheter bal- to encroach on the middle and inferior turbinates until loon was inflated to its recommended maximum vol- the balloon volume was reduced to between 4 and 7 mL. ume with 15 mL of water. Firm traction was applied to The balloon slid out of the nose at a volume of 5 mL or the catheter. Colored liquid was instilled into the ipsi- less. The inflation volumes ranging from 8 to 12 mL were lateral aspect of the nasal cavity, and liquid leakage into statistically more effective in sealing the choana than lower the contralateral side was monitored using a nasoendo- volumes (4-7 mL) (P,.002, x2 test). -

Evolution of the Nasal Structure in the Lower Tetrapods
AM. ZOOLOCIST, 7:397-413 (1967). Evolution of the Nasal Structure in the Lower Tetrapods THOMAS S. PARSONS Department of Zoology, University of Toronto, Toronto, Ontario, Canada SYNOPSIS. The gross structure of the nasal cavities and the distribution of the various types of epithelium lining them are described briefly; each living order of amphibians and reptiles possesses a characteristic and distinctive pattern. In most groups there are two sensory areas, one lined by olfactory epithelium with nerve libers leading to the main olfactory bulb and the other by vomeronasal epithelium Downloaded from https://academic.oup.com/icb/article/7/3/397/244929 by guest on 04 October 2021 with fibers to the accessory bulb. All amniotes except turtles have the vomeronasal epithelium in a ventromedial outpocketing of the nose, the Jacobson's organ, and have one or more conchae projecting into the nasal cavity from the lateral wall. Although urodeles and turtles possess the simplest nasal structure, it is not possible to show that they are primitive or to define a basic pattern for either amphibians or reptiles; all the living orders are specialized and the nasal anatomy of extinct orders is unknown. Thus it is impossible, at present, to give a convincing picture of the course of nasal evolution in the lower tetrapods. Despite the rather optimistic title of this (1948, squamates), Stebbins (1948, squa- paper, I shall, unfortunately, be able to do mates), Bellairs and Boyd (1950, squa- iittle more than make a few guesses about mates), and Parsons (1959a, reptiles). Most the evolution of the nose. I can and will of the following descriptions are based on mention briefly the major features of the these works, although others, specifically nasal anatomy of the living orders of cited in various places, were also used. -

Surgical Anatomy of the Paranasal Sinus M
13674_C01.qxd 7/28/04 2:14 PM Page 1 1 Surgical Anatomy of the Paranasal Sinus M. PAIS CLEMENTE The paranasal sinus region is one of the most complex This chapter is divided into three sections: develop- areas of the human body and is consequently very diffi- mental anatomy, macroscopic anatomy, and endoscopic cult to study. The surgical anatomy of the nose and anatomy. A basic understanding of the embryogenesis of paranasal sinuses is published with great detail in most the nose and the paranasal sinuses facilitates compre- standard textbooks, but it is the purpose of this chapter hension of the complex and variable adult anatomy. In to describe those structures in a very clear and systematic addition, this comprehension is quite useful for an accu- presentation focused for the endoscopic sinus surgeon. rate evaluation of the various potential pathologies and A thorough knowledge of all anatomical structures their managements. Macroscopic description of the and variations combined with cadaveric dissections using nose and paranasal sinuses is presented through a dis- paranasal blocks is of utmost importance to perform cussion of the important structures of this complicated proper sinus surgery and to avoid complications. The region. A correlation with intricate endoscopic topo- complications seen with this surgery are commonly due graphical anatomy is discussed for a clear understanding to nonfamiliarity with the anatomical landmarks of the of the nasal cavity and its relationship to adjoining si- paranasal sinus during surgical dissection, which is con- nuses and danger areas. A three-dimensional anatomy is sequently performed beyond the safe limits of the sinus. -

Nasal Cavity (F3)
THE NASAL CAVITY Created by Michael Guo with help from The amazing structures and spaces in our nasal cavity allow us to filter the air Michael Markos that comes through our nostrils, buffer pressure changes in the environment, create resonance in our voices, smell our surroundings, and protect against Designed by Erin Lee foreign particles that may cause disease. The nasal cavity can be thought of as a box, with important anatomical landmarks that act as borders: NASAL CAVITY top front back bottom Top Front cranium orbits Kiesselbach area septum nostrils Air comes in through the nostrils, which are a very At the roof of this box is the floor of our small portion of the nasal cavity. A wall of cartilage cranium, a bony box where the brain resides. that separates the nasal cavity into two sides, each The top of the nasal cavity is enclosed on both fed by one nostril. The septum provides flexibility for sides by your orbits, which contain your eyeballs your nose and may break during trauma. A deviated and the muscles, nerves and blood vessels septum, when the septum to diverges away from the essential for your vision. Complications of the middle, can result in problems in breathing, facial nasal cavity in direct contact with these pain and nose bleeds. There are many tiny blood structures may affect your vision and brain, vessels in this space, which cause bleeding if such as double vision, headache, and altered damaged (ie. during nose picking). A densely-packed mental state. region of blood vessels, known as the Kiesselbach area, is a common origin of nose-bleeds. -

Lungfishes, Tetrapods, Paleontology, and Plesiomorphy
LUNGFISHES, TETRAPODS, PALEONTOLOGY, AND PLESIOMORPHY DONN E. ROSEN Curator, Department of Ichthyology American Museum of Natural History Adjunct Professor, City University of New York PETER L. FOREY Principal Scientific Officer, Department of Palaeontology British Museum (Natural History) BRIAN G. GARDINER Reader in Zoology, SirJohn Atkins Laboratories Queen Elizabeth College, London COLIN PATTERSON Research Associate, Department of Ichthyology American Museum of Natural History Senior Principal Scientyifc Officer, Department of Palaeontology British Museum (Natural History) BULLETIN OF THE AMERICAN MUSEUM OF NATURAL HISTORY VOLUME 167: ARTICLE 4 NEW YORK: 1981 BULLETIN OF THE AMERICAN MUSEUM OF NATURAL HISTORY Volume 167, article 4, pages 159-276, figures 1-62, tables 1,2 Issued February 26, 1981 Price: $6.80 a copy ISSN 0003-0090 Copyright © American Museum of Natural History 1981 CONTENTS Abstract ........................................ 163 Introduction ...................... ........................ 163 Historical Survey ...................... ........................ 166 Choana, Nostrils, and Snout .............................................. 178 (A) Initial Comparisons and Inferences .......................................... 178 (B) Nasal Capsule ............. ................................. 182 (C) Choana and Nostril in Dipnoans ............................................ 184 (D) Choana and Nostril in Rhipidistians ........................................ 187 (E) Choana and Nostril in Tetrapods .......................................... -
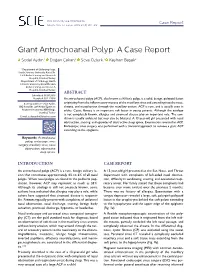
Giant Antrochoanal Polyp: a Case Report
DOI: 10.14744/scie.2018.98698 Case Report South. Clin. Ist. Euras. 2018;29(4):310-312 Giant Antrochoanal Polyp: A Case Report 1 1 1 2 Sedat Aydın, Doğan Çakan, Seva Öztürk, Kayhan Başak 1 Department of Otolaryngology, Heath Sciences University Kartal Dr. Lütfi Kırdar Training and Research Hospital, İstanbul, Turkey 2Department of Pathology, Heath Sciences University Kartal Dr. Lütfi Kırdar Training and Research Hospital, İstanbul, Turkey ABSTRACT Submitted: 01.07.2018 Accepted: 05.11.2018 An antrochoanal polyp (ACP), also known as Killian’s polyp, is a solid, benign, polypoid lesion Correspondence: Sedat Aydın, originating from the inflammatory mucosa of the maxillary sinus and extending into the nose, SBÜ Kartal Dr. Lütfi Kırdar Eğitim ve choana, and nasopharynx through the maxillary ostium. ACP is rare, and is usually seen in Araştırma Hastanesi, KBB Kliniği, adults. Cystic fibrosis is an important risk factor in young patients. Although the etiology İstanbul, Turkey is not completely known, allergies and sinonasal disease play an important role. The con- E-mail: [email protected] dition is usually unilateral but may also be bilateral. A 13-year-old girl presented with nasal obstruction, snoring, and episodes of obstructive sleep apnea. Examination revealed an ACP. Endoscopic sinus surgery was performed with a transoral approach to remove a giant ACP extending to the epiglottis. Keywords: Antrochoanal polyp; endoscopic sinus surgery; maxillary sinus; nasal obstruction; obstructive sleep apnea. INTRODUCTION CASE REPORT An antrochoanal polyp (ACP) is a rare, benign solitary le- A 13-year-old girl presented at the Ear, Nose, and Throat sion that constitutes approximately 4% to 6% of all nasal department with complaints of left-sided nasal obstruc- polyps. -
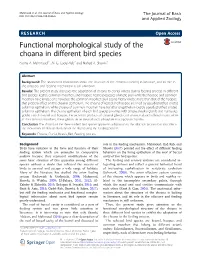
Functional Morphological Study of the Choana in Different Bird Species Fatma A
Mahmoud et al. The Journal of Basic and Applied Zoology (2018)79:11 The Journal of Basic DOI 10.1186/s41936-018-0026-6 and Applied Zoology RESEARCH Open Access Functional morphological study of the choana in different bird species Fatma A. Mahmoud1*, Ali G. Gadel-Rab2 and Nahed A. Shawki1 Abstract Background: The anatomical information about the structure of the choana is lacking in literature, and its role in the olfactory and feeding mechanism is still unknown Results: The present study discusses the adaptation of choana to cranial kinesis during feeding process in different bird species: kestrel, common moorhen, and hoopoe. Kestrel possesses a kinetic skull while the hoopoe and common moorhen have kinetic one; however, the common moorhen skull seems highly kinetic more than that of the hoopoe that properly effect on the choanal epithelium. The choana of kestrel and hoopoe are lined by pseudostratified ciliated columnar epithelium, while choana of common moorhen have transitional epithelium beside pseudostratified ciliated columnar epithelium. The choana epithelium of each bird species provides with simple alveolar glands and numerous goblet cells. In kestrel and hoopoe, the secretion products of choanal glands contain neutral and sulfated mucin, while in the common moorhen, these glands secret neutral and carboxylate mucopolysaccharides. Conclusion: The choana of the three studied bird species apparents adaptationtotheolfactionprocessbutalsoaffects the movement of skeletal elements of the skull during the feeding process Keywords: Choana, Cranial, Kinesis, Bird, Feeding process Background role in the feeding mechanism. Mahmoud, Gad-Rab, and Birds have variation in the form and function of their Shawki (2017) pointed out the effect of different feeding feeding system which are amenable to comparative behaviors on the lining epithelium of the roof of buccal analysis because they represent modifications of the cavity of two bird species. -

Inferior Concha Bullosa Communicating Into the Maxillary Sinus: Case Report
Central Annals of Otolaryngology and Rhinology Case Report *Corresponding author Murat Sereflican, Department of Otorhinolaryngology, AbantIzzet Baysal University, Faculty of Medicine, Inferior Concha Bullosa Golkoy, Turkey, Tel: 90-3742534656–3347; Fax: 90- 3742534559; Email: Communicating into the Maxillary Submitted: 08 February 2016 Accepted: 07 March 2016 Sinus: Case Report Published: 08 March 2016 ISSN: 2379-948X Murat Şereflican1*, Sıddıka Halıcıoğlu2, Sinan Seyhan1, Veysel Copyright Yurttaş1, Yasemin Ongun Funda3 and Muharrem Dağlı1 © 2016 Şereflican et al. 1Department of Otorhinolaryngology, AbantIzzet Baysal University School of Medicine, OPEN ACCESS Turkey 2Department of Radiology, AbantIzzet Baysal University School of Medicine, Turkey Keywords 3 Department of Otorhinolaryngology, Fatma Hatun Private Hospital, Turkey • Nasal concha • Maxillary sinus Abstract • Nasal obstruction Concha bullosa or conchal pneumatization refers to the presence of an air cell within a nasal turbinate. Pneumatization is most commonly seen in the middle turbinate followed by the superior turbinate. Pneumatized inferior turbinate is rare, and most of the papers in the literature appear as case reports. In this study, a 33-year-old female patient complaining from unilateral nasal stuffiness and intermittent headache is presented. Symptomatology, diagnostic and therapeutic methods for inferior concha bullosa is discussed. In clinical practice, the pneumatization status should well be studied on the scans before sinus and turbinate surgery and inferior concha bullosa should be kept in mind. ABBREVIATIONS inferior concha pneumatization associated with the maxillary sinus. Here, we present this rare case with the review of the CT: Computerized Tomography literature. INTRODUCTION CASE PRESENTATION Inferior turbinates are important anatomical structures A 33-year-old female patient presented to our clinic with a located along the lateral nasal wall. -

B. Blasberg, Dmds Stool, Mds Oka
Choanal Atresia-A Cryptic Congenital Anomaly ‘ B. BLASBERG, D.M.D. S. STOOL, M.D. S. OKA, D.M.D. Philadelphia, Pennsylvania 19104 Introduction Choanal atresia is a cryptic congenital anomaly that may result in significant physiological and anatomical alterations of the dentofacial complex. It is a congenital obstruction of one or both posterior nares. The obstruction may be due to varying amounts of bone or soft tissue. This condition which is of major concern to the Pediatrician and Otolaryngologist has received little attention in the cranio-facial literature. Anatomy. The posterior choanae connect the nasal chamber anteriorly with the nasopharynx posteriorly. Each is a four sided opening; its height being greater than its width. The borders of each choana are as follows: medially, the vomer; inferiorly, the horizontal process of the palatine bone; laterally, the medial pterygoid plate of the sphenoid; and superiorly, the ala of the vomer articulating with the vaginal process of the pterygoid plate (7). Emsrvorocy. At about five weeks in utero, specialized ectodermal thicken- ings appear on either side of the frontal prominence. This specialized ectoderm, the nasal placodes, becomes surrounded by horseshoe shaped elevations. These elevations, called the medial and lateral nasal processes grow forward leaving the placodes to line the depressions the processes have created. These depressions are the beginning of nasal cavities and are called the nasal pits or fossae (Figure 1A). As the face continues to grow forward, the floor of the nasal fossae also becomes the roof of the oral cavity. The most anterior part of this separation grows and becomes the primitive palate. -

Nasal Cavity CT Imaging Contribution to the Diagnosis and Treatment of Choanal Atresia
medicina Article Nasal Cavity CT Imaging Contribution to the Diagnosis and Treatment of Choanal Atresia Irina Šebová 1,*, Ivana Vyrvová 1,2 and Jana Barkociová 1 1 Department of Pediatric Otorhinolaryngology, Faculty of Medicine, Comenius University and National Institute of Children’s Diseases, 83101 Bratislava, Slovakia; [email protected] (I.V.); [email protected] (J.B.) 2 Faculty of Medicine, Masaryk University, 62500 Brno, Czech Republic * Correspondence: [email protected]; Tel.: +421-903-650-978 Abstract: Background and Objectives: Choanal atresia is the most common congenital malformation of the nose. Materials and Methods: We have evaluated 24 CT images of children with choanal atresia treated at the Department of Pediatric Otorhinolaryngology FM CU and the NICD Bratislava (Slovakia). In accordance with the methodology used by Slovis et al. (1985), we have measured parameters related to anomalous development in the nasal cavity: vomer width, the width of soft atresia and the width of the air space of unilaterally developed choana. Results: In the group of 24 patients, 11 (46%) were male and 13 (54%) were female. The age of patients at the time of CT imaging varied. Associated syndromes had been manifested in 11 (46%) children, with 7 (29%) patients having CHARGE syndrome. In 13 (54%) cases it was a bone membranous type of atresia, in 8 (33%) cases a membranous type, and in 3 (13%) patients a bone type. Among the group of patients, unilateral disorder was present in 13 (54%) patients and bilateral in 11 (46%). Based on the Pearson’s correlation test, we have found in the studied group that the width of the vomer correlates with age, and the vomer is wider in bone atresia than in the membranous ones. -

Sphenochoanal Polyp: Radiological Diagnosis
CASE REPOI~T swimming. Nasal endoscopy revealed a Sphenochoanal right sided solitary polypoid mass with a slender pedicle extending from the polyp: sphenoethmoidal recess to the choana. An unenhanced CT scan of paranasal sinuses (5 x 5 mm coronal radiological scans) was performed on a GE 8800 scanner (Milwaukee, USA). A soft tis- sue polyp extending from the right diagnosis sphenoid sinus/sphenoethmoidal recess to the right choana was demonstrated. MWPak* Abstract Chronic right sphenoid sinusitis with FRCS(Ed) A sphenochoanal reactive sclerosis was seen. Inside the J Kew# polyp is seen as an sphenoid sinus there was a convex up- FFRad, (D) SA isolated soft tissue per margin to the soft tissue which in- * Division of Otorhinolaryngology, dicated the presence of either a mucous Depal1ment of Surgery, density mass that retention cyst or a polyp. The other # Depal1ment of Diagnostic Radiology and arises from the Organ Imaging, Prince ofWa/es Hosp/ta/, paranasalsinuseswere clear (Figures1-4). Chinese University of Hong Kong sphenoid sinus and The clinical and radiological findings extends to the choana indicated a sphenochoanal polyp. The on computed patient was admitted for excision un- tomograph ic scans. der general anaesthesia. Under endo- Distinction from its scopic control, the anterior wall of the more cornrnon sphenoid sinus was opened and the counterpart, polyp, together with its sphenoidal com- antrochoanal polyp ponent, was removed. No recurrence vvbich arises from the was noted two years after surgery. maxillary sinus, is essential prior to Discussion surgery. A case is A choanal polyp results from pro- presented to iII ustrate lapsed mucosa of an isolated paranasal that CT scan of sinus and accounts for 3-6% of nasal paranasal sinus plays polyps.P Characteristically, it passes an important role in through the enlarged sinus ostium and the identification of protrudes into the choana leading to the sinus of origin. -
Human Computational Fluid Dynamics: from the Nose Model to the Real Nose*
Digitale Bibliothek Braunschweig 160 Wolfgang Schröder Human Computational Fluid Dynamics: From the Nose Model to the Real Nose* WOLFGANG SCHRÖDER Institute of Aerodynamics, RWTH Aachen University Wüllnerstraße 5 A, D-52062 Aachen The following article summaries the work that has been performed at the Institute of Aerodynamics since roughly 2005 in the field of biomedical flows, a fantastic area where medicine, biology, and fluid mechanics interact. The focus of the discussion is on nasal cavity flows. It represents an excerpt of the work that has been jointly performed with I. Hörschler, M. Meinke, and A. Lintermann. I. Introduction The human nasal cavity must satisfy a variety of functions. Besides respiration it is responsible for moistening, tempering, and cleaning the air. These functions are expected to strongly depend on the complex internal geometry of the nasal cavity. Impaired nasal respiration especially under normal breathing conditions, i.e., in everyday life situations, is a common and widespread disease, which makes nose surgery one of the most often performed operations in the western world. Unfortunately, the success rate, i.e., the number of people having no problems after surgery, is by no means satisfactory. To enhance this situation, it is desired to numerically predict the flow field inside the nose and its relation to geometric changes. This can finally lead to a computer assisted surgery (CAS) tool, that will help on the one hand, to understand the flow in the extremely complex human nasal cavity and on the other hand, to derive criteria how to better predict the outcome and to improve the success of nose operations.