Metastasis in Pancreatic Ductal Adenocarcinoma: Current Standing and Methodologies
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Oncology 101 Dictionary
ONCOLOGY 101 DICTIONARY ACUTE: Symptoms or signs that begin and worsen quickly; not chronic. Example: James experienced acute vomiting after receiving his cancer treatments. ADENOCARCINOMA: Cancer that begins in glandular (secretory) cells. Glandular cells are found in tissue that lines certain internal organs and makes and releases substances in the body, such as mucus, digestive juices, or other fluids. Most cancers of the breast, pancreas, lung, prostate, and colon are adenocarcinomas. Example: The vast majority of rectal cancers are adenocarcinomas. ADENOMA: A tumor that is not cancer. It starts in gland-like cells of the epithelial tissue (thin layer of tissue that covers organs, glands, and other structures within the body). Example: Liver adenomas are rare but can be a cause of abdominal pain. ADJUVANT: Additional cancer treatment given after the primary treatment to lower the risk that the cancer will come back. Adjuvant therapy may include chemotherapy, radiation therapy, hormone therapy, targeted therapy, or biological therapy. Example: The decision to use adjuvant therapy often depends on cancer staging at diagnosis and risk factors of recurrence. BENIGN: Not cancerous. Benign tumors may grow larger but do not spread to other parts of the body. Also called nonmalignant. Example: Mary was relieved when her doctor said the mole on her skin was benign and did not require any further intervention. BIOMARKER TESTING: A group of tests that may be ordered to look for genetic alterations for which there are specific therapies available. The test results may identify certain cancer cells that can be treated with targeted therapies. May also be referred to as genetic testing, molecular testing, molecular profiling, or mutation testing. -

Lung Cancer 2020 Fact Sheet
Lung Cancer 2020 Fact Sheet Lung cancer: the most fatal cancer • The most frequently diagnosed cancer is lung cancer (11.6 percent), followed by female breast (11.6 percent) and colorectal cancers (10.2 percent). • Worldwide lung cancer incidents are on track to increase by 38 percent to 2.89 million by 2030. • Lung cancer is the leading cause of death from cancer at 1.74 million (18.4 percent), followed by colorectal (9.2 percent) and stomach cancers (8.2 percent). • Lung cancer deaths exceed breast cancer mortality for women in 28 countries. • Lung cancer mortality is projected to reach 2.45 million worldwide by 2030, a 39 percent increase since 2018. • About 80 percent of lung cancer deaths are as a result of smoking tobacco. Smokers exposed to other known risk factors such as radon and asbestos are at an even higher risk. • For men, lung cancer is the most prevalent form of cancer, it is third for women. • The five-year cancer survival rate in middle-income countries for all types of lung cancer (19 percent) is lower than many other leading cancer sites, such as the colon (71 percent), breast (85 percent) and prostate (98.9 percent). Treating lung cancer • In lower-income countries, access to care and cost-effective treatments can reduce the human burden and societal impact of lung cancer. • Screening with CT scans compared with chest radiography resulted in a 20 percent reduction in lung cancer-specific deaths, but much cheaper and more accessible methods are needed for low-income settings. • Early-stage lung cancer is treated with curative-intent surgery or radiation therapy. -

Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma
cancers Review Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma Fraser Brims 1,2,3 1 Curtin Medical School, Curtin University, Perth, WA 6845, Australia; [email protected] 2 Department of Respiratory Medicine, Sir Charles Gairdner Hospital, Perth, WA 6009, Australia 3 National Centre for Asbestos Related Diseases, Institute for Respiratory Health, Perth, WA 6009, Australia Simple Summary: Mesothelioma is a cancer of the lining of the lungs caused by breathing in asbestos fibres. Asbestos was widely used in industry in the last century in most developed countries and is still present in many older buildings to this day. There is no known safe level of asbestos exposure. Symptoms of mesothelioma can include worsening breathlessness, chest pain and loss of weight. There is no cure, and the treatment of mesothelioma is limited, although there have been some recent improvements in therapy. Survival is very variable although most people live for around one year after diagnosis. Efforts to improve and maintain the quality of life for patients with mesothelioma remain a priority. Abstract: Mesothelioma is a cancer predominantly of the pleural cavity. There is a clear association of exposure to asbestos with a dose dependent risk of mesothelioma. The incidence of mesothelioma in different countries reflect the historical patterns of commercial asbestos utilisation in the last century and predominant occupational exposures mean that mesothelioma is mostly seen in males. Modern imaging techniques and advances in immunohistochemical staining have contributed to an improved diagnosis of mesothelioma. There have also been recent advances in immune checkpoint inhibition, however, mesothelioma remains very challenging to manage, especially Citation: Brims, F. -
Small Cell Lung Cancer (SCLC) Algorithm
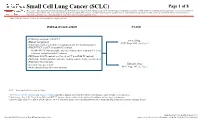
Small Cell Lung Cancer (SCLC) Page 1 of 8 Disclaimer: This algorithm has been developed for MD Anderson using a multidisciplinary approach considering circumstances particular to MD Anderson’s specific patient population, services and structure, and clinical information. This is not intended to replace the independent medical or professional judgment of physicians or other health care providers in the context of individual clinical circumstances to determine a patient's care. This algorithm should not be used to treat pregnant women. Note: Consider Clinical Trials as treatment options for eligible patients. INITIAL EVALUATION STAGE ● Pathology consistent with SCLC Limited Stage ● History and physical AJCC Stage I-III2, see Page 2 ● Laboratory studies to include hematological and full chemistry panels ● FDG PET/CT and CT chest with IV contrast ○ If FDG PET/CT not available: nuclear medicine bone scan and CT chest, abdomen, and pelvis with IV contrast ● MRI brain with IV contrast (preferred) or CT head with IV contrast ● MRI spine, lumbar puncture and bone marrow aspirate/biopsy as indicated ● Pulmonary function tests 1 Extensive Stage ● Lifestyle risk assessment AJCC Stage IV3, see Page 3 ● Molecular profiling (for never smokers) AJCC = American Joint Committee on Cancer 1 See Physical Activity, Nutrition, and Tobacco Cessation algorithms; ongoing reassessment of lifestyle risks should be a part of routine clinical practice 2 Limited stage: Stage I-III (T any, N any, M0) per AJCC 8th edition or disease confined to the ipsilateral hemithorax -

Pathology and Classification of SCLC
cancers Review Pathology and Classification of SCLC Maria Gabriela Raso * , Neus Bota-Rabassedas and Ignacio I. Wistuba * Department of Translational Molecular Pathology, The University of Texas MD Anderson Cancer Center, Houston, TX 77030, USA; [email protected] * Correspondence: [email protected] (M.G.R.); [email protected] (I.I.W.); Tel.: +1-713-834-6026 (M.G.R.); +1-713-563-9184 (I.I.W.) Simple Summary: Small cell lung carcinoma (SCLC), is a high-grade neuroendocrine carcinoma defined by its aggressiveness, poor differentiation, and somber prognosis. This review highlights cur- rent pathological concepts including classification, immunohistochemistry features, and differential diagnosis. Additionally, we summarize the current knowledge of the immune tumor microenvi- ronment, tumor heterogeneity, and genetic variations of SCLC. Recent comprehensive genomic research has improved our understanding of the diverse biological processes that occur in this tumor type, suggesting that a new era of molecular-driven treatment decisions is finally foreseeable for SCLC patients. Abstract: Lung cancer is consistently the leading cause of cancer-related death worldwide, and it ranks as the second most frequent type of new cancer cases diagnosed in the United States, both in males and females. One subtype of lung cancer, small cell lung carcinoma (SCLC), is an aggressive, poorly differentiated, and high-grade neuroendocrine carcinoma that accounts for 13% of all lung carcinomas. SCLC is the most frequent neuroendocrine lung tumor, and it is commonly presented as an advanced stage disease in heavy smokers. Due to its clinical presentation, it is typically diagnosed in small biopsies or cytology specimens, with routine immunostaining only. However, Citation: Raso, M.G.; immunohistochemistry markers are extremely valuable in demonstrating neuroendocrine features of Bota-Rabassedas, N.; Wistuba, I.I. -

Final Lung Cancer Full Slides.Pdf
1 2 Thank you Laurie. Hello everyone, my name is Beth Phelps I am a nurse practitioner and the coordinator of the thoracic oncology program at the SimmonsCooper Cancer Institute in Springfield, IL. I have the pleasure of working with a multidisciplinary panel of physicians to provide advanced cancer care to our patients. As part of our effort to provide the most scientifically advanced care; the physicians participate in clinic trials. Currently, we are participating in numerous research studies including; I-125 radioactive seed implants, vaccine trials, and new protocols for chemotherapy and radiation. 3 My job today is to give you an overview of lung cancer. Other speakers will give you more in-depth information about smoking cessation and radon. As you can see; lung cancer is the leading cause of cancer death in both men and women, and accounts for approximately 72% of all cancer deaths in Illinois. In Illinois, efforts have been made to reduce smoking. The State of Illinois is now smoke free in public buildings. National campaigns like the American Lung Association’s Great American Smoke Out are bringing public awareness to the problem. 4 In Illinois, it was estimated that we would have over 9,000 new cases of lung cancer in 2006 and 7,000 deaths. There are more deaths from lung cancer than prostate, breast, and colorectal cancers combined. 5 Lung cancer in women, account for 12% of all cases of lung cancer. There are more deaths from lung cancer in women than in breast, ovarian, and uterine cancers combined. 6 Despite our best efforts; we are still not making a big enough impact in the incidence of new lung cancers. -

About Lung Cancer What Is Lung Cancer?
cancer.org | 1.800.227.2345 About Lung Cancer Overview and Types If you have been diagnosed with lung cancer or are worried about it, you likely have a lot of questions. Learning some basics is a good place to start. ● What Is Lung Cancer? Research and Statistics See the latest estimates for new cases of lung cancer and deaths in the US and what research is currently being done. ● Key Statistics for Lung Cancer ● What’s New in Lung Cancer Research? What Is Lung Cancer? Lung cancer is a type of cancer that starts in the lungs. Cancer starts when cells in the body begin to grow out of control. To learn more about how cancers start and spread, see What Is Cancer?1 Normal structure and function of the lungs 1 ____________________________________________________________________________________American Cancer Society cancer.org | 1.800.227.2345 Your lungs are 2 sponge-like organs in your chest. Your right lung has 3 sections, called lobes. Your left lung has 2 lobes. The left lung is smaller because the heart takes up more room on that side of the body. When you breathe in, air enters through your mouth or nose and goes into your lungs through the trachea (windpipe). The trachea divides into tubes called bronchi, which enter the lungs and divide into smaller bronchi. These divide to form smaller branches called bronchioles. At the end of the bronchioles are tiny air sacs known as alveoli. The alveoli absorb oxygen into your blood from the inhaled air and remove carbon dioxide from the blood when you exhale. -

Lung Nodules in Melanoma Patients: Morphologic Criteria to Differentiate Non-Metastatic and Metastatic Lesions
diagnostics Article Lung Nodules in Melanoma Patients: Morphologic Criteria to Differentiate Non-Metastatic and Metastatic Lesions Simone Alexandra Stadelmann 1, Christian Blüthgen 1 , Gianluca Milanese 2, Thi Dan Linh Nguyen-Kim 1, Julia-Tatjana Maul 3, Reinhard Dummer 3, Thomas Frauenfelder 1 and Matthias Eberhard 1,* 1 Institute of Diagnostic and Interventional Radiology, University Hospital Zurich, Raemistrasse 100, 8091 Zurich, Switzerland; [email protected] (S.A.S.); [email protected] (C.B.); [email protected] (T.D.L.N.-K.); [email protected] (T.F.) 2 Department of Medicine and Surgery (DiMeC), University of Parma, 43126 Parma, Italy; [email protected] 3 Department of Dermatology, University Hospital Zurich, Raemistrasse 100, 8091 Zurich, Switzerland; [email protected] (J.-T.M.); [email protected] (R.D.) * Correspondence: [email protected]; Tel.: +41-(0)44-255-9139; Fax: +41-(0)44-255-4443 Abstract: Lung nodules are frequent findings in chest computed tomography (CT) in patients with metastatic melanoma. In this study, we assessed the frequency and compared morphologic differences of metastases and benign nodules. We retrospectively evaluated 85 patients with melanoma (AJCC stage III or IV). Inclusion criteria were ≤20 lung nodules and follow-up using CT ≥183 days after baseline. Lung nodules were evaluated for size and morphology. Nodules with significant growth, Citation: Stadelmann, S.A.; Blüthgen, nodule regression in line with RECIST assessment or histologic confirmation were judged to be C.; Milanese, G.; Nguyen-Kim, T.D.L.; metastases. A total of 438 lung nodules were evaluated, of which 68% were metastases. -

Squamous Cell Lung Cancer Foreword
TYPES OF LUNG CANCER UPDATED FEBRUARY 2016 What you need to know about... squamous cell lung cancer foreword About LUNGevity LUNGevity is the largest national lung cancer-focused nonprofit, changing outcomes for people with lung cancer through research, education, and support. About the LUNGevity PATIENT EDUCATION SERIES LUNGevity has developed a comprehensive series of materials for patients/survivors and their caregivers, focused on understanding how lung cancer develops, how it can be diagnosed, and treatment options. Whether you or someone you care about has been diagnosed with lung cancer, or you are concerned about your lung cancer risk, we have resources to help you. The medical experts and lung cancer survivors who provided their valuable expertise and experience in developing these materials all share the belief that well-informed patients make their own best advocates. In addition to this and other brochures in the LUNGevity patient education series, information and resources can be found on LUNGevity’s website at www.LUNGevity.org, under “About Lung Cancer” and “Support & Survivorship.” This patient education booklet was produced through charitable donations from: table of contents 01 Understanding Squamous Cell Lung Cancer ......................................2 What is squamous cell lung cancer? .............................................................................. 2 Diagnosis of squamous cell lung cancer ....................................................................... 3 How is squamous cell lung cancer diagnosed? -

Chemicals, Cancer, and You
Chemicals, Cancer, and You There are many risk factors for cancer: age, family history, viruses and bacteria, lifestyle (behaviors), and contact with (touching, eating, drinking, or breathing) harmful substances. More than 100,000 chemicals are used by Americans, and about 1,000 new chemicals are introduced each year. These chemicals are found in everyday items, such as foods, personal products, packaging, prescription drugs, and household and lawn care products. While some chemicals can be harmful, not all contact with chemicals is dangerous to your health. This booklet will discuss the relationship between contact with harmful chemicals, cancer, and you. It will explain risk factors (things that make you likelier to get cancer), how cancer develops, and how contact with (exposure to) chemicals affects your body. Agency for Toxic Substances and Disease Registry Division of Health Assessment and Consultation CS218078-A 1 Chemicals, Cancer, and You Some factors that increase your risk of developing cancer include behaviors such as smoking, heavy alcohol Examples of Known Human Carcinogens consumption, on-the-job exposure to chemicals, radiation and sun exposure, and some viruses and bacteria. When all these risks are considered together, the role of chemical • Asbestos exposures in causing cancer is small and, as of now, not very clear. Scientists know very little about how contact with • Arsenic most chemicals causes cancer. • Benzene Substances known to cause cancer are called carcinogens. Coming into contact with a carcinogen does not mean you • Beryllium will get cancer. It depends on what you were exposed to, how often you were exposed, and how much you were • Vinyl chloride exposed to, among other things. -

Understanding Lung Nodules
Understanding Lung Nodules Northwestern Memorial Hospital 251 East Huron Street Chicago, Illinois 60611 312.926.2000 Northwestern Medicine Lake Forest Hospital 1000 North Westmoreland Road Lake Forest, Illinois 60045 847.234.5600 TTY for the hearing impaired 312.926.6363 nm.org For healthcare information at your fingertips, download the MyNM app today. 20-335B/1119/200 © 2019 Northwestern Medicine. All rights reserved. Northwestern Medicine Oncology If lung nodules have been found If your screening chest CT shows you have lung nodules, this brochure will help you understand: What they are What follow-up care is needed Why they are important What questions to ask Their size, appearance your physician and composition What are lung nodules? Lung nodules are small areas of abnormal tissue in the lungs. They may also be called spots on the lung, or lesions. These spots may be solitary (single) pulmonary nodules (SPNs) or multiple pulmonary nodules (MPNs). Lung nodules are common. In fact, nearly half of all people have one (or more) by the time they are 50 years old. In the Chicagoland area, nodules are found in nearly 85% of people who are screened for lung cancer. While most lung nodules are benign (not cancerous), almost all lung cancers do start out as nodules. Many lung nodules are caused by infections. Infection causes inflammation, which leads to scarring that may heal in the form of small nodules. Other lung irritants may also cause lung nodules. Inhaling cigarette smoke, or chemicals or fibers at your place of work may lead to lung nodules that could be cancerous. -

Treating Non-Small Cell Lung Cancer
cancer.org | 1.800.227.2345 Treating Non-Small Cell Lung Cancer If you've been diagnosed with non-small cell lung cancer (NSCLC), your cancer care team will discuss your treatment options with you. It's important to weigh the benefits of each treatment option against the possible risks and side effects. How is non-small cell lung cancer treated? Treatments for NSCLC can include: ● Surgery for Non-Small Cell Lung Cancer ● Radiofrequency Ablation (RFA) for Non-Small Cell Lung Cancer ● Radiation Therapy for Non-Small Cell Lung Cancer ● Chemotherapy for Non-Small Cell Lung Cancer ● Targeted Drug Therapy for Non-Small Cell Lung Cancer ● Immunotherapy for Non-Small Cell Lung Cancer ● Palliative Procedures for Non-Small Cell Lung Cancer Common treatment approaches The treatment options for non-small cell lung cancer (NSCLC) are based mainly on the stage (extent) of the cancer, but other factors, such as a person’s overall health and lung function, as well as certain traits of the cancer itself, are also important. In many cases, more than one of type of treatment is used. ● Treatment Choices for Non-Small Cell Lung Cancer, by Stage Who treats non-small cell lung cancer? You may have different types of doctors on your treatment team, depending on the 1 ____________________________________________________________________________________American Cancer Society cancer.org | 1.800.227.2345 stage of your cancer and your treatment options. These doctors could include: ● A thoracic surgeon: a doctor who treats diseases of the lungs and chest with surgery ● A radiation oncologist: a doctor who treats cancer with radiation therapy ● A medical oncologist: a doctor who treats cancer with medicines such as chemotherapy, targeted therapy, and immunotherapy ● A pulmonologist: a doctor who specializes in medical treatment of diseases of the lungs Many other specialists may be involved in your care as well, including nurse practitioners, nurses, psychologists, social workers, rehabilitation specialists, and other health professionals.