Serendipitous Detection of Pancreas Cancer During Lung Cancer Screening with Low-Dose Computed Tomography
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mouth Esophagus Stomach Rectum and Anus Large Intestine Small
1 Liver The liver produces bile, which aids in digestion of fats through a dissolving process known as emulsification. In this process, bile secreted into the small intestine 4 combines with large drops of liquid fat to form Healthy tiny molecular-sized spheres. Within these spheres (micelles), pancreatic enzymes can break down fat (triglycerides) into free fatty acids. Pancreas Digestion The pancreas not only regulates blood glucose 2 levels through production of insulin, but it also manufactures enzymes necessary to break complex The digestive system consists of a long tube (alimen- 5 carbohydrates down into simple sugars (sucrases), tary canal) that varies in shape and purpose as it winds proteins into individual amino acids (proteases), and its way through the body from the mouth to the anus fats into free fatty acids (lipase). These enzymes are (see diagram). The size and shape of the digestive tract secreted into the small intestine. varies in each individual (e.g., age, size, gender, and disease state). The upper part of the GI tract includes the mouth, throat (pharynx), esophagus, and stomach. The lower Gallbladder part includes the small intestine, large intestine, The gallbladder stores bile produced in the liver appendix, and rectum. While not part of the alimentary 6 and releases it into the duodenum in varying canal, the liver, pancreas, and gallbladder are all organs concentrations. that are vital to healthy digestion. 3 Small Intestine Mouth Within the small intestine, millions of tiny finger-like When food enters the mouth, chewing breaks it 4 protrusions called villi, which are covered in hair-like down and mixes it with saliva, thus beginning the first 5 protrusions called microvilli, aid in absorption of of many steps in the digestive process. -

Pancreatic Cancer
A Patient’s Guide to Pancreatic Cancer COMPREHENSIVE CANCER CENTER Staff of the Comprehensive Cancer Center’s Multidisciplinary Pancreatic Cancer Program provided information for this handbook GI Oncology Program, Patient Education Program, Gastrointestinal Surgery Department, Medical Oncology, Radiation Oncology and Surgical Oncology Digestive System Anatomy Esophagus Liver Stomach Gallbladder Duodenum Colon Pancreas (behind the stomach) Anatomy of the Pancreas Celiac Plexus Pancreatic Duct Common Bile Duct Sphincter of Oddi Head Body Tail Pancreas ii A Patient’s Guide to Pancreatic Cancer ©2012 University of Michigan Comprehensive Cancer Center Table of Contents I. Overview of pancreatic cancer A. Where is the pancreas located?. 1 B. What does the pancreas do? . 2 C. What is cancer and how does it affect the pancreas? .....................2 D. How common is pancreatic cancer and who is at risk?. .3 E. Is pancreatic cancer hereditary? .....................................3 F. What are the symptoms of pancreatic cancer? ..........................4 G. How is pancreatic cancer diagnosed?. 7 H. What are the types of cancer found in the pancreas? .....................9 II. Treatment A. Treatment of Pancreatic Cancer. 11 1. What are the treatment options?. 11 2. How does a patient decide on treatment? ..........................12 3. What factors affect prognosis and recovery?. .12 D. Surgery. 13 1. When is surgery a treatment?. 13 2. What other procedures are done?. .16 E. Radiation therapy . 19 1. What is radiation therapy? ......................................19 2. When is radiation therapy given?. 19 3. What happens at my first appointment? . 20 F. Chemotherapy ..................................................21 1. What is chemotherapy? ........................................21 2. How does chemotherapy work? ..................................21 3. When is chemotherapy given? ...................................21 G. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

And Pancreas Divisum
Gut: first published as 10.1136/gut.27.2.203 on 1 February 1986. Downloaded from Gut 1986, 27, 203-212 Progress report A historical perspective on the discovery of the accessory duct of the pancreas, the ampulla 'of Vater' andpancreas divisum SUMMARY The discovery of the accessory duct of the pancreas is usually ascribed to Giovanni Domenico Santorini (1681-1737), after whom this structure is named. The papilla duodeni (ampulla 'of Vater', or papilla 'of Santorini') is named after Abraham Vater (1684-1751) or after GD Santorini. Pancreas divisum, a persistence through non-fusion of the embryonic dorsal and ventral pancreas is a relatively common clinical condition, the discovery of which is usually ascribed to Joseph Hyrtl (1810-1894). In this review I report that pancreas divisum, the accessory duct and the papilla duodeni (ampulla 'of Vater') had all been observed and the observations published during the 17th century by at least seven anatomists before Santorini, Vater, and Hyrtl. I further suggest, in the light of frequent anatomical misattributions in common usage, that anatomical structures be referred to only by their proper anatomical names. The human pancreas forms during the seventh week of embryonic http://gut.bmj.com/ development by the fusion of two pancreatic primordia, one dorsal and the other ventral.1 4Each of these two primordia contains a duct, opening into the duodenum. After fusion, the distal part of the main duct of the pancreas ('Wirsung's duct') is formed from the duct of the ventral pancreas, and its proximal part from the proximal portion of the duct of the dorsal primordium. -

Oncology 101 Dictionary
ONCOLOGY 101 DICTIONARY ACUTE: Symptoms or signs that begin and worsen quickly; not chronic. Example: James experienced acute vomiting after receiving his cancer treatments. ADENOCARCINOMA: Cancer that begins in glandular (secretory) cells. Glandular cells are found in tissue that lines certain internal organs and makes and releases substances in the body, such as mucus, digestive juices, or other fluids. Most cancers of the breast, pancreas, lung, prostate, and colon are adenocarcinomas. Example: The vast majority of rectal cancers are adenocarcinomas. ADENOMA: A tumor that is not cancer. It starts in gland-like cells of the epithelial tissue (thin layer of tissue that covers organs, glands, and other structures within the body). Example: Liver adenomas are rare but can be a cause of abdominal pain. ADJUVANT: Additional cancer treatment given after the primary treatment to lower the risk that the cancer will come back. Adjuvant therapy may include chemotherapy, radiation therapy, hormone therapy, targeted therapy, or biological therapy. Example: The decision to use adjuvant therapy often depends on cancer staging at diagnosis and risk factors of recurrence. BENIGN: Not cancerous. Benign tumors may grow larger but do not spread to other parts of the body. Also called nonmalignant. Example: Mary was relieved when her doctor said the mole on her skin was benign and did not require any further intervention. BIOMARKER TESTING: A group of tests that may be ordered to look for genetic alterations for which there are specific therapies available. The test results may identify certain cancer cells that can be treated with targeted therapies. May also be referred to as genetic testing, molecular testing, molecular profiling, or mutation testing. -

Fact Sheet - Symptoms of Pancreatic Cancer
Fact Sheet - Symptoms of Pancreatic Cancer Diagnosis Pancreatic cancer is often difficult to diagnose, because the pancreas lies deep in the abdomen, behind the stomach, so tumors are not felt during a physical exam. Pancreatic cancer is often called the “silent” cancer because the tumor can grow for many years before it causes pressure, pain, or other signs of illness. When symptoms do appear, they can vary depending on the size of the tumor and where it is located on the pancreas. For these reasons, the symptoms of pancreatic cancer are seldom recognized until the cancer has progressed to an advanced stage and often spread to other areas of the body. General Symptoms Pain The first symptom of pancreatic cancer is often pain, because the tumors invade nerve clusters. Pain can be felt in the stomach area and/or in the back. The pain is generally worse after eating and when lying down, and is sometimes relieved by bending forward. Pain is more common in cancers of the body and tail of the pancreas. The abdomen may also be generally tender or painful if the liver, pancreas or gall bladder are inflamed or enlarged. It is important to keep in mind that there are many other causes of abdominal and back pain! Jaundice More than half of pancreatic cancer sufferers have jaundice, a yellowing of the skin and whites of the eyes. Jaundice is caused by a build-up bilirubin, a substance which is made in the liver and a component of bile. Bilirubin contains a lot of yellow pigment, and gives bile it’s color. -

Lung Cancer 2020 Fact Sheet
Lung Cancer 2020 Fact Sheet Lung cancer: the most fatal cancer • The most frequently diagnosed cancer is lung cancer (11.6 percent), followed by female breast (11.6 percent) and colorectal cancers (10.2 percent). • Worldwide lung cancer incidents are on track to increase by 38 percent to 2.89 million by 2030. • Lung cancer is the leading cause of death from cancer at 1.74 million (18.4 percent), followed by colorectal (9.2 percent) and stomach cancers (8.2 percent). • Lung cancer deaths exceed breast cancer mortality for women in 28 countries. • Lung cancer mortality is projected to reach 2.45 million worldwide by 2030, a 39 percent increase since 2018. • About 80 percent of lung cancer deaths are as a result of smoking tobacco. Smokers exposed to other known risk factors such as radon and asbestos are at an even higher risk. • For men, lung cancer is the most prevalent form of cancer, it is third for women. • The five-year cancer survival rate in middle-income countries for all types of lung cancer (19 percent) is lower than many other leading cancer sites, such as the colon (71 percent), breast (85 percent) and prostate (98.9 percent). Treating lung cancer • In lower-income countries, access to care and cost-effective treatments can reduce the human burden and societal impact of lung cancer. • Screening with CT scans compared with chest radiography resulted in a 20 percent reduction in lung cancer-specific deaths, but much cheaper and more accessible methods are needed for low-income settings. • Early-stage lung cancer is treated with curative-intent surgery or radiation therapy. -

Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma
cancers Review Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma Fraser Brims 1,2,3 1 Curtin Medical School, Curtin University, Perth, WA 6845, Australia; [email protected] 2 Department of Respiratory Medicine, Sir Charles Gairdner Hospital, Perth, WA 6009, Australia 3 National Centre for Asbestos Related Diseases, Institute for Respiratory Health, Perth, WA 6009, Australia Simple Summary: Mesothelioma is a cancer of the lining of the lungs caused by breathing in asbestos fibres. Asbestos was widely used in industry in the last century in most developed countries and is still present in many older buildings to this day. There is no known safe level of asbestos exposure. Symptoms of mesothelioma can include worsening breathlessness, chest pain and loss of weight. There is no cure, and the treatment of mesothelioma is limited, although there have been some recent improvements in therapy. Survival is very variable although most people live for around one year after diagnosis. Efforts to improve and maintain the quality of life for patients with mesothelioma remain a priority. Abstract: Mesothelioma is a cancer predominantly of the pleural cavity. There is a clear association of exposure to asbestos with a dose dependent risk of mesothelioma. The incidence of mesothelioma in different countries reflect the historical patterns of commercial asbestos utilisation in the last century and predominant occupational exposures mean that mesothelioma is mostly seen in males. Modern imaging techniques and advances in immunohistochemical staining have contributed to an improved diagnosis of mesothelioma. There have also been recent advances in immune checkpoint inhibition, however, mesothelioma remains very challenging to manage, especially Citation: Brims, F. -

Liver, Gallbladder, Bile Ducts, Pancreas
Liver, gallbladder, bile ducts, pancreas Coding issues Otto Visser May 2021 Anatomy Liver, gallbladder and the proximal bile ducts Incidence of liver cancer in Europe in 2018 males females Relative survival of liver cancer (2000 10% 15% 20% 25% 30% 35% 40% 45% 50% 0% 5% Bulgaria Latvia Estonia Czechia Slovakia Malta Denmark Croatia Lithuania N Ireland Slovenia Wales Poland England Norway Scotland Sweden Netherlands Finland Iceland Ireland Austria Portugal EUROPE - Germany 2007) Spain Switzerland France Belgium Italy five year one year Liver: topography • C22.1 = intrahepatic bile ducts • C22.0 = liver, NOS Liver: morphology • Hepatocellular carcinoma=HCC (8170; C22.0) • Intrahepatic cholangiocarcinoma=ICC (8160; C22.1) • Mixed HCC/ICC (8180; TNM: C22.1; ICD-O: C22.0) • Hepatoblastoma (8970; C22.0) • Malignant rhabdoid tumour (8963; (C22.0) • Sarcoma (C22.0) • Angiosarcoma (9120) • Epithelioid haemangioendothelioma (9133) • Embryonal sarcoma (8991)/rhabdomyosarcoma (8900-8920) Morphology*: distribution by sex (NL 2011-17) other other ICC 2% 3% 28% ICC 56% HCC 41% HCC 70% males females * Only pathologically confirmed cases Liver cancer: primary or metastatic? Be aware that other and unspecified morphologies are likely to be metastatic, unless there is evidence of the contrary. For example, primary neuro-endocrine tumours (including small cell carcinoma) of the liver are extremely rare. So, when you have a diagnosis of a carcinoid or small cell carcinoma in the liver, this is probably a metastatic tumour. Anatomy of the bile ducts Gallbladder -

Nomina Histologica Veterinaria, First Edition
NOMINA HISTOLOGICA VETERINARIA Submitted by the International Committee on Veterinary Histological Nomenclature (ICVHN) to the World Association of Veterinary Anatomists Published on the website of the World Association of Veterinary Anatomists www.wava-amav.org 2017 CONTENTS Introduction i Principles of term construction in N.H.V. iii Cytologia – Cytology 1 Textus epithelialis – Epithelial tissue 10 Textus connectivus – Connective tissue 13 Sanguis et Lympha – Blood and Lymph 17 Textus muscularis – Muscle tissue 19 Textus nervosus – Nerve tissue 20 Splanchnologia – Viscera 23 Systema digestorium – Digestive system 24 Systema respiratorium – Respiratory system 32 Systema urinarium – Urinary system 35 Organa genitalia masculina – Male genital system 38 Organa genitalia feminina – Female genital system 42 Systema endocrinum – Endocrine system 45 Systema cardiovasculare et lymphaticum [Angiologia] – Cardiovascular and lymphatic system 47 Systema nervosum – Nervous system 52 Receptores sensorii et Organa sensuum – Sensory receptors and Sense organs 58 Integumentum – Integument 64 INTRODUCTION The preparations leading to the publication of the present first edition of the Nomina Histologica Veterinaria has a long history spanning more than 50 years. Under the auspices of the World Association of Veterinary Anatomists (W.A.V.A.), the International Committee on Veterinary Anatomical Nomenclature (I.C.V.A.N.) appointed in Giessen, 1965, a Subcommittee on Histology and Embryology which started a working relation with the Subcommittee on Histology of the former International Anatomical Nomenclature Committee. In Mexico City, 1971, this Subcommittee presented a document entitled Nomina Histologica Veterinaria: A Working Draft as a basis for the continued work of the newly-appointed Subcommittee on Histological Nomenclature. This resulted in the editing of the Nomina Histologica Veterinaria: A Working Draft II (Toulouse, 1974), followed by preparations for publication of a Nomina Histologica Veterinaria. -
Small Cell Lung Cancer (SCLC) Algorithm
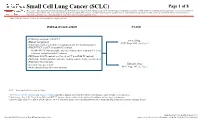
Small Cell Lung Cancer (SCLC) Page 1 of 8 Disclaimer: This algorithm has been developed for MD Anderson using a multidisciplinary approach considering circumstances particular to MD Anderson’s specific patient population, services and structure, and clinical information. This is not intended to replace the independent medical or professional judgment of physicians or other health care providers in the context of individual clinical circumstances to determine a patient's care. This algorithm should not be used to treat pregnant women. Note: Consider Clinical Trials as treatment options for eligible patients. INITIAL EVALUATION STAGE ● Pathology consistent with SCLC Limited Stage ● History and physical AJCC Stage I-III2, see Page 2 ● Laboratory studies to include hematological and full chemistry panels ● FDG PET/CT and CT chest with IV contrast ○ If FDG PET/CT not available: nuclear medicine bone scan and CT chest, abdomen, and pelvis with IV contrast ● MRI brain with IV contrast (preferred) or CT head with IV contrast ● MRI spine, lumbar puncture and bone marrow aspirate/biopsy as indicated ● Pulmonary function tests 1 Extensive Stage ● Lifestyle risk assessment AJCC Stage IV3, see Page 3 ● Molecular profiling (for never smokers) AJCC = American Joint Committee on Cancer 1 See Physical Activity, Nutrition, and Tobacco Cessation algorithms; ongoing reassessment of lifestyle risks should be a part of routine clinical practice 2 Limited stage: Stage I-III (T any, N any, M0) per AJCC 8th edition or disease confined to the ipsilateral hemithorax -

Pathology and Classification of SCLC
cancers Review Pathology and Classification of SCLC Maria Gabriela Raso * , Neus Bota-Rabassedas and Ignacio I. Wistuba * Department of Translational Molecular Pathology, The University of Texas MD Anderson Cancer Center, Houston, TX 77030, USA; [email protected] * Correspondence: [email protected] (M.G.R.); [email protected] (I.I.W.); Tel.: +1-713-834-6026 (M.G.R.); +1-713-563-9184 (I.I.W.) Simple Summary: Small cell lung carcinoma (SCLC), is a high-grade neuroendocrine carcinoma defined by its aggressiveness, poor differentiation, and somber prognosis. This review highlights cur- rent pathological concepts including classification, immunohistochemistry features, and differential diagnosis. Additionally, we summarize the current knowledge of the immune tumor microenvi- ronment, tumor heterogeneity, and genetic variations of SCLC. Recent comprehensive genomic research has improved our understanding of the diverse biological processes that occur in this tumor type, suggesting that a new era of molecular-driven treatment decisions is finally foreseeable for SCLC patients. Abstract: Lung cancer is consistently the leading cause of cancer-related death worldwide, and it ranks as the second most frequent type of new cancer cases diagnosed in the United States, both in males and females. One subtype of lung cancer, small cell lung carcinoma (SCLC), is an aggressive, poorly differentiated, and high-grade neuroendocrine carcinoma that accounts for 13% of all lung carcinomas. SCLC is the most frequent neuroendocrine lung tumor, and it is commonly presented as an advanced stage disease in heavy smokers. Due to its clinical presentation, it is typically diagnosed in small biopsies or cytology specimens, with routine immunostaining only. However, Citation: Raso, M.G.; immunohistochemistry markers are extremely valuable in demonstrating neuroendocrine features of Bota-Rabassedas, N.; Wistuba, I.I.