Pathology and Classification of SCLC
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cholangiocarcinoma 2020: the Next Horizon in Mechanisms and Management
CONSENSUS STATEMENT Cholangiocarcinoma 2020: the next horizon in mechanisms and management Jesus M. Banales 1,2,3 ✉ , Jose J. G. Marin 2,4, Angela Lamarca 5,6, Pedro M. Rodrigues 1, Shahid A. Khan7, Lewis R. Roberts 8, Vincenzo Cardinale9, Guido Carpino 10, Jesper B. Andersen 11, Chiara Braconi 12, Diego F. Calvisi13, Maria J. Perugorria1,2, Luca Fabris 14,15, Luke Boulter 16, Rocio I. R. Macias 2,4, Eugenio Gaudio17, Domenico Alvaro18, Sergio A. Gradilone19, Mario Strazzabosco 14,15, Marco Marzioni20, Cédric Coulouarn21, Laura Fouassier 22, Chiara Raggi23, Pietro Invernizzi 24, Joachim C. Mertens25, Anja Moncsek25, Sumera Rizvi8, Julie Heimbach26, Bas Groot Koerkamp 27, Jordi Bruix2,28, Alejandro Forner 2,28, John Bridgewater 29, Juan W. Valle 5,6 and Gregory J. Gores 8 Abstract | Cholangiocarcinoma (CCA) includes a cluster of highly heterogeneous biliary malignant tumours that can arise at any point of the biliary tree. Their incidence is increasing globally, currently accounting for ~15% of all primary liver cancers and ~3% of gastrointestinal malignancies. The silent presentation of these tumours combined with their highly aggressive nature and refractoriness to chemotherapy contribute to their alarming mortality, representing ~2% of all cancer-related deaths worldwide yearly. The current diagnosis of CCA by non-invasive approaches is not accurate enough, and histological confirmation is necessary. Furthermore, the high heterogeneity of CCAs at the genomic, epigenetic and molecular levels severely compromises the efficacy of the available therapies. In the past decade, increasing efforts have been made to understand the complexity of these tumours and to develop new diagnostic tools and therapies that might help to improve patient outcomes. -

The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Inherited Polyposis Syndromes Daniel Herzig, M.D
CLINICAL PRACTICE GUIDELINES The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Inherited Polyposis Syndromes Daniel Herzig, M.D. • Karin Hardimann, M.D. • Martin Weiser, M.D. • Nancy Yu, M.D. Ian Paquette, M.D. • Daniel L. Feingold, M.D. • Scott R. Steele, M.D. Prepared by the Clinical Practice Guidelines Committee of The American Society of Colon and Rectal Surgeons he American Society of Colon and Rectal Surgeons METHODOLOGY (ASCRS) is dedicated to ensuring high-quality pa- tient care by advancing the science, prevention, and These guidelines are built on the last set of the ASCRS T Practice Parameters for the Identification and Testing of management of disorders and diseases of the colon, rectum, Patients at Risk for Dominantly Inherited Colorectal Can- and anus. The Clinical Practice Guidelines Committee is 1 composed of society members who are chosen because they cer published in 2003. An organized search of MEDLINE have demonstrated expertise in the specialty of colon and (1946 to December week 1, 2016) was performed from rectal surgery. This committee was created to lead interna- 1946 through week 4 of September 2016 (Fig. 1). Subject tional efforts in defining quality care for conditions related headings for “adenomatous polyposis coli” (4203 results) to the colon, rectum, and anus, in addition to the devel- and “intestinal polyposis” (445 results) were included, us- opment of Clinical Practice Guidelines based on the best ing focused search. The results were combined (4629 re- available evidence. These guidelines are inclusive and not sults) and limited to English language (3981 results), then prescriptive. -

Germline Fumarate Hydratase Mutations in Patients with Ovarian Mucinous Cystadenoma
European Journal of Human Genetics (2006) 14, 880–883 & 2006 Nature Publishing Group All rights reserved 1018-4813/06 $30.00 www.nature.com/ejhg SHORT REPORT Germline fumarate hydratase mutations in patients with ovarian mucinous cystadenoma Sanna K Ylisaukko-oja1, Cezary Cybulski2, Rainer Lehtonen1, Maija Kiuru1, Joanna Matyjasik2, Anna Szyman˜ska2, Jolanta Szyman˜ska-Pasternak2, Lars Dyrskjot3, Ralf Butzow4, Torben F Orntoft3, Virpi Launonen1, Jan Lubin˜ski2 and Lauri A Aaltonen*,1 1Department of Medical Genetics, Biomedicum Helsinki, University of Helsinki, Helsinki, Finland; 2International Hereditary Cancer Center, Department of Genetics and Pathology, Pomeranian Medical University, Szczecin, Poland; 3Department of Clinical Biochemistry, Aarhus University Hospital, Skejby, Denmark; 4Pathology and Obstetrics and Gynecology, University of Helsinki, Helsinki, Finland Germline mutations in the fumarate hydratase (FH) gene were recently shown to predispose to the dominantly inherited syndrome, hereditary leiomyomatosis and renal cell cancer (HLRCC). HLRCC is characterized by benign leiomyomas of the skin and the uterus, renal cell carcinoma, and uterine leiomyosarcoma. The aim of this study was to identify new families with FH mutations, and to further examine the tumor spectrum associated with FH mutations. FH germline mutations were screened from 89 patients with RCC, skin leiomyomas or ovarian tumors. Subsequently, 13 ovarian and 48 bladder carcinomas were analyzed for somatic FH mutations. Two patients diagnosed with ovarian mucinous cystadenoma (two out of 33, 6%) were found to be FH germline mutation carriers. One of the changes was a novel mutation (Ala231Thr) and the other one (435insAAA) was previously described in FH deficiency families. These results suggest that benign ovarian tumors may be associated with HLRCC. -

HPV-Negative Penile Squamous Cell Carcinoma
Modern Pathology (2017) 30, 1013–1020 © 2017 USCAP, Inc All rights reserved 0893-3952/17 $32.00 1013 HPV-negative penile squamous cell carcinoma: disruptive mutations in the TP53 gene are common Karl Kashofer, Elke Winter, Iris Halbwedl, Andrea Thueringer, Marisa Kreiner, Stefan Sauer and Sigrid Regauer Institute of Pathology, Medical University of Graz, Graz, Austria The majority of penile squamous cell carcinomas is caused by transforming human papilloma virus (HPV) infection. The etiology of HPV-negative cancers is unclear, but TP53 mutations have been implicated. Archival tissues of 108 invasive squamous cell carcinoma from a single pathology institution in a low-incidence area were analyzed for HPV-DNA and p16ink4a overexpression and for TP53 mutations by ion torrent next-generation sequencing. Library preparation failed in 32/108 squamous cell carcinomas. Institutional review board approval was obtained. Thirty of 76 squamous cell carcinomas (43%; average 63 years) were HPV-negative with 8/33 squamous cell carcinomas being TP53 wild-type (24%; average 63 years). Twenty-five of 33 squamous cell carcinomas (76%; average 65 years) showed 32 different somatic TP53 mutations (23 missense mutations in exons 5–8, 6 nonsense, 1 frameshift and 2 splice-site mutations). Several hotspot mutations were detected multiple times (R175H, R248, R282, and R273). Eighteen of 19 squamous cell carcinomas with TP53 expression in immunohistochemistry had TP53 mutations. Fifty percent of TP53-negative squamous cell carcinomas showed mostly truncating loss-of-function TP53 mutations. Patients without mutations had longer survival (5 years: 86% vs 61%; 10 years: 60% vs 22%), but valid clinically relevant conclusions cannot be drawn due to different tumor stages and heterogeneous treatment of the cases presented in this study. -

Oncology 101 Dictionary
ONCOLOGY 101 DICTIONARY ACUTE: Symptoms or signs that begin and worsen quickly; not chronic. Example: James experienced acute vomiting after receiving his cancer treatments. ADENOCARCINOMA: Cancer that begins in glandular (secretory) cells. Glandular cells are found in tissue that lines certain internal organs and makes and releases substances in the body, such as mucus, digestive juices, or other fluids. Most cancers of the breast, pancreas, lung, prostate, and colon are adenocarcinomas. Example: The vast majority of rectal cancers are adenocarcinomas. ADENOMA: A tumor that is not cancer. It starts in gland-like cells of the epithelial tissue (thin layer of tissue that covers organs, glands, and other structures within the body). Example: Liver adenomas are rare but can be a cause of abdominal pain. ADJUVANT: Additional cancer treatment given after the primary treatment to lower the risk that the cancer will come back. Adjuvant therapy may include chemotherapy, radiation therapy, hormone therapy, targeted therapy, or biological therapy. Example: The decision to use adjuvant therapy often depends on cancer staging at diagnosis and risk factors of recurrence. BENIGN: Not cancerous. Benign tumors may grow larger but do not spread to other parts of the body. Also called nonmalignant. Example: Mary was relieved when her doctor said the mole on her skin was benign and did not require any further intervention. BIOMARKER TESTING: A group of tests that may be ordered to look for genetic alterations for which there are specific therapies available. The test results may identify certain cancer cells that can be treated with targeted therapies. May also be referred to as genetic testing, molecular testing, molecular profiling, or mutation testing. -

Lung Equivalent Terms, Definitions, Charts, Tables and Illustrations C340-C349 (Excludes Lymphoma and Leukemia M9590-9989 and Kaposi Sarcoma M9140)
Lung Equivalent Terms, Definitions, Charts, Tables and Illustrations C340-C349 (Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140) Introduction Use these rules only for cases with primary lung cancer. Lung carcinomas may be broadly grouped into two categories, small cell and non-small cell carcinoma. Frequently a patient may have two or more tumors in one lung and may have one or more tumors in the contralateral lung. The physician may biopsy only one of the tumors. Code the case as a single primary (See Rule M1, Note 2) unless one of the tumors is proven to be a different histology. It is irrelevant whether the other tumors are identified as cancer, primary tumors, or metastases. Equivalent or Equal Terms • Low grade neuroendocrine carcinoma, carcinoid • Tumor, mass, lesion, neoplasm (for multiple primary and histology coding rules only) • Type, subtype, predominantly, with features of, major, or with ___differentiation Obsolete Terms for Small Cell Carcinoma (Terms that are no longer recognized) • Intermediate cell carcinoma (8044) • Mixed small cell/large cell carcinoma (8045) (Code is still used; however current accepted terminology is combined small cell carcinoma) • Oat cell carcinoma (8042) • Small cell anaplastic carcinoma (No ICD-O-3 code) • Undifferentiated small cell carcinoma (No ICD-O-3 code) Definitions Adenocarcinoma with mixed subtypes (8255): A mixture of two or more of the subtypes of adenocarcinoma such as acinar, papillary, bronchoalveolar, or solid with mucin formation. Adenosquamous carcinoma (8560): A single histology in a single tumor composed of both squamous cell carcinoma and adenocarcinoma. Bilateral lung cancer: This phrase simply means that there is at least one malignancy in the right lung and at least one malignancy in the left lung. -

Lung Cancer 2020 Fact Sheet
Lung Cancer 2020 Fact Sheet Lung cancer: the most fatal cancer • The most frequently diagnosed cancer is lung cancer (11.6 percent), followed by female breast (11.6 percent) and colorectal cancers (10.2 percent). • Worldwide lung cancer incidents are on track to increase by 38 percent to 2.89 million by 2030. • Lung cancer is the leading cause of death from cancer at 1.74 million (18.4 percent), followed by colorectal (9.2 percent) and stomach cancers (8.2 percent). • Lung cancer deaths exceed breast cancer mortality for women in 28 countries. • Lung cancer mortality is projected to reach 2.45 million worldwide by 2030, a 39 percent increase since 2018. • About 80 percent of lung cancer deaths are as a result of smoking tobacco. Smokers exposed to other known risk factors such as radon and asbestos are at an even higher risk. • For men, lung cancer is the most prevalent form of cancer, it is third for women. • The five-year cancer survival rate in middle-income countries for all types of lung cancer (19 percent) is lower than many other leading cancer sites, such as the colon (71 percent), breast (85 percent) and prostate (98.9 percent). Treating lung cancer • In lower-income countries, access to care and cost-effective treatments can reduce the human burden and societal impact of lung cancer. • Screening with CT scans compared with chest radiography resulted in a 20 percent reduction in lung cancer-specific deaths, but much cheaper and more accessible methods are needed for low-income settings. • Early-stage lung cancer is treated with curative-intent surgery or radiation therapy. -

Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma
cancers Review Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma Fraser Brims 1,2,3 1 Curtin Medical School, Curtin University, Perth, WA 6845, Australia; [email protected] 2 Department of Respiratory Medicine, Sir Charles Gairdner Hospital, Perth, WA 6009, Australia 3 National Centre for Asbestos Related Diseases, Institute for Respiratory Health, Perth, WA 6009, Australia Simple Summary: Mesothelioma is a cancer of the lining of the lungs caused by breathing in asbestos fibres. Asbestos was widely used in industry in the last century in most developed countries and is still present in many older buildings to this day. There is no known safe level of asbestos exposure. Symptoms of mesothelioma can include worsening breathlessness, chest pain and loss of weight. There is no cure, and the treatment of mesothelioma is limited, although there have been some recent improvements in therapy. Survival is very variable although most people live for around one year after diagnosis. Efforts to improve and maintain the quality of life for patients with mesothelioma remain a priority. Abstract: Mesothelioma is a cancer predominantly of the pleural cavity. There is a clear association of exposure to asbestos with a dose dependent risk of mesothelioma. The incidence of mesothelioma in different countries reflect the historical patterns of commercial asbestos utilisation in the last century and predominant occupational exposures mean that mesothelioma is mostly seen in males. Modern imaging techniques and advances in immunohistochemical staining have contributed to an improved diagnosis of mesothelioma. There have also been recent advances in immune checkpoint inhibition, however, mesothelioma remains very challenging to manage, especially Citation: Brims, F. -

What Are Basal and Squamous Cell Skin Cancers?
cancer.org | 1.800.227.2345 About Basal and Squamous Cell Skin Cancer Overview If you have been diagnosed with basal or squamous cell skin cancer or are worried about it, you likely have a lot of questions. Learning some basics is a good place to start. ● What Are Basal and Squamous Cell Skin Cancers? Research and Statistics See the latest estimates for new cases of basal and squamous cell skin cancer and deaths in the US and what research is currently being done. ● Key Statistics for Basal and Squamous Cell Skin Cancers ● What’s New in Basal and Squamous Cell Skin Cancer Research? What Are Basal and Squamous Cell Skin Cancers? Basal and squamous cell skin cancers are the most common types of skin cancer. They start in the top layer of skin (the epidermis), and are often related to sun exposure. 1 ____________________________________________________________________________________American Cancer Society cancer.org | 1.800.227.2345 Cancer starts when cells in the body begin to grow out of control. Cells in nearly any part of the body can become cancer cells. To learn more about cancer and how it starts and spreads, see What Is Cancer?1 Where do skin cancers start? Most skin cancers start in the top layer of skin, called the epidermis. There are 3 main types of cells in this layer: ● Squamous cells: These are flat cells in the upper (outer) part of the epidermis, which are constantly shed as new ones form. When these cells grow out of control, they can develop into squamous cell skin cancer (also called squamous cell carcinoma). -
Small Cell Lung Cancer (SCLC) Algorithm
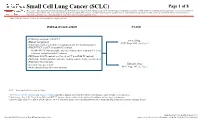
Small Cell Lung Cancer (SCLC) Page 1 of 8 Disclaimer: This algorithm has been developed for MD Anderson using a multidisciplinary approach considering circumstances particular to MD Anderson’s specific patient population, services and structure, and clinical information. This is not intended to replace the independent medical or professional judgment of physicians or other health care providers in the context of individual clinical circumstances to determine a patient's care. This algorithm should not be used to treat pregnant women. Note: Consider Clinical Trials as treatment options for eligible patients. INITIAL EVALUATION STAGE ● Pathology consistent with SCLC Limited Stage ● History and physical AJCC Stage I-III2, see Page 2 ● Laboratory studies to include hematological and full chemistry panels ● FDG PET/CT and CT chest with IV contrast ○ If FDG PET/CT not available: nuclear medicine bone scan and CT chest, abdomen, and pelvis with IV contrast ● MRI brain with IV contrast (preferred) or CT head with IV contrast ● MRI spine, lumbar puncture and bone marrow aspirate/biopsy as indicated ● Pulmonary function tests 1 Extensive Stage ● Lifestyle risk assessment AJCC Stage IV3, see Page 3 ● Molecular profiling (for never smokers) AJCC = American Joint Committee on Cancer 1 See Physical Activity, Nutrition, and Tobacco Cessation algorithms; ongoing reassessment of lifestyle risks should be a part of routine clinical practice 2 Limited stage: Stage I-III (T any, N any, M0) per AJCC 8th edition or disease confined to the ipsilateral hemithorax -

Leishmania Infection and Neuroinflammation
Journal of Neuroimmunology 289 (2015) 21–29 Contents lists available at ScienceDirect Journal of Neuroimmunology journal homepage: www.elsevier.com/locate/jneuroim Leishmania infection and neuroinflammation: Specific chemokine profile and absence of parasites in the brain of naturally-infected dogs Guilherme D. Melo a,1, José Eduardo S. Silva a,FernandaG.Granoa,MilenaS.Souzab,GiseleF.Machadoa,⁎ a Faculdade de Medicina Veterinária, UNESP – Univ Estadual Paulista, Laboratório de Patologia Aplicada (LApap), Araçatuba, São Paulo, Brazil b Faculdade de Medicina Veterinária, UNESP – Univ Estadual Paulista, Araçatuba, São Paulo, Brazil article info abstract Article history: Visceral leishmaniasis is a chronic disease caused by Leishmania infantum. We aimed to detect the parasite in the Received 24 June 2015 brain of fifteen naturally-infected dogs using in situ hybridization and immunohistochemistry, and the gene ex- Received in revised form 28 August 2015 pression of selected chemokines by RT-qPCR. We detected no parasite in the brain, but perivascular deposition of Accepted 8 October 2015 parasite DNA and IgG in the choroid plexus. We noticed up-regulation of CCL-3, CCL-4 and CCL-5, coherent with T lymphocyte accumulation, stating the brain as a pro-inflammatory environment. Indeed, not necessarily the par- Keywords: fl Chemokine CCL3 asite itself, but rather its DNA seems to act as a trigger to promote brain in ammation during visceral Chemokine CCL4 leishmaniasis. Chemokine CCL5 © 2015 Elsevier B.V. All rights reserved. Central nervous system Tlymphocytes Visceral leishmaniasis 1. Introduction Specifically in the brain, the parasite is not often detected (Márquez et al., 2013; Viñuelas et al., 2001), however, inflammatory lesions even Visceral leishmaniasis (VL) is a chronic disease caused by parasitic in the absence of the parasite are commonly observed, predominantly protozoans from the Leishmania donovani complex, namely L. -

Primary Neuroendocrine Small Cell Carcinoma in Larynx
Romanian Journal of Rhinology, Vol. 7, No. 27, July - September 2017 DOI: 10.1515/rjr-2017-0021 CASE REPORT Primary neuroendocrine small cell carcinoma in larynx: case report and literature review Anca Evsei1,2 , Cristina Iosif2, Simona Enache2,3, Claudiu Manea1,4, Codrut Sarafoleanu1,4 1CESITO Center, “Sfanta Maria” Clinical Hospital, Bucharest, Romania 2Department of Pathology, “Sfanta Maria” Clinical Hospital, Bucharest, Romania 3“Victor Babes” National Institute of Research – Development in the Pathology Domain and Biomedical Sciences, Bucharest, Romania 4ENT&HNS Department, “Sfanta Maria” Clinical Hospital, Bucharest, Romania ABSTRACT BACKGROUND. Neuroendocrine tumors of the larynx represent a rare group of neoplasms characterized by pathological and biological heterogeneity. The histological and immunohistochemical diagnosis is the most important step in the appropri- ate management of these tumors and the prognosis varies according to histological types. Conventional anatomical and func- tional imaging can be complementary for diagnosis, staging and monitoring of treatment response. MATERIAL AND METHODS. Here we report on a case of a laryngeal neuroendocrine small cell carcinoma occurring in a 67-year-old man who was referred to our clinic for clinical reevaluation, diagnosis and treatment. The clinical presentation, the histopathological and immunohistochemical examination and management of this kind of tumor are highlighted. CONCLUSION. Small cell neuroendocrine carcinomas are very aggressive neoplasms. Patients could benefit from surgery, but radiotherapy and chemotherapy remain the treatment of choice. Very low incidence of neuroendocrine tumors in the larynx and specifically very poor prognosis of neuroendocrine small cell carcinoma encouraged an extensive literature review. KEYWORDS: small cell carcinoma, laryngeal, neuroendocrine, prognosis. INTRODUCTION group of neoplasms, which share specific pathological and immunohistochemical features, with prognosis Neuroendocrine neoplasms of the larynx are a het- dependent on the tumor type.