Lung Nodule Clinic, We and Are a Smoker, It Is Very Specialize in Caring for Patients Like You
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Lung Anatomy
Lung anatomy Breathing Breathing is an automatic and usually subconscious process which is controlled by the brain. The brain will determine how much oxygen we require and how fast we need to breathe in order to supply our vital organs (brain, heart, kidneys, liver, stomach and bowel), as well as our muscles and joints, with enough oxygen to carry out our normal daily activities. In order for breathing to be effective we need to use our lungs, breathing muscles and blood system efficiently. This leaflet should help you to better understand the process of breathing and how we get the much needed oxygen into our bodies. The lungs You have two lungs, one in the right side and one in the left side of your chest. The right lung is bigger than the left due to the position of the heart (which is positioned in the left side of the chest). Source: Pulmonary Rehabilitation Reference No: 66354-1 Issue date: 13/2/20 Review date: 13/2/23 Page 1 of 5 Both lungs are covered by 2 thin layers of tissue called the pleura. The pleura stop the surface of the lungs rubbing together as we breathe in and out. The lungs are protected by the ribcage. The airways Within the lungs there is a vast network of airways (tubes) which help to transport the oxygen into the lungs and the carbon dioxide out. These tubes branch into smaller and smaller tubes the further they go into the lungs. Page 2 of 5 Trachea (windpipe): This tube connects your nose and mouth to your lungs. -

Lung Microbiome Participation in Local Immune Response Regulation in Respiratory Diseases
microorganisms Review Lung Microbiome Participation in Local Immune Response Regulation in Respiratory Diseases Juan Alberto Lira-Lucio 1 , Ramcés Falfán-Valencia 1 , Alejandra Ramírez-Venegas 2, Ivette Buendía-Roldán 3 , Jorge Rojas-Serrano 4 , Mayra Mejía 4 and Gloria Pérez-Rubio 1,* 1 HLA Laboratory, Instituto Nacional de Enfermedades Respiratorias Ismael Cosío Villegas, Mexico City 14080, Mexico; [email protected] (J.A.L.-L.); [email protected] (R.F.-V.) 2 Tobacco Smoking and COPD Research Department, Instituto Nacional de Enfermedades Respiratorias Ismael Cosío Villegas, Mexico City 14080, Mexico; [email protected] 3 Translational Research Laboratory on Aging and Pulmonary Fibrosis, Instituto Nacional de Enfermedades Respiratorias Ismael Cosío Villegas, Mexico City 14080, Mexico; [email protected] 4 Interstitial Lung Disease and Rheumatology Unit, Instituto Nacional de Enfermedades Respiratorias Ismael Cosío Villegas, Mexico City 14080, Mexico; [email protected] (J.R.-S.); [email protected] (M.M.) * Correspondence: [email protected]; Tel.: +52-55-5487-1700 (ext. 5152) Received: 11 June 2020; Accepted: 7 July 2020; Published: 16 July 2020 Abstract: The lung microbiome composition has critical implications in the regulation of innate and adaptive immune responses. Next-generation sequencing techniques have revolutionized the understanding of pulmonary physiology and pathology. Currently, it is clear that the lung is not a sterile place; therefore, the investigation of the participation of the pulmonary microbiome in the presentation, severity, and prognosis of multiple pathologies, such as asthma, chronic obstructive pulmonary disease, and interstitial lung diseases, contributes to a better understanding of the pathophysiology. Dysregulation of microbiota components in the microbiome–host interaction is associated with multiple lung pathologies, severity, and prognosis, making microbiome study a useful tool for the identification of potential therapeutic strategies. -

Oncology 101 Dictionary
ONCOLOGY 101 DICTIONARY ACUTE: Symptoms or signs that begin and worsen quickly; not chronic. Example: James experienced acute vomiting after receiving his cancer treatments. ADENOCARCINOMA: Cancer that begins in glandular (secretory) cells. Glandular cells are found in tissue that lines certain internal organs and makes and releases substances in the body, such as mucus, digestive juices, or other fluids. Most cancers of the breast, pancreas, lung, prostate, and colon are adenocarcinomas. Example: The vast majority of rectal cancers are adenocarcinomas. ADENOMA: A tumor that is not cancer. It starts in gland-like cells of the epithelial tissue (thin layer of tissue that covers organs, glands, and other structures within the body). Example: Liver adenomas are rare but can be a cause of abdominal pain. ADJUVANT: Additional cancer treatment given after the primary treatment to lower the risk that the cancer will come back. Adjuvant therapy may include chemotherapy, radiation therapy, hormone therapy, targeted therapy, or biological therapy. Example: The decision to use adjuvant therapy often depends on cancer staging at diagnosis and risk factors of recurrence. BENIGN: Not cancerous. Benign tumors may grow larger but do not spread to other parts of the body. Also called nonmalignant. Example: Mary was relieved when her doctor said the mole on her skin was benign and did not require any further intervention. BIOMARKER TESTING: A group of tests that may be ordered to look for genetic alterations for which there are specific therapies available. The test results may identify certain cancer cells that can be treated with targeted therapies. May also be referred to as genetic testing, molecular testing, molecular profiling, or mutation testing. -

Lung Cancer 2020 Fact Sheet
Lung Cancer 2020 Fact Sheet Lung cancer: the most fatal cancer • The most frequently diagnosed cancer is lung cancer (11.6 percent), followed by female breast (11.6 percent) and colorectal cancers (10.2 percent). • Worldwide lung cancer incidents are on track to increase by 38 percent to 2.89 million by 2030. • Lung cancer is the leading cause of death from cancer at 1.74 million (18.4 percent), followed by colorectal (9.2 percent) and stomach cancers (8.2 percent). • Lung cancer deaths exceed breast cancer mortality for women in 28 countries. • Lung cancer mortality is projected to reach 2.45 million worldwide by 2030, a 39 percent increase since 2018. • About 80 percent of lung cancer deaths are as a result of smoking tobacco. Smokers exposed to other known risk factors such as radon and asbestos are at an even higher risk. • For men, lung cancer is the most prevalent form of cancer, it is third for women. • The five-year cancer survival rate in middle-income countries for all types of lung cancer (19 percent) is lower than many other leading cancer sites, such as the colon (71 percent), breast (85 percent) and prostate (98.9 percent). Treating lung cancer • In lower-income countries, access to care and cost-effective treatments can reduce the human burden and societal impact of lung cancer. • Screening with CT scans compared with chest radiography resulted in a 20 percent reduction in lung cancer-specific deaths, but much cheaper and more accessible methods are needed for low-income settings. • Early-stage lung cancer is treated with curative-intent surgery or radiation therapy. -

Manatee Anatomy and Physiology
Manatee Anatomy and Physiology Grade level: Elementary 5 Subject Area: Biology, Anatomy and Physiology, Marine Biology Duration: Teach: 15 minutes, Activity: 20 minutes, Discussion: 20 minutes. Setting: Classroom Next Generation Sunshine State Standards: Reading: LAFS.5.RI Reading standards for Information text Cluster 3 LAFS.5.RI.3 Writing: LA.B.2.1, LA.B.1.2 Speaking and Listening: Cluster 2 LAFS.5.SL.Z Presentation of Knowledge and Ideas Science: Body of Knowledge Life Science: SC.5.L.14, SC.5.L.15, SC.5.L.17, Body of Knowledge Nature of Science Supporting Idea 1: SC.5.N.1 Practice of Science, Supporting Idea 2:SC.5.N.2 Characteristics of Scientific Knowledge Earth Systems and Patterns: 7SC.E.E.7 Statewide Science Assessment Prompt: How might humans help manatees survive? Objectives: Students will learn about manatee bodies and explain some anatomical and physiological differences between manatees, humans and other animals. Materials: Handouts of basic manatee anatomy, dolphin anatomy & human anatomy, crayons or markers, coloring direction sheet, question worksheet, Quiz sheet Vocabulary: Mammal, endangered species, habitat, conservation, vibrissae, nares, blowhole, flipper, herbivore, omnivore, carnivore. Background/Preparation: Handouts of manatee, dolphin, and human anatomy. Fact sheets comparing and contrasting specific and unique anatomical aspects of each species. Basic manatee fact sheet highlighting personality, limited habitat, endangered status and conservation efforts. Teachers can review the manatee fact sheets, and select points of interest they would most like to incorporate into a lesson. This activity may fit best into the week where the human anatomy lessons are addressed. Teachers can present the information via traditional lecture, group discussion, question and answer session, or doing the coloring activity as the lesson points are addressed, etc. -
Information About Lung Nodules
Information about lung nodules Introduction/procedure You have been informed that you have a nodule (or nodules) in your lung. This is a very common finding and is usually nothing to worry about. Lung nodules are often very small (too small to investigate further) and cause no symptoms. They are often found incidentally whilst having a chest x-ray or CT scan for another condition and do not affect the function of the lungs or interfere with breathing. Once discovered, it’s important to observe the appearance of the nodule(s) over time. This is done by repeating an x-ray or CT scan of your chest at certain intervals. Some nodules can be seen on chest x-ray whilst others require a CT scan to be seen clearly. The interval between the scans or x-rays is usually 3 or 6 months and is determined by your age, whether you smoke and the original size of the nodule(s). It is not the same for everyone, but we follow nationally agreed guidelines. After each scan, the images will be reviewed by the specialist chest team and the nodules measured. You will be informed of the result of the review by telephone 2-3 weeks after the scan. Most lung nodules stay exactly the same size, get smaller or even disappear over time. If a nodule has not increased in size over a series of scans or x-rays, you will be informed that no more follow up is required. Rarely a lung nodule may increase in size. If so, it’s important to determine the nature of the nodule and further investigation will be necessary. -

The Fifth Pulmonary Vein
CASE REPORT Anatomy Journal of Africa. 2016. Vol 5 (2): 704 - 706 The Fifth Pulmonary vein Hilkiah Kinfemichael, Asrat Dawit Correspondence to Hilkiah Kinfemichael, Myungsung Medical College, Addis Ababa, Ethiopia PO Box 14972 Email : [email protected]. ABSTRACT A cadaver in Myungsung Medical College (MMC) had a 3rd pulmonary vein originating from the middle lobe of the right lung. Such anatomical variations are very rare. People with this variation have a total of five pulmonary veins entering left atrium. It has clinical implications especially for thoracic surgeons and radiologists during radiofrequency ablations, lobectomies, valve replacements, pulmonary vein catheterizations, video-assisted thoracic surgery (VATS) and others. Key Words: Anatomy, Variations, Pulmonary veins. INTRODUCTION Two pulmonary veins usually drain oxygenated upper lobe, is formed by the union of blood from each lung to left atrium of the apicoposterior, anterior and lingular veins. The heart. The lobular tributaries lie mainly in the inferior left pulmonary vein, which drains the interlobular septa and two pulmonary veins lower lobe, is formed by the hilar union of two from each lung enter left atrium through two veins, superior and common basal veins. The separate pulmonary ostia on either side. On the right and left pulmonary veins perforate the right lung veins from the apical, anterior and fibrous pericardium and open separately in the posterior part of upper lobe unite with a middle posterosuperior aspect of the left atrium lobar vein, which is formed by lateral and (Standring et al., 2008). This anatomy could medial tributaries, and form the superior right show variations, with more veins draining pulmonary vein (Standring, 2008). -

Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma
cancers Review Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma Fraser Brims 1,2,3 1 Curtin Medical School, Curtin University, Perth, WA 6845, Australia; [email protected] 2 Department of Respiratory Medicine, Sir Charles Gairdner Hospital, Perth, WA 6009, Australia 3 National Centre for Asbestos Related Diseases, Institute for Respiratory Health, Perth, WA 6009, Australia Simple Summary: Mesothelioma is a cancer of the lining of the lungs caused by breathing in asbestos fibres. Asbestos was widely used in industry in the last century in most developed countries and is still present in many older buildings to this day. There is no known safe level of asbestos exposure. Symptoms of mesothelioma can include worsening breathlessness, chest pain and loss of weight. There is no cure, and the treatment of mesothelioma is limited, although there have been some recent improvements in therapy. Survival is very variable although most people live for around one year after diagnosis. Efforts to improve and maintain the quality of life for patients with mesothelioma remain a priority. Abstract: Mesothelioma is a cancer predominantly of the pleural cavity. There is a clear association of exposure to asbestos with a dose dependent risk of mesothelioma. The incidence of mesothelioma in different countries reflect the historical patterns of commercial asbestos utilisation in the last century and predominant occupational exposures mean that mesothelioma is mostly seen in males. Modern imaging techniques and advances in immunohistochemical staining have contributed to an improved diagnosis of mesothelioma. There have also been recent advances in immune checkpoint inhibition, however, mesothelioma remains very challenging to manage, especially Citation: Brims, F. -
The Respiratory System
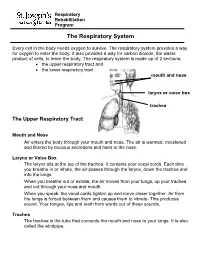
Respiratory Rehabilitation Program The Respiratory System Every cell in the body needs oxygen to survive. The respiratory system provides a way for oxygen to enter the body. It also provides a way for carbon dioxide, the waste product of cells, to leave the body. The respiratory system is made up of 2 sections: the upper respiratory tract and the lower respiratory tract mouth and nose larynx or voice box trachea The Upper Respiratory Tract Mouth and Nose Air enters the body through your mouth and nose. The air is warmed, moistened and filtered by mucous secretions and hairs in the nose. Larynx or Voice Box The larynx sits at the top of the trachea. It contains your vocal cords. Each time you breathe in or inhale, the air passes through the larynx, down the trachea and into the lungs. When you breathe out or exhale, the air moves from your lungs, up your trachea and out through your nose and mouth. When you speak, the vocal cords tighten up and move closer together. Air from the lungs is forced between them and causes them to vibrate. This produces sound. Your tongue, lips and teeth form words out of these sounds. Trachea The trachea is the tube that connects the mouth and nose to your lungs. It is also called the windpipe. The Lower Respiratory Tract Inside Lungs Outside Lungs bronchial tubes alveoli diaphragm (muscle) Bronchial Tubes The trachea splits into 2 bronchial tubes in your lungs. These are called the left bronchus and right bronchus. The bronchus tubes keep branching off into smaller and smaller tubes called bronchi. -

Lung Lobe Segmentation Based on Lung Fissure Surface Classification
algorithms Article Lung Lobe Segmentation Based on Lung Fissure Surface Classification Using a Point Cloud Region Growing Approach Xin Chen 1, Hong Zhao 2 and Ping Zhou 3,* 1 College of Electrical and Information Engineering, Hunan University, Changsha 410082, China; [email protected] 2 College of Aerospace Science and Engineering, National University of Defense Technology, Changsha 410003, China; [email protected] 3 College of Biology, Hunan University, Changsha 410082, China * Correspondence: [email protected] Received: 2 September 2020; Accepted: 13 October 2020; Published: 15 October 2020 Abstract: In anatomy, the lung can be divided by lung fissures into several pulmonary lobe units with specific functions. Identifying the lung lobes and the distribution of various diseases among different lung lobes from CT images is important for disease diagnosis and tracking after recovery. In order to solve the problems of low tubular structure segmentation accuracy and long algorithm time in segmenting lung lobes based on lung anatomical structure information, we propose a segmentation algorithm based on lung fissure surface classification using a point cloud region growing approach. We cluster the pulmonary fissures, transformed into point cloud data, according to the differences in the pulmonary fissure surface normal vector and curvature estimated by principal component analysis. Then, a multistage spline surface fitting method is used to fill and expand the lung fissure surface to realize the lung lobe segmentation. The proposed approach was qualitatively and quantitatively evaluated on a public dataset from Lobe and Lung Analysis 2011 (LOLA11), and obtained an overall score of 0.84. Although our approach achieved a slightly lower overall score compared to the deep learning based methods (LobeNet_V2 and V-net), the inter-lobe boundaries from our approach were more accurate for the CT images with visible lung fissures. -
Small Cell Lung Cancer (SCLC) Algorithm
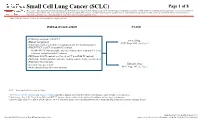
Small Cell Lung Cancer (SCLC) Page 1 of 8 Disclaimer: This algorithm has been developed for MD Anderson using a multidisciplinary approach considering circumstances particular to MD Anderson’s specific patient population, services and structure, and clinical information. This is not intended to replace the independent medical or professional judgment of physicians or other health care providers in the context of individual clinical circumstances to determine a patient's care. This algorithm should not be used to treat pregnant women. Note: Consider Clinical Trials as treatment options for eligible patients. INITIAL EVALUATION STAGE ● Pathology consistent with SCLC Limited Stage ● History and physical AJCC Stage I-III2, see Page 2 ● Laboratory studies to include hematological and full chemistry panels ● FDG PET/CT and CT chest with IV contrast ○ If FDG PET/CT not available: nuclear medicine bone scan and CT chest, abdomen, and pelvis with IV contrast ● MRI brain with IV contrast (preferred) or CT head with IV contrast ● MRI spine, lumbar puncture and bone marrow aspirate/biopsy as indicated ● Pulmonary function tests 1 Extensive Stage ● Lifestyle risk assessment AJCC Stage IV3, see Page 3 ● Molecular profiling (for never smokers) AJCC = American Joint Committee on Cancer 1 See Physical Activity, Nutrition, and Tobacco Cessation algorithms; ongoing reassessment of lifestyle risks should be a part of routine clinical practice 2 Limited stage: Stage I-III (T any, N any, M0) per AJCC 8th edition or disease confined to the ipsilateral hemithorax -

Pathology and Classification of SCLC
cancers Review Pathology and Classification of SCLC Maria Gabriela Raso * , Neus Bota-Rabassedas and Ignacio I. Wistuba * Department of Translational Molecular Pathology, The University of Texas MD Anderson Cancer Center, Houston, TX 77030, USA; [email protected] * Correspondence: [email protected] (M.G.R.); [email protected] (I.I.W.); Tel.: +1-713-834-6026 (M.G.R.); +1-713-563-9184 (I.I.W.) Simple Summary: Small cell lung carcinoma (SCLC), is a high-grade neuroendocrine carcinoma defined by its aggressiveness, poor differentiation, and somber prognosis. This review highlights cur- rent pathological concepts including classification, immunohistochemistry features, and differential diagnosis. Additionally, we summarize the current knowledge of the immune tumor microenvi- ronment, tumor heterogeneity, and genetic variations of SCLC. Recent comprehensive genomic research has improved our understanding of the diverse biological processes that occur in this tumor type, suggesting that a new era of molecular-driven treatment decisions is finally foreseeable for SCLC patients. Abstract: Lung cancer is consistently the leading cause of cancer-related death worldwide, and it ranks as the second most frequent type of new cancer cases diagnosed in the United States, both in males and females. One subtype of lung cancer, small cell lung carcinoma (SCLC), is an aggressive, poorly differentiated, and high-grade neuroendocrine carcinoma that accounts for 13% of all lung carcinomas. SCLC is the most frequent neuroendocrine lung tumor, and it is commonly presented as an advanced stage disease in heavy smokers. Due to its clinical presentation, it is typically diagnosed in small biopsies or cytology specimens, with routine immunostaining only. However, Citation: Raso, M.G.; immunohistochemistry markers are extremely valuable in demonstrating neuroendocrine features of Bota-Rabassedas, N.; Wistuba, I.I.