Pdabu315.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Seasonal Malaria Chemoprevention in Guinea Maya Zhang, Stacy Attah-Poku, Noura Al-Jizawi, Jordan Imahori, Stanley Zlotkin
Seasonal Malaria Chemoprevention in Guinea Maya Zhang, Stacy Attah-Poku, Noura Al-Jizawi, Jordan Imahori, Stanley Zlotkin April 2021 This research was made possible through the Reach Alliance, a partnership between the University of Toronto’s Munk School of Global Affairs & Public Policy and the Mastercard Center for Inclusive Growth. Research was also funded by the Ralph and Roz Halbert Professorship of Innovation at the Munk School of Global Affairs & Public Policy. We express our gratitude and appreciation to those we met and interviewed. This research would not have been possible without the help of Dr. Paul Milligan from the London School of Hygiene and Tropical Medicine, ACCESS-SMC, Catholic Relief Services, the Government of Guinea and other individuals and organizations in providing and publishing data and resources. We are also grateful to Dr. Kovana Marcel Loua, director general of the National Institute of Public Health in Guinea and professor at the Gamal Abdel Nasser University of Conakry, Guinea. Dr. Loua was instrumental in the development of this research — advising on key topics, facilitating ethics board approval in Guinea and providing data and resources. This research was vetted by and received approval from the Ethics Review Board at the University of Toronto. Research was conducted during the COVID-19 pandemic in compliance with local public health measures. MASTERCARD CENTER FOR INCLUSIVE GROWTH The Center for Inclusive Growth advances sustainable and equitable economic growth and financial inclusion around the world. Established as an independent subsidiary of Mastercard, we activate the company’s core assets to catalyze action on inclusive growth through research, data philanthropy, programs, and engagement. -

Cloth, Commerce and History in Western Africa 1700-1850
The Texture of Change: Cloth, Commerce and History in Western Africa 1700-1850 The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters Citation Benjamin, Jody A. 2016. The Texture of Change: Cloth, Commerce and History in Western Africa 1700-1850. Doctoral dissertation, Harvard University, Graduate School of Arts & Sciences. Citable link http://nrs.harvard.edu/urn-3:HUL.InstRepos:33493374 Terms of Use This article was downloaded from Harvard University’s DASH repository, and is made available under the terms and conditions applicable to Other Posted Material, as set forth at http:// nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of- use#LAA The Texture of Change: Cloth Commerce and History in West Africa, 1700-1850 A dissertation presented by Jody A. Benjamin to The Department of African and African American Studies in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the subject of African and African American Studies Harvard University Cambridge, Massachusetts May 2016 © 2016 Jody A. Benjamin All rights reserved. Dissertation Adviser: Professor Emmanuel Akyeampong Jody A. Benjamin The Texture of Change: Cloth Commerce and History in West Africa, 1700-1850 Abstract This study re-examines historical change in western Africa during the eighteenth and nineteenth centuries through the lens of cotton textiles; that is by focusing on the production, exchange and consumption of cotton cloth, including the evolution of clothing practices, through which the region interacted with other parts of the world. It advances a recent scholarly emphasis to re-assert the centrality of African societies to the history of the early modern trade diasporas that shaped developments around the Atlantic Ocean. -
PRSP II) for Guinea and the Public Disclosure Authorized Joint IDA-IMF Staff Advisory Note (JSAN) on the PRSP II
OFFICIAL USE ONLY IDA/SecM2007-0684 December 12, 2007 Public Disclosure Authorized For meeting of Board: Tuesday, January 8, 2008 FROM: Vice President and Corporate Secretary Guinea: Second Poverty Reduction Strategy Paper and Joint IDA-IMF Staff Advisory Note 1. Attached is the Second Poverty Reduction Strategy Paper (PRSP II) for Guinea and the Public Disclosure Authorized Joint IDA-IMF Staff Advisory Note (JSAN) on the PRSP II. The IMF is currently scheduled to discuss this document on December 21, 2007. 2. The PRSP II was prepared by the Government of Guinea. The paper acknowledges the disappointing outcome of the first PRSP, which covered the period 2002-2006. The political, social and economic environment in which the implementation of PRSP I took place was characterized by poor governance, political instability, and low growth which led to an increase in poverty from 49 percent in 2002 to an estimated 54 percent in 2005. Overall, public service delivery deteriorated in terms of both quality and access and the living conditions for most Guineans worsened. Public Disclosure Authorized 3. PRSP II aims at recapturing lost ground over the past five years. The overall strategy is based on three pillars: (i) improving governance; (ii) accelerating growth and increasing employment opportunities; and (iii) improving access to basic services. It focuses on restoring macroeconomic stability, institutional and structural reforms, and mechanisms to strengthen the democratic process implementation capacity. 4. As approved by the Board on August 6, 2007, the pilot Board Technical Questions and Answer Database (http://boardqa.worldbank.org or from the EDs' portal) is now open for questions. -

Appraisal Report Kankan-Kouremale-Bamako Road Multinational Guinea-Mali
AFRICAN DEVELOPMENT FUND ZZZ/PTTR/2000/01 Language: English Original: French APPRAISAL REPORT KANKAN-KOUREMALE-BAMAKO ROAD MULTINATIONAL GUINEA-MALI COUNTRY DEPARTMENT OCDW WEST REGION JANUARY 1999 SCCD : N.G. TABLE OF CONTENTS Page PROJECT INFORMATION BRIEF, EQUIVALENTS, ACRONYMS AND ABBREVIATIONS, LIST OF ANNEXES AND TABLES, BASIC DATA, PROJECT LOGICAL FRAMEWORK, ANALYTICAL SUMMARY i-ix 1 INTRODUCTION.............................................................................................................. 1 1.1 Project Genesis and Background.................................................................................... 1 1.2 Performance of Similar Projects..................................................................................... 2 2 THE TRANSPORT SECTOR ........................................................................................... 3 2.1 The Transport Sector in the Two Countries ................................................................... 3 2.2 Transport Policy, Planning and Coordination ................................................................ 4 2.3 Transport Sector Constraints.......................................................................................... 4 3 THE ROAD SUB-SECTOR .............................................................................................. 5 3.1 The Road Network ......................................................................................................... 5 3.2 The Automobile Fleet and Traffic................................................................................. -
Guinea: Reference Map of Faranah Prefecture (As of 05 March 2015)
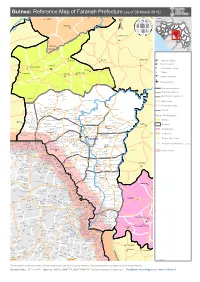
Guinea: Reference Map of Faranah Prefecture (as of 05 March 2015) Kalinko SENEGAL MALI GUINEA Sélouma BISSAU GUINEA Komola Koura COTE D'IVOIRE SIERRA LEONE Dialakoro Kankama LIBERIA Sisséla Sanguiana Bissikirima Regional Capital District Capital Dabola Arfamoussayah Sub District Capital Banko Kounendou Village Dogomet N'demba Unpaved runway Paved runway Region boundaries Koulambo District boundaries Morigbeya Dar Es Salam Daro Gada Walan Sub District boundaries Kindoyé DIGUILA CENTRE Fabouya TOUMANIA CENTRE Boubouya Main roads Yombo Nialen Moria Dansoya Secondary roads NIENOUYA CENTRE Teliayaga Doukou Passaya Souriya Mansira Moribaya KONDEBOU KASSA BOUNA CENTRE Tambaya Rivers Foya Gadha Mongoli Babakadia Hafia Gomboya BELEYA CENTRE SABERE KALIA Keema SOUNGBANYA CENTRE Balandou Beindougou SANSANKO CENTRE Sidakoro Gueagbely Gueafari Sokora District (Préfectures) Harounaya Miniandala Badhi Gnentin Oussouya Banire Wolofouga Lamiya Gueagbely Mameyire SANSAMBOU CENTRE BIRISSA CENTRE NGUENEYA CENTRE NIAKO CENTRE Koumandi Koura Dabola Wassakaria Kobalen Bingal Dansoya Tomata Konkofaya Heredou Marela karimbou Sansamba Bouran SOLOYA CENTRE Kolmatamba KOUMANDI KORO Sanamoussaya MILIDALA CENTRE Banfele Labatara Gninantamba BONTALA Koura Sambouya DIANA CENTRE Sansando Faranah Wossekalia FRIGUIA CENTRE MAGNA Halossagoya KALIA CENTRE I KOMBONYA Ballayany Herewa Alia Filly Fore Sakoromaya SOLONYEREYA Khamaya Bindou Dansaya Koutamodiya Salia Kamako Kissidougou Goulouya Fantoumaniya Nerekoro SEREKORO CENTRE Guidonya Kombonyady Wassambala Balankhamba Kabaya -

For Personal Use Only Use Personal For
Mt Edon House 2nd Floor,West Apartment, Hse 2/7 Inner Road, 30 Ledgar Rd Immeuble Archêvèche, Cantonments, Accra Balcatta WA Conakry Ghana Australia Républic De Guinée P. +233 021 782348 P. +61 8 9240 7660 B.P. 3938 Conakry F. +61 8 9240 2406 Républic De Guinée A.B.N. 14 113 517 203 P. +8821 621 153 527 www.bureygold.com 29 April 2011 MARCH 2011 QUARTERLY ACTIVITY REPORT HIGHLIGHTS Balatindi Project • A total of 10 sub-vertical HQ diamond drill holes were completed for a total of 3,468.6 metres. • An additional 22 reverse circulation (RC) drill holes for 1,848 metres tested the substrate of five areas, designated anomalies A to E, of substantial surface radiometric anomalism and associated alteration. Kossanke Project • Refurbishment of the previous field camp, Farassabeben, on the Kossanke Licence area is currently in progress. • Executed an agreement with local company Societe Bossoba sarlu allowing Burey to earn an 80% interest in the Celein exploration licence, Mandiana Prefecture, Guinea Post Period Highlights • By the end of April 2011, Burey had completed approximately 25% of a 7,000m RC infill and extension program at the Mansounia Project in 15 RC drill holes for approximately 1,500 metres. • Contracted exploration consulting group SEMS Exploration Services, which has started preparatory logistics work to allow commencement of a soil sampling program at the Kossanke and Celein Licences in May. • It is anticipated that all assay results for gold and the associated multi-element ICP MS analytical process which have been returned to date (with most of the polymetallic ICP results still awaited) from the initial six holes of the ten hole programme which investigated the Balatindi polymetallic occurrence, will be released in early May. -

2.3.16 Guinea Border Crossing of Heremakonon
2.3.16 Guinea Border Crossing of Heremakonon Overview Daily Capacity Customs Clearance Other Relevant Information Overview Hérémakonon is a town and sub-prefecture in the Faranah Prefecture in the Faranah Region of Guinea. As of 2014 it had a population of 12,890 people. The road is not paved and it is very difficult to access during the rainy season. BORDER CROSSING LOCATION & CONTACT Name of Border Crossing Heremakonon [Guinea] Gberia Fotombu [Sierra Leone] Province or District Nzerekore / Faranah Nearest Town or City Faranah 44 km Latitude 9.718564 Longitude -11.00049 Managing Authority/Agency Customs Authority Contact Person N/A Travel Times Nearest International Airport Gbessia International Airport 420 km Truck: 8 hours Car: 6 hours Nearest Port Port Autonome of Conakry 430 km Truck: 8 hours Car: 6 hours Nearest Major Market Faranah 44 km Truck: 2 hours Car: 1 hour Other Information There are no weighing bridges en-route. Hours of Operation MONDAYS 0800 - 1830 TUESDAYS 0800 - 1830 WEDNESDAYS 0800 - 1830 THURSDAYS 0800 - 1830 Page 1 FRIDAYS 0800 - 1830 SATURDAYS 0800 - 1830 SUNDAYS 0800 - 1830 NATIONAL HOLIDAYS 0800 - 1830 SEASONAL CONSTRAINTS Rainy season Daily Capacity The borders were closed during the Ebola outbreak in 2014/2015. Private cars are not provided a separate lane. Customs Clearance In order to obtain a customs clearance, all the documents should be prepared and approved by the Customs authority in Conakry, then transmitted to the regional customs office respectively. A copy should be made available at the border post by the requester/transporter. The waybill and commercial invoice are the main documents requested by the customs at the border. -

REPUBLIC of GUINEA Labor–Justice–Solidarity
REPUBLIC OF GUINEA Labor–Justice–Solidarity MINISTRY OF AGRICULTURE AND LIVESTOCK NATIONAL STRATEGY FOR THE DEVELOPMENT OF RICE GROWING APRIL 2009 Table of contents LIST OF ACRONYMS AND ABBREVIATIONS 5 SUMMARY 6 I. INTRODUCTION 8 II. REVIEWING THE RICE SECTOR 9 2.1. The policy position of rice 10 2.2 Preferences and demand estimates 10 2.3 Typology and number of rice farmers, processors and marketers 11 2.4. Gender dimensions 13 2.5. Comparative advantage of national rice production 14 III. CHALLENGES AND OPPORTUNITIES 14 3.1. The potential of local rice for rural poverty reduction and economic growth 14 3.2. The land system 15 3.3. Social issues 16 3.4. Trans-border and regional issues 16 3.5. Knowledge and lessons learnt from R&D in rice 16 VI. PRIORITY AREAS AND PERSPECTIVES 17 4.1. Ranking by order of priority in terms of potential contribution to national production 17 4.2. Identification and ranking specific environmental challenges and related opportunities by order of priority 18 4.3. Identification of policy challenges/opportunities 20 4.3.1. Policy challenges 20 4.3.1. Opportunities 21 V. VISION AND FRAMEWORK OF THE NATIONAL RICE STRATEGY 21 5.1. Objectives of rice production 21 5.5.1. Overall target: 21 5.5.2. Quantified objectives: 21 5.2.3. Strategy development phase 23 5.2.4. Key interventions 24 5.2.5 Scientists, technicians and agricultural advisory agents in 2008 and beyond 25 5.2.6. Governance of the Rice Growing Development Strategy 25 5.2.7. -
MCHIP Guinea End-Of-Project Report October 2010–June 2014
MCHIP Guinea End-of-Project Report October 2010–June 2014 Submitted on: September 15, 2014 Submitted to: United States Agency for International Development under Coooperative Agreement # GHS-A-00-08-00002-000 Submitted by: Yolande Hyjazi, Rachel Waxman and Bethany Arnold 1 The Maternal and Child Health Integrated Program (MCHIP) is the USAID Bureau for Global Health’s flagship maternal, neonatal and child health (MNCH) program. MCHIP supports programming in maternal, newborn and child health, immunization, family planning, malaria, nutrition, and HIV/AIDS, and strongly encourages opportunities for integration. Cross-cutting technical areas include water, sanitation, hygiene, urban health and health systems strengthening. MCHIP brings together a partnership of organizations with demonstrated success in reducing maternal, newborn and child mortality rates and malnutrition. Each partner will take the lead in developing programs around specific technical areas: Jhpiego, as the Prime, will lead maternal health, family planning/reproductive health, and prevention of mother-to-child transmission of HIV (PMTCT); JSI—child health, immunization, and pediatric AIDS; Save the Children—newborn health, community interventions for MNCH, and community mobilization; PATH—nutrition and health technology; JHU/IIP—research and evaluation; Broad Branch—health financing; PSI—social marketing; and ICF International—continues support for the Child Survival and Health Grants Program (CSHGP) and the Malaria Communities Program (MCP). This report was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Leader with Associates Cooperative Agreement GHS-A-00-08-00002-00. The contents are the responsibility of the Maternal and Child Health Integrated Program (MCHIP) and do not necessarily reflect the views of USAID or the United States Government. -
Community Development Funds and Agreements in Guinea Under the New Mining Code
Community Development Funds and Agreements in Guinea Under the New Mining Code June 2013 With support from: 1 This report was prepared as part of a project, funded by AngloGold Ashanti (AGA), in which the Earth Institute at Columbia University, in partnership with Millennium Promise, worked with local governments and communities around the gold mines in Northern Guinea to formulate integrated MDG-based local development plans. In addition, the Columbia Center on Sustainable Investment (CCSI), a joint Center of Columbia Law School and the Earth Institute, assessed the legal and fiscal framework for investments in gold in the region to better understand the total impact of and contribution to development of this sector. This report forms part of that analysis: specifically looking at how revenues from the mines could support local development plans. At the time of the drafting, in mid-2013, the Government of Guinea was formulating new regulations to govern how resource revenues would fund local development. The purpose of this report is to serve as the basis for discussion and consultation between the Government of Guinea and its development partners in the public and private sector as the regulations are being finalized; the report helps to shed light on relevant aspects of the legal framework to-date, including how they have operated in practice, and shares models and good practices of community development agreements and community development funds from elsewhere in the world. This is a work product of CCSI and does not necessarily reflect the views of any other organizations or partners in the Northern Guinea projects, including the Government of Guinea and Anglo Gold Ashanti. -

West Africa – Ebola Outbreak Fact Sheet #27, Fiscal Year (Fy) 2015 March 31, 2015
WEST AFRICA – EBOLA OUTBREAK FACT SHEET #27, FISCAL YEAR (FY) 2015 MARCH 31, 2015 NUMBERS AT HIGHLIGHTS USG HUMANITARIAN ASSISTANCE TO EVD OUTBREAK RESPONSE A GLANCE TO DATE IN FY 2014 & FY 2015 Last confirmed EVD case dies in 25,178 Liberia; no new confirmed cases USAID/OFDA1 $515,176,019 detected since March 20 USAID/FFP2 $57,479,546 Number of Suspected, Sierra Leone’s three-day stay-at-home Probable, and Confirmed USAID/GH3 $20,076,000 Ebola Virus Disease (EVD) period occurs with widespread Cases in Acutely Affected compliance USAID/Liberia $16,100,000 Countries* President of Guinea Alpha Condé USAID/Guinea $3,482,000 UN World Health Organization declares a 45-day health emergency (WHO) – DoD4 $360,255,000 March 31, 2015 period; closes border between Guinea and Sierra Leone CDC5 $391,576,1366 10,445 $1,364,144,701 Number of EVD-Related USG ASSISTANCE TO THE WEST AFRICA 7 Deaths* EVD OUTBREAK RESPONSE WHO – March 31, 2015 KEY DEVELOPMENTS 11,974 The Government of Sierra Leone (GoSL) enacted a three-day stay-at-home period on March Number of EVD Cases in 27–29. Approximately 8,300 three-person teams—each comprising a nurse, a social Sierra Leone* mobilizer, and a community task force member—went door-to-door to distribute soap, WHO – March 31, 2015 promote good hygiene practices, and identify possible EVD cases. The GoSL National Ebola Response Center (NERC) reported that teams focused on EVD hotspot areas and did not 9,712 deploy to four districts that have no current active transmission chains. -

West Africa – Ebola Outbreak Fact Sheet #23, Fiscal Year (Fy) 2015 March 4, 2015
WEST AFRICA – EBOLA OUTBREAK FACT SHEET #23, FISCAL YEAR (FY) 2015 MARCH 4, 2015 NUMBERS AT HIGHLIGHTS USG HUMANITARIAN ASSISTANCE A GLANCE TO EVD OUTBREAK RESPONSE WHO reports 132 new confirmed cases of TO DATE IN FY 2014 & FY 2015 EVD in Guinea and Sierra Leone in the 23,934 week ending on March 1. USAID/OFDA1 $463,846,949 No new EVD cases confirmed in Liberia USAID/FFP2 $57,479,546 Number of Suspected, in nearly two weeks. Probable, and Confirmed USAID/GH3 $20,076,000 Ebola Virus Disease (EVD) Response actors remain concerned Cases in Acutely Affected regarding ongoing EVD transmission USAID/Liberia $16,100,000 Countries* chains in Guinea’s Forécariah Prefecture, USAID/Guinea $3,482,000 UN World Health Organization where 23 EVD cases since February 28— (WHO) – DoD4 $353,958,000 March 4, 2015 more than 70 percent of the 32 confirmed cases in the same time period CDC5 $131,455,1156 countrywide—have occurred. 9,792 $1,046,397,610 Number of EVD-Related USG ASSISTANCE TO THE WEST AFRICA 7 Deaths* EVD OUTBREAK RESPONSE WHO – March 4, 2015 KEY DEVELOPMENTS 11,466 As of March 3, the Government of Liberia (GoL) Incident Management System (IMS) had Number of EVD Cases in not reported a confirmed case of EVD in 12 days, with the most recent case documented in Sierra Leone* Montserrado County on February 19. On February 27, the IMS announced that Liberia had WHO – March 4, 2015 entered Phase 3 of the EVD response, which will focus on restoring non-EVD health services and improving triage and referral processes to enable medical staff to safely identify and isolate suspect EVD cases.