Learning from Safe Male Circumcision Project in Kayunga District
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

DISTRICT BASELINE: Nakasongola, Nakaseke and Nebbi in Uganda
EASE – CA PROJECT PARTNERS EAST AFRICAN CIVIL SOCIETY FOR SUSTAINABLE ENERGY & CLIMATE ACTION (EASE – CA) PROJECT DISTRICT BASELINE: Nakasongola, Nakaseke and Nebbi in Uganda SEPTEMBER 2019 Prepared by: Joint Energy and Environment Projects (JEEP) P. O. Box 4264 Kampala, (Uganda). Supported by Tel: +256 414 578316 / 0772468662 Email: [email protected] JEEP EASE CA PROJECT 1 Website: www.jeepfolkecenter.org East African Civil Society for Sustainable Energy and Climate Action (EASE-CA) Project ALEF Table of Contents ACRONYMS ......................................................................................................................................... 4 ACKNOWLEDGEMENT .................................................................................................................... 5 EXECUTIVE SUMMARY .................................................................................................................. 6 CHAPTER ONE: INTRODUCTION ................................................................................................. 8 1.1 Background of JEEP ............................................................................................................ 8 1.2 Energy situation in Uganda .................................................................................................. 8 1.3 Objectives of the baseline study ......................................................................................... 11 1.4 Report Structure ................................................................................................................ -
Kayunga District Statistical Abstract for 2017/2018
Kayunga District Statistical Abstract for 2017/2018 THE REPUBLIC OF UGANDA KAYUNGA DISTRICT LOCAL GOVERNMENT STATISTICAL ABSTRACT 2017/18 Kayunga District Local Government P.O Box 18000, Kayunga Tel: +256-xxxxxx September 2018 E-mail: [email protected] Website: www.Kayunga.go.ug i Kayunga District Statistical Abstract for 2017/2018 TABLE OF CONTENTS TABLE OF CONTENTS .................................................................................................................... II LIST OF TABLES .............................................................................................................................. V FOREWORD .................................................................................................................................. VIII ACKNOWLEDGEMENT ................................................................................................................... IX LIST OF ACRONYMS ....................................................................................................................... X GLOSSARY ..................................................................................................................................... XI EXECUTIVE SUMMARY ................................................................................................................ XIII GENERAL INFORMATION ABOUT THE DISTRICT ..................................................................... XVI CHAPTER 1: BACKGROUND INFORMATION ................................................................................ -

Profit Making for Smallholder Farmers Proceedings of the 5Th MATF Experience Sharing Workshop 25Th - 29Th May 2009, Entebbe, Uganda
Profit Making for Smallholder Farmers Proceedings of the 5th MATF Experience Sharing Workshop 25th - 29th May 2009, Entebbe, Uganda Profit Making for Small Holder Farmers 1 Charles Katusabe with his cow he G.ilbert/MATF : purchased from his garlic income Photo 2 MATF 5th Grant Holders’ Workshop Profit Making for Smallholder Farmers Proceedings of the 5th MATF Experience Sharing Workshop 25th - 29th May 2009, Entebbe, Uganda Editors: Dr. Ralph Roothaert and Gilbert Muhanji Workshop organisers: Chris Webo, Fatuma Buke, Gilbert Muhanji, Monicah Nyang, Dr. Ralph Roothaert and Renison Kilonzo. Preferred citation: R. Roothaert and G. Muhanji (Eds), 2009. Profit Making for Smallholder Farmers. Proceedings of the 5th MATF Experience Sharing Workshop, 25th - 29th May 2009, Entebbe, Uganda. FARM-Africa, Nairobi, 44 pp. This book is an output of the Maendeleo Agricultural Technology Fund (MATF), with joint funding from the Rockefeller Foundation and the Gatsby Charitable Foundation since 2002, and funded by the Kilimo Trust since 2005. The views expressed are not necessarily those of the Kilimo Trust as the contents are solely the responsibility of the authors. MATF is managed by the Food and Agricultural Research Management (FARM)-Africa. © Food and Agricultural Research Management (FARM)-Africa, 2009 Profit Making for Small Holder Farmers 1 Contents Executive summary 3 Acknowledgement 5 Abbreviations and acronyms 6 1.0 INTRODUCTION 7 1.1 FARM-Africa and MATF 7 1.2 Round V 8 1.3 The workshop 9 1.4 Highlights from minister’s speech 10 2.0 PROJECT -
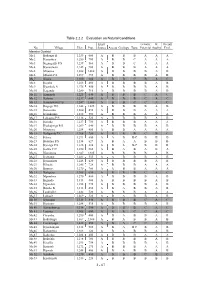
Table 2.2.2 Evaluation on Natural Conditions
Table 2.2.2 Evaluation on Natural Conditions Exist. G-water W. Overall No. Village Elev. Pop. Source Access Geology Topo. Potential Auality Eval. Masaka Destrict Ma 1 Bukango B 1,239 600 A B B B A A A Ma 2 Kasambya 1,250 700 A B B C A A A Ma 3 Kigangazzi P/S 1,239 560 A B B C A A A Ma 4 Kyawamala 1,245 900 A B B B A A A Ma 5 Mijunwa 1,208 1,060 A B B B B A B Ma 6 Mbirizi P/S 1,299 455 A B B B B A B Ma 7 Kisala 1,300 380 A B B C B A C Ma 8 Kigaba 1,206 400 A B B B B A B Ma 9 Kyankole A 1,276 450 A B B B B A B Ma 10 Kagando 1,280 710 A B B B B A B Ma 11 Kamanda 1,225 640 A B B B C A C Ma 12 Katoma 1,217 440 A B B B C A C Ma 13 Kassebwavu P/S 1,247 1,000 A B B C C A C Ma 14 Kagogo H/C 1,248 1,025 A B B B B A B Ma 15 Buwembo 1,280 490 A B B B A A A Ma 16 Kyankonko 1,272 590 A B B B A A A Ma 17 Lukaawa P/S 1,316 520 A B B B B A B Ma 18 Kirinda 1,237 750 A B B B A A A Ma 19 Kyakajwiga P/S 1,209 640 A B B B B A B Ma 20 Miteteero 1,258 480 A B B A A A A Ma 21 Kaligondo T/C 1,308 780 A B B B C B C Ma 22 Kitwa 1,291 600 A A B B-C B B B Ma 23 Bbuuliro P/S 1,134 627 A B A A B B B Ma 24 Kyesiga P/S 1,228 888 A B A B-C B B B Ma 25 Katwe T/C 1,250 380 A B A B A B A Ma 26 Nsangamo 1,287 1,485 A B B B B A B Ma 27 Kyetume 1,281 535 A A B B B A B Ma 28 Kyamakata 1,248 620 A B B B B A B Ma 29 Kibaale 1,246 728 A B B B A A A Ma 30 Bunyere 1,270 780 A A B B A A A Ma 31 Kalegero 1,305 620 A B B B C A C Ma 32 Mpembwe 1,270 400 A B B B B A B Ma 33 Bigando 1,313 400 A B B B B A B Ma 34 Ngondati 1,258 775 A B B B B A B Ma 35 Busibo B 1,313 455 A B A B B A B Ma -

WHO UGANDA BULLETIN February 2016 Ehealth MONTHLY BULLETIN
WHO UGANDA BULLETIN February 2016 eHEALTH MONTHLY BULLETIN Welcome to this 1st issue of the eHealth Bulletin, a production 2015 of the WHO Country Office. Disease October November December This monthly bulletin is intended to bridge the gap between the Cholera existing weekly and quarterly bulletins; focus on a one or two disease/event that featured prominently in a given month; pro- Typhoid fever mote data utilization and information sharing. Malaria This issue focuses on cholera, typhoid and malaria during the Source: Health Facility Outpatient Monthly Reports, Month of December 2015. Completeness of monthly reporting DHIS2, MoH for December 2015 was above 90% across all the four regions. Typhoid fever Distribution of Typhoid Fever During the month of December 2015, typhoid cases were reported by nearly all districts. Central region reported the highest number, with Kampala, Wakiso, Mubende and Luweero contributing to the bulk of these numbers. In the north, high numbers were reported by Gulu, Arua and Koti- do. Cholera Outbreaks of cholera were also reported by several districts, across the country. 1 Visit our website www.whouganda.org and follow us on World Health Organization, Uganda @WHOUganda WHO UGANDA eHEALTH BULLETIN February 2016 Typhoid District Cholera Kisoro District 12 Fever Kitgum District 4 169 Abim District 43 Koboko District 26 Adjumani District 5 Kole District Agago District 26 85 Kotido District 347 Alebtong District 1 Kumi District 6 502 Amolatar District 58 Kween District 45 Amudat District 11 Kyankwanzi District -

Chased Away and Left to Die
Chased Away and Left to Die How a National Security Approach to Uganda’s National Digital ID Has Led to Wholesale Exclusion of Women and Older Persons ! ! ! ! ! ! ! ! ! ! Publication date: June 8, 2021 Cover photo taken by ISER. An elderly woman having her biometric and biographic details captured by Centenary Bank at a distribution point for the Senior Citizens’ Grant in Kayunga District. Consent was obtained to use this image in our report, advocacy, and associated communications material. Copyright © 2021 by the Center for Human Rights and Global Justice, Initiative for Social and Economic Rights, and Unwanted Witness. All rights reserved. Center for Human Rights and Global Justice New York University School of Law Wilf Hall, 139 MacDougal Street New York, New York 10012 United States of America This report does not necessarily reflect the views of NYU School of Law. Initiative for Social and Economic Rights Plot 60 Valley Drive, Ministers Village Ntinda – Kampala Post Box: 73646, Kampala, Uganda Unwanted Witness Plot 41, Gaddafi Road Opp Law Development Centre Clock Tower Post Box: 71314, Kampala, Uganda 2 Chased Away and Left to Die ACKNOWLEDGMENTS This report is a joint publication by the Digital Welfare State and Human Rights Project at the Center for Human Rights and Global Justice (CHRGJ) based at NYU School of Law in New York City, United States of America, the Initiative for Social and Economic Rights (ISER) and Unwanted Witness (UW), both based in Kampala, Uganda. The report is based on joint research undertaken between November 2020 and May 2021. Work on the report was made possible thanks to support from Omidyar Network and the Open Society Foundations. -
Poverty Map Report
Poverty Maps of Uganda Mapping the Spatial Distribution of Poor Households and Child Poverty Based on Data from the 2016/17 Uganda National Household Survey and the 2014 National Housing and Population Census Technical Report October 2019 1 Acknowledgement This technical report presents the results of the Uganda poverty map update exercise, which was conducted by the Uganda Bureau of Statistics (UBOS) in close collaboration with UNICEF and the World Bank. The core task team at UBOS consisted of Mr. James Muwonge (Director of Socio-Economic Surveys), Mr. Justus Bernard Muhwezi (Manager of Geo-Information Services), Mr. Stephen Baryahirwa (Principal Statistician and Head of the Household Surveys Unit), Mr. Vincent Ssennono (Principal Statistician and Head of the Methodology and Analysis Unit), and Mr. Adriku Charles (Senior Geo-Information Officer). The core task team at the World Bank consisted of Dr. Nobuo Yoshida (Lead Economist), Dr. Carolina Mejia-Mantilla (Uganda Country Poverty Economist), Dr. Minh Cong Nguyen (Senior Economist) and Ms. Miyoko Asai (Consultant). Dr. Nobuo Yoshida and Dr. Minh Cong Nguyen supervised the exercise and ensured that the latest international experience and technical innovations were available to the team. The core task team in UNICEF consisted of Dr. Diego Angemi (Chief Social Policy and Advocacy), Mr. Arthur Muteesasira (Information Management and GIS Officer), and Ms. Sarah Kabaija (Monitoring and Evaluation Specialist). The team benefited from the support and guidance provided by Dr. Robin D. Kibuka(Chairman of the Board, UBOS), Ms. Doreen Mulenga (Country Representative, UNICEF), Mr. Antony Thompson (Country Manager, World Bank), and Dr. Pierella Paci (Practice Manager, World Bank). -

Kayunga DLG.Pdf
Local Government Workplan Vote: 523 Kayunga District Structure of Workplan Foreword Executive Summary A: Revenue Performance and Plans B: Summary of Department Performance and Plans by Workplan C: Draft Annual Workplan Outputs for 2016/17 D: Details of Annual Workplan Activities and Expenditures for 2016/17 Page 1 Local Government Workplan Vote: 523 Kayunga District Foreword Page 2 Local Government Workplan Vote: 523 Kayunga District Executive Summary Revenue Performance and Plans 2015/16 2016/17 Approved Budget Receipts by End Proposed Budget Dec UShs 000's 1. Locally Raised Revenues 806,526 440,275 1,117,379 2a. Discretionary Government Transfers 3,811,918 1,306,119 3,548,991 2b. Conditional Government Transfers 18,803,947 9,129,257 22,425,677 2c. Other Government Transfers 1,057,192 328,999 396,948 3. Local Development Grant 380,387 0 4. Donor Funding 812,000 495,577 1,005,438 Total Revenues 25,291,583 12,080,615 28,494,434 Revenue Performance in 2015/16 The District received Shs 6,388,894,000/=; Shs 219,641,000/= Local revenue; 4,894,086,000 Central government transfers; Shs 618,080,000/=, direct transfers from Ministry of Finance, Shs 179,236,000 grants from Other government Agencies and 319,563,000/= was from donor agency. Most grants performed above 20% apart from the Other Government Transfers which was at 17%. Planned Revenues for 2016/17 The District has planned this FY 2016/17 to receive more fund s compared to last FY 2015/16. This is because of an estimated increase in the locally raised revenues,central Government transfers and donor funded projects.This increment is due to Government’s commitment to fulfil the 15% Teacher’s pay rise, increase development funding to the LLGs, and have retiring staff and already existing Pensioners receive their entitlements as well as facilitating Local Government political leaders to fulfil their mandate.Also, more resources have been provided for transitional grants to cater for IFMS and the Construction of the District Building block. -

Uganda Road Fund Annual Report FY 2011-12
ANNUAL REPORT 2011-12 Telephone : 256 41 4707 000 Ministry of Finance, Planning : 256 41 4232 095 & Economic Development Fax : 256 41 4230 163 Plot 2-12, Apollo Kaggwa Road : 256 41 4343 023 P.O. Box 8147 : 256 41 4341 286 Kampala Email : [email protected] Uganda. Website : www.finance.go.ug THE REPUBLIC OF UGANDA In any correspondence on this subject please quote No. ISS 140/255/01 16 Dec 2013 The Clerk to Parliament The Parliament of the Republic of Uganda KAMPALA. SUBMISSION OF UGANDA ROAD FUND ANNUAL REPORT FOR FY 2010/11 In accordance with Section 39 of the Uganda Road Act 2008, this is to submit the Uganda Road Fund Annual performance report for FY 2011/12. The report contains: a) The Audited accounts of the Fund and Auditor General’s report on the accounts of the Fund for FY 2011/12; b) The report on operations of the Fund including achievements and challenges met during the period of reporting. It’s my sincere hope that future reports shall be submitted in time as the organization is now up and running. Maria Kiwanuka MINISTER OF FINANCE, PLANNING AND ECONOMIC DEVELOPMENT cc: The Honourable Minister of Works and Transport cc: The Honourable Minister of Local Government cc: Permanent Secretary/ Secretary to the Treasury cc: Permanent Secretary, Ministry of Works and Transport cc: Permanent Secretary Ministry of Local Government cc: Permanent Secretary Office of the Prime Minister cc: Permanent Secretary Office of the President cc: Chairman Uganda Road Fund Board TABLE OF CONTENTS Abbreviations and Acronyms iii our vision iv -

Funding Going To
% Funding going to Funding Country Name KP‐led Timeline Partner Name Sub‐awardees SNU1 PSNU MER Structural Interventions Allocated Organizations HTS_TST Quarterly stigma & discrimination HTS_TST_NEG meetings; free mental services to HTS_TST_POS KP clients; access to legal services PrEP_CURR for KP PLHIV PrEP_ELIGIBLE Centro de Orientacion e PrEP_NEW Dominican Republic $ 1,000,000.00 88.4% MOSCTHA, Esperanza y Caridad, MODEMU Region 0 Distrito Nacional Investigacion Integral (COIN) PrEP_SCREEN TX_CURR TX_NEW TX_PVLS (D) TX_PVLS (N) TX_RTT Gonaives HTS_TST KP sensitization focusing on Artibonite Saint‐Marc HTS_TST_NEG stigma & discrimination, Nord Cap‐Haitien HTS_TST_POS understanding sexual orientation Croix‐des‐Bouquets KP_PREV & gender identity, and building Leogane PrEP_CURR clinical providers' competency to PrEP_CURR_VERIFY serve KP FY19Q4‐ KOURAJ, ACESH, AJCCDS, ANAPFEH, APLCH, CHAAPES, PrEP_ELIGIBLE Haiti $ 1,000,000.00 83.2% FOSREF FY21Q2 HERITAGE, ORAH, UPLCDS PrEP_NEW Ouest PrEP_NEW_VERIFY Port‐au‐Prince PrEP_SCREEN TX_CURR TX_CURR_VERIFY TX_NEW TX_NEW_VERIFY Bomu Hospital Affiliated Sites Mombasa County Mombasa County not specified HTS_TST Kitui County Kitui County HTS_TST_NEG CHS Naishi Machakos County Machakos County HTS_TST_POS Makueni County Makueni County KP_PREV CHS Tegemeza Plus Muranga County Muranga County PrEP_CURR EGPAF Timiza Homa Bay County Homa Bay County PrEP_CURR_VERIFY Embu County Embu County PrEP_ELIGIBLE Kirinyaga County Kirinyaga County HWWK Nairobi Eastern PrEP_NEW Tharaka Nithi County Tharaka Nithi County -
Legend " Wanseko " 159 !
CONSTITUENT MAP FOR UGANDA_ELECTORAL AREAS 2016 CONSTITUENT MAP FOR UGANDA GAZETTED ELECTORAL AREAS FOR 2016 GENERAL ELECTIONS CODE CONSTITUENCY CODE CONSTITUENCY CODE CONSTITUENCY CODE CONSTITUENCY 266 LAMWO CTY 51 TOROMA CTY 101 BULAMOGI CTY 154 ERUTR CTY NORTH 165 KOBOKO MC 52 KABERAMAIDO CTY 102 KIGULU CTY SOUTH 155 DOKOLO SOUTH CTY Pirre 1 BUSIRO CTY EST 53 SERERE CTY 103 KIGULU CTY NORTH 156 DOKOLO NORTH CTY !. Agoro 2 BUSIRO CTY NORTH 54 KASILO CTY 104 IGANGA MC 157 MOROTO CTY !. 58 3 BUSIRO CTY SOUTH 55 KACHUMBALU CTY 105 BUGWERI CTY 158 AJURI CTY SOUTH SUDAN Morungole 4 KYADDONDO CTY EST 56 BUKEDEA CTY 106 BUNYA CTY EST 159 KOLE SOUTH CTY Metuli Lotuturu !. !. Kimion 5 KYADDONDO CTY NORTH 57 DODOTH WEST CTY 107 BUNYA CTY SOUTH 160 KOLE NORTH CTY !. "57 !. 6 KIIRA MC 58 DODOTH EST CTY 108 BUNYA CTY WEST 161 OYAM CTY SOUTH Apok !. 7 EBB MC 59 TEPETH CTY 109 BUNGOKHO CTY SOUTH 162 OYAM CTY NORTH 8 MUKONO CTY SOUTH 60 MOROTO MC 110 BUNGOKHO CTY NORTH 163 KOBOKO MC 173 " 9 MUKONO CTY NORTH 61 MATHENUKO CTY 111 MBALE MC 164 VURA CTY 180 Madi Opei Loitanit Midigo Kaabong 10 NAKIFUMA CTY 62 PIAN CTY 112 KABALE MC 165 UPPER MADI CTY NIMULE Lokung Paloga !. !. µ !. "!. 11 BUIKWE CTY WEST 63 CHEKWIL CTY 113 MITYANA CTY SOUTH 166 TEREGO EST CTY Dufile "!. !. LAMWO !. KAABONG 177 YUMBE Nimule " Akilok 12 BUIKWE CTY SOUTH 64 BAMBA CTY 114 MITYANA CTY NORTH 168 ARUA MC Rumogi MOYO !. !. Oraba Ludara !. " Karenga 13 BUIKWE CTY NORTH 65 BUGHENDERA CTY 115 BUSUJJU 169 LOWER MADI CTY !. -

PA00W7QH.Pdf
~~ ~~ uKaid from the British people Governance, Accountability, Pa1ticipation and Performance (GAPP) Program Voices From The Field A Collection of short stories on improved service delivery in Uganda through systems strengthening and increasing citizen participation in local governance September 2017 Table of Contents I. Strategic Engagements Improve Access to Education in Patwol village, Gulu district ............................. 7 2. Duty bearers embrace accountability dialogues ................................................................................................ 9 3. Enabling Citizens to Effectively Engage in Local Government Budget Processes .................................... 10 4. Citizen Involvement in Improving the Quality of Water in Nebbi distric ................................................ 12 5. Improving Community Services Through Joint Ef.. ......................................................................................... 14 6. Grassroots Communities Mount Pressure for Better Services .................................................................. 15 7. CSO Mounts Pressure on School to Construct Ramps for Children with Disabilities ......................... 17 8. Government Improves Health Services Following Pressure From Community ..................................... 18 9. Reducing Teacher Absenteeism through Provision of Accommodation Facility ..................................... 20 I 0. Strategic Collaboration results in Safe Drinking Water for Ruchuko Primary School. ....................