A Simple Low-Invasive Method to Assess Sound Pressure Levels at the Eardrum Using Dual-Microphone Measurements in the Open Or Occluded Ear
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Personal Hearing Protection Devices ______
Safe Operating Procedure (Revised 10/14) PERSONAL HEARING PROTECTION DEVICES _____________________________________________________________________ When employees are exposed to sound levels in excess of occupational exposure or action limits, the first course of action is to reduce the noise with source and pathway controls (engineering controls). When sound levels cannot be reduced to less than an 8-hour Time Weighted Average (TWA) of 85 dBA through source and pathway control(s) and/or receiver controls (administrative controls), hearing protection should be used to protect workers from work-related hearing loss. Choosing the right kind of hearing protective device and correct use are essential to protection from hazardous noise exposures. This SOP describes the most common types of hearing protectors used at UNL. There may be specialty hearing protectors prescribed for certain UNL employees exposed to impulse noises which are not addressed in this SOP. Regardless, all employees participating in UNL’s Hearing Conservation Program will receive instruction in proper use of the hearing protectors prescribed for their exposure situation. Types of Hearing Protection There are two main types of hearing protection devices: ear plugs and ear muffs. Ear Plugs Ear plugs (figure 1) are commonly available in the following styles: roll-down foam; pre-molded; and semi-insert. Roll-down foam earplugs are rolled before each use and inserted into the ear canals. They conform to the shape of individual’s ear canals. One size of roll-down foam will fit most workers although workers with extremely small or large ear canals may need a different size. One disadvantage of roll-down foam ear plugs is that workers need to roll them each time they wear them, thus making it harder to use if workers have to take ear plugs out frequently during a work shift. -
Digital Active Noise Reduction (DANR) Custom Earplugs PIN 05-021001
THE SOUND OF SAFETY USER MANUAL Digital Active Noise Reduction (DANR) Custom Earplugs PIN 05-021001 INSIDE: Custom DANR Earplugs 2 Identification . 2 Earplug Insertion Tips . 3 Correct Earplug Insertion 3 Typical Earplug Insertion 4 Waxguard Replacement 5 Replacement Parts . 5-6 Warning . 6 Caution . 7 Contact . 8 DANR Custom Earplugs Connectors Coiled Cables Left Earplug Right Earplug (blue) (red) Replaceable Engraved Serial Waxguard Number Identification Each earplug is molded with a serial number that is used to identify the user. There is a ‘P’ at the beginning of each serial number to indicate the text orientation. 2 | DANR THP & THPC EARPLUGS Earplug Insertion Tips • Inspect the earplugs before each use. The earplugs should be free of debris, Helix tears, and other physical damage. Tip • Inspect the coiled cable and the cable connection to the earplug. Left Earplug Right Earplug • Lubricate the earplugs with water or Aegisound Ear Gel around the canal tip, being careful not to allow water or gel into the opening at the earplug tip. • Gently insert the tip of the earplug into the ear canal with the helix rotated forward. • Rotate the earplug backwards while pushing the earplug until the tip slides into the canal and the helix fits into the pocket at the top of the ear. Correct Earplug Insertion Correct Incorrect Insertion Insertion (Earplug (Earplug not locked locked in in helix) helix) Custom Earplug Familiarization • Wearing the custom earplugs for long periods of time may require an adjustment period of a week or more. • Begin by wearing earplugs for one hour at a time for the first several days. -

Honeywell Howard Leight Arc Flash Protection Brochure
SOUNDSOURCE™ NO. 7-NA-US Arc Flash Protection What requirements must a hearing protector meet for arc flash protection? Arc flash is the term describing an extremely dangerous electrical hazard when uncontrolled current passes through the air between two conductors. When voltage is high enough (over 480V), the intense heat of the arc flash can create a serious hazard for workers in the arc flash zone; temperatures can reach 35,000° F, and the impulse sound resulting from the explosive expansion from the arc can exceed 160 dB peak. Shrapnel from an arc blast can be propelled over 700 mph. Each year, more than 2,000 persons are treated for arc flash burns (NFPA 70E-2015, Annex K). The National Fire Protection Association publishes its NFPA 70E Standard for Electrical Safety in the Workplace1, which defines arc flash boundary zones, and recommended PPE (personal protective equipment) for each zone. The FAQs on the next page summarize the requirements for hearing protection defined in NFPA 70E-2015. Are hearing protectors required for arc flash hazard zones, according to NFPA 70E ? References: Yes, the 2015 standard requires workers in an arc flash hazard zone to wear insert-type 1. National Fire Protection hearing protection (earplugs), as defined in Section 130.7(C)(5)). Association, NFPA 70E®: Standard for Electrical Safety Does NFPA certify or approve particular hearing protectors as being compliant with in the Workplace®, NFPA 70E-2015? No, the NFPA does not certify or approve any PPE. Any manufacturer 2015 edition. claims that a particular piece of PPE has been tested to NFPA standards, or has been 2. -

Measurements of Earplug Attenuation Under Supra-Aural and Circumaural Headphones
International Journal of Audiology 2012; 51: 730–738 Original Article Measurements of earplug attenuation under supra-aural and circumaural headphones Jennifer B. Tufts* , Jillian V. Palmer * & Lynne Marshall† *Department of Communication Sciences, University of Connecticut, Storrs, USA, and †Naval Submarine Medical Research Laboratory, Groton, Connecticut, USA Abstract Objective: Supra-aural audiometric headphones are generally not recommended for use in measuring the attenuation of earplugs, because contact between the headphone and pinna and/or earplug could alter the attenuation obtained, and because of concerns of non-comparability between modes of excitation from supra-aural headphones and the sound-fi eld procedure required by the standardized method. In this study, we compared measurements of earplug attenuation obtained under Telephonics TDH-50P supra-aural headphones with measurements obtained under circumaural headphones designed expressly for such testing. Design: The attenuation of three types of earplugs (foam, premolded quadruple-fl ange, and custom-molded) was measured in a repeated-measures design. Study sample: The study sample comprised 42 normal-hearing adults (21 females, 21 males). Results: With the foam earplugs, nearly all of the attenuation measurements under the supra-aural headphones fell within 10 dB of the measurements under the circumaural headphones. With the fl ange and custom earplugs, approximately 10% of individuals obtained spuriously high attenuation under the supra-aural headphones. Conclusions: We conclude that standard supra-aural audiometric headphones are suitable for measuring the attenuation provided by foam earplugs. However, supra-aural headphones should not be used to measure the attenuation of fl ange or custom-molded earplugs. The potential exists for substantial over-estimation of attenuation, especially of custom plugs. -

DBZ-Earplug Instructions 110518.Indd
For best results follow video instructions at www.decibullz.com/earplug-instructions 3 SHAPE WHAT IS INCLUDED 7 Place ONE mold in the hot water. Multiple molds 5 Let cool for 5 minutes before removing, repeat HEAT WILL stick together if heated at the same time. steps 1-7 with the other mold and ear. (fig. 7) Let sit for 5 minutes. (fig. 3) Insert the mold into your ear and firmly press 1 the back plug into the ear canal (fig. 5) Left and Right 2 Back Plugs S, M, L Triple Flange Attach back plug and correct size silicone tip to custom mold. (fig. 1) Custom Mold Silicone Tips* (NRR 24) DO NOT USE FOAM TIPS FOR MOLDING You can change the tips after the molding process is complete. Check that the tip is securely attached before molding. If the tip CUSTOM MOLDED becomes dislodged in the ear canal seek medical attention. ✔ OR fig. 3 Back plug Silicone tip ✘ fig. 7 Medium Max INCORRECT CORRECT fig. 5 Isolation Foam Drawstring fig. 1 EARPLUG TIP Tips* (NRR 31) Carrying Pouch 4 : Use a mirror to see what you are doing, or have a friend help. To If, for any reason, you are not satisfied with your INSTRUCTIONS ensure a smooth looking mold, avoid using your finger-nails. Remove mold with metal spoon and let cool for Decibullz product, please contact us at 30 seconds. (fig. 4) CAUTION: ITEMS MAY BE VERY HOT. [email protected] before returning. WARNING! 2 Be sure to use a metal spoon, the mold WILL stick to plastic. -

PERSONAL PROTECTIVE EQUIPMENT PROGRAM Owner: Risk Management Document Number: S-006 Revision No: 01 Date Last Revised: 03-02-2018
PERSONAL PROTECTIVE EQUIPMENT PROGRAM Owner: Risk Management Document number: S-006 Revision No: 01 Date last revised: 03-02-2018 Table of Contents 1.0 Applicability ......................................................................................................................................................2 2.0 Scope ...............................................................................................................................................................2 3.0 Definitions ........................................................................................................................................................2 4.0 Core Information and Requirements ...............................................................................................................3 5.0 Roles and Responsibilities ............................................................................................................................ 12 6.0 Goals, Objectives and Performance Measures ............................................................................................ 14 7.0 Training ......................................................................................................................................................... 15 8.0 Program Evaluation ...................................................................................................................................... 15 9.0 Resources .................................................................................................................................................... -
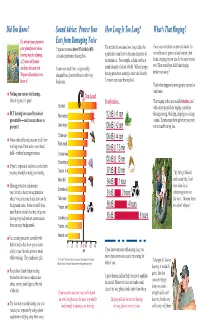
Protect Your Ears from Damaging Noise
Did You Know? Sound Advice: Protect Your How Long Is Too Long? What's That Ringing? It's not just your parent or Ears from Damaging Noise your grandparent whose Exposure to noise above 85 decibels (dB) The red bar below shows how long it takes for Have you ever driven an open cab tractor for hearing may be slipping. can cause permanent hearing loss. a particular sound level to become dangerous to several hours or gone to a loud concert, then A 25-year-old farmer the human ear. For example, a chain saw has a heard a ringing in your ears for the next hour or two? How would you feel if that ringing can have the ears of a It can even result from a single nearby sound intensity of about 109 dB. Without proper never went away? 50-year-old and not even shotgun blast, dynamite blast or other very hearing protection, running a chain saw for only know it! loud noise. 2 minutes can cause hearing loss! That's what happens to many people exposed to loud noise. Nothing can restore lost hearing. Too Loud Once it’s gone, it’s gone! 85 It only takes... That ringing in the ears is called tinnitus, and Gunshot while many people hear ringing, some hear BUT hearing loss caused by noise is Firecrackers 112 dB <1 min hissing, roaring, whistling, chirping or clicking preventable — and you can choose to sounds. Tinnitus may show up before you even prevent it. Grain dryer 109 dB <2 min notice much hearing loss. -

Sound Advice on Hearing Protection for Young Ears
® http://www.noisyplanet.nidcd.nih.gov Sound Advice on Hearing Protection for Young Ears Noise-induced hearing loss (NIHL) occurs when tiny sensory cells in our inner ear, called hair cells, are damaged by sounds that are too loud and that last too long. How near we are to the source of the noise also matters. NIHL can be permanent—but it is preventable. You can help your tween enjoy healthy hearing for a lifetime by learning about hearing protectors and when to use them. When are hearing protectors recommended? Hearing protectors are recommended whenever a person’s hearing is exposed to noise levels that exceed a certain level and time. Scientists have set this level in the workplace at 85 decibels for exposures longer than eight continuous hours. The louder the sound, the shorter the time before damage can occur. In practical terms, your child won’t damage his or her hearing by temporarily cranking up the volume for a favorite song or by taking a short ride on the subway. On the other hand, your tween could potentially damage his or her hearing by listening to music at maximum volume for an extended period of time. The same is true when your tween participates in any activity that exceeds a safe noise level and listening time. Your child should wear hearing protectors while using a lawn mower, operating many power tools, or riding a snowmobile or farm tractor. Hearing protectors may also be advisable when your tween attends certain events in stadiums, gymnasiums, amusement parks, auditoriums, and other entertainment venues. -

Max Single-Use Earplug Highest Attenuation in Single-Use Earplugs
Middle East / India Partners Where To Buy Product Family Max Single-Use Earplug Highest attenuation in single-use earplugs Learn more about our products at howardleight.com > Product Numbers & Ordering Information Product Numbers Details 3301130 Max - corded SNR 37 H - 36 M - 35 L - 31 3301161 Max - uncorded SNR 37 H - 36 M - 35 L - 31 Overview Key Features The world’s most-used polyurethane foam earplug Bell shape delivers maximum in-ear comfort Contoured design easier to insert, resists tendency to back-out of ear canal Polyurethane foam enhances comfort, especially for long-term wear Smooth, soil-resistant closed cell-foam skin prevents dirt build-up Bulk refills for Leight Source 400 and Leight Source 500 Earplug Dispensers save time, waste and space Recommended Industries/Use Agriculture Chemical Construction Fire Protection Forestry Government Law Enforcement Manufacturing Medical Military Mining Municipal Services Oil and Gas Pharmaceutical Steel and Metals Transportation Utilities Welding Hazards Noise Regulations 29 CFR 1910.95 - OSHA Occupational Noise Exposure (US) ANSI S3.19-1974 - Attenuation Test Protocol (US) Page 1 of 3 © Honeywell International Inc. Max Single-Use Earplug - EMEAI Part II, (R.S.C. 1985, c. L-2) - Canada Labour Code Z94.2-1994 - Attenuation Test Protocol (CAN) 2003/10/EC - EU Hearing Directive 89/686/EEC - EC Directive/PPE Category II - EC Category/PPE EN 352-2:2002 - EU Standards NOHSC: 1007 (2000) - National Standard for Occupational Noise (AUS/NZ) NR 15 - Security and Health of Work, Annexes 1 and 2, -

Evaluating the Effectiveness of Earplugs in Preventing Noise-Induced Hearing Loss in an Auto Parts Factory in China
International Journal of Environmental Research and Public Health Article Evaluating the Effectiveness of Earplugs in Preventing Noise-Induced Hearing Loss in an Auto Parts Factory in China Wei Gong 1 , Liangliang Zhao 1, Ling Li 1, Thais C. Morata 2, Wei Qiu 3 , Huiling Amy Feng 2 and Baoli Zhu 4,* 1 Jiangsu Provincial Center for Disease Control and Prevention, Nanjing 210009, China; [email protected] or [email protected] (W.G.); [email protected] (L.Z.); [email protected] (L.L.) 2 National Institute for Occupational Safety and Health (NIOSH), Centers for Disease Control and Prevention (CDC), Cincinnati, OH 45226, USA; [email protected] (T.C.M.); [email protected] (H.A.F.) 3 Auditory Research Laboratories, State University of New York at Plattsburgh, Plattsburgh, NY 12903, USA; [email protected] 4 Center for Global Health, School of Public Health, Nanjing Medical University, Nanjing 211166, China * Correspondence: [email protected]; Tel.: +86-25-83759982 Abstract: A survey was administered to 385 noise-exposed workers from an auto parts factory and 1268 non-noise-exposed health department employees in China. Individual 8 h A-weighted equiva- lent sound levels (LAeq,8h), earplug personal attenuation ratings (PARs), and pure-tone audiometric tests were performed. The average LAeq,8h of noise-exposed workers was 87 dB (A) with a mean PAR of 7 dB. The prevalence of high-frequency hearing loss was 65% for noise-exposed workers and 33% for the non-noise-exposed employees. The use of earplugs had no observable effect on the prevalence of high-frequency hearing loss of the study participants (OR 0.964, 95% CI 0.925–1.005, p = 0.085). -

Danr Thp Danr Thpc
THE SOUND OF SAFETY HEADSET FITTING AND OPERATIONS MANUAL DANR THP DANR THPC INSIDE: Overview .. 2 Before Usage . 2 Earplug Insertion . 3 Headset Assembly and Fitting . 4 Operation . 7 Battery Charging and Maintenance . 8 Earseal Replacement . 10 Warnings . 11 Contact . 12 Overview The Digital Active Noise Reduction (DANR) Triple Hearing Protector (THP) offers superior performance as a double hearing protector with the addition of digital active noise reduction, for a third layer of protection. The DANR Triple Hearing Protector with Communications (THPC) represents Gentex Corporation’s top of the line product for combined communications and hearing protection for excellent performance in extreme noise fields. Before Usage Always evaluate the adequacy of your protective gear before entering hazardous environments. The wearer should ensure that: • The earmuffs and earplugs are fitted, adjusted, and maintained in accordance with the manufacturer’s instructions. Improper fit of this device will reduce its effectiveness in attenuating noise. Consult the included instructions for proper fit. • The earmuffs and earplugs have been inspected for serviceability. • The earmuffs and earplugs are worn at all times in noisy surroundings. The use of any hearing protective device will not guarantee adequate protection for hearing loss for all persons under all circumstances. Consult your physician or audiologist frequently when being exposed to high noise levels. If exposure to high noise levels occurs during employment activities, also consult your employer regularly. US Federal Law requires the following additional statements: The level of noise entering a person’s ear, when hearing protector is worn as directed, is closely approximated by the difference between the A-weighted environmental noise level and the Noise Reduction Rating (NRR). -

11 Personal Measures and Hearing Conservation
11 PERSONAL MEASURES AND HEARING CONSERVATION Professor Samir N.Y. Gerges Federal University of Santa Catarina Mechanical Engineering Department-Noise and Vibration Laboratory Cx.P.476 - Florianópolis - SC BRAZIL [email protected] Mr L. Vedsmand Mr H. Lester* Consultant, Work Environment Health and Safety Executive, UK BAT-Kartellet, Kampmannsgade 4 Postboks 392 DK-1790 Copenhagen DENMARK [email protected] 11.1. WORK PRACTICES AND ADMINISTRATIVE CONTROLS Evaluation of the workplace for noise exposure includes preliminary noise measurements, separation of the workplace into different noise risk areas - and development of both short and long term noise management plans. After evaluation of the workplace, it might be appropriate to evaluate possibilities which the individual employee has to control his or her own (noise) work environment and to evaluate simple measures which may result in a further reduction of the noise level. Whatever noise levels are agreed upon in the workplace, or have been legally demanded, there will always for the individual employee and for a specific group of employees in definite sections of the workplace be a question of what risk is acceptable - or "the acceptability of the noise level in the work environment". Every human has their own limit of acceptance - according to their attitude to their own life and health, their family and their colleaques. This limit of acceptance varies a lot from human to human, but even if the limit is exceeded one will back away from the risk. The limit is rather vague and is related to workers’ traditions, possibilities of finding other less unhealthy jobs and the degree of influence at the workplace.