An Update on Pharmacological Therapy for ADHD Derek Ott, M.D., M.S
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
On Speed: the Many Lives of Amphetamine
On Speed Nicolas Rasmussen On Speed The Many Lives of Amphetamine a New York University Press • New York and London NEW YORK UNIVERSITY PRESS New York and London www.nyupress.org © 2008 by New York University All rights reserved Library of Congress Cataloging-in-Publication Data Rasmussen, Nicolas, 1962– On speed : the many lives of amphetamine / Nicolas Rasmussen. p. ; cm. Includes bibliographical references and index. ISBN-13: 978-0-8147-7601-8 (cl : alk. paper) ISBN-10: 0-8147-7601-9 (cl : alk. paper) 1. Amphetamines—United States—History. 2. Amphetamine abuse— United States—History. I. Title. II. Title: Many lives of amphetamine. [DNLM: 1. Amphetamines—history—United States. 2. Amphetamine-Related Disorders—history—United States. 3. History, 20th Century—United States. 4. History, 21st Century—United States. QV 102 R225o 2007] RM666.A493R37 2007 362.29'90973—dc22 2007043261 New York University Press books are printed on acid-free paper, and their binding materials are chosen for strength and durability. Manufactured in the United States of America c10987654321 p10987654321 To my parents, Laura and Norman, for teaching me to ask questions Contents Acknowledgments ix Introduction 1 1 The New Sensation 6 2 Benzedrine: The Making of a Modern Medicine 25 3 Speed and Total War 53 4 Bootleggers, Beatniks, and Benzedrine Benders 87 5 A Bromide for the Atomic Age 113 6 Amphetamine and the Go-Go Years 149 7 Amphetamine’s Decline: From Mental Medicine to Social Disease 182 8 Fast Forward: Still on Speed, 1971 to Today 222 Conclusion: The Lessons of History 255 Notes 261 List of Archival Sources 347 Index 348 About the Author 352 Illustrations appear in two groups following pages 86 and 148. -

Progress Towards Understanding of Mechanisms of Action of Potent
Wayne State University Wayne State University Dissertations 1-1-2013 Progress Towards Understanding Of Mechanisms Of Action Of Potent Multifunctional Disease Modifying Therapeutics For Parkinson's Disease & Investigating The ethM amphetamine-Induced Striatal Microglia Activation. Mrudang M. Shah Wayne State University, Follow this and additional works at: http://digitalcommons.wayne.edu/oa_dissertations Part of the Medicinal Chemistry and Pharmaceutics Commons, Neurosciences Commons, and the Pharmacology Commons Recommended Citation Shah, Mrudang M., "Progress Towards Understanding Of Mechanisms Of Action Of Potent Multifunctional Disease Modifying Therapeutics For Parkinson's Disease & Investigating The eM thamphetamine-Induced Striatal Microglia Activation." (2013). Wayne State University Dissertations. Paper 916. This Open Access Dissertation is brought to you for free and open access by DigitalCommons@WayneState. It has been accepted for inclusion in Wayne State University Dissertations by an authorized administrator of DigitalCommons@WayneState. PROGRESS TOWARDS UNDERSTANDING OF MECHANISMS OF ACTION OF POTENT MULTIFUNCTIONAL DISEASE MODIFYING THERAPEUTICS FOR PARKINSON’S DISEASE & INVESTIGATING THE METHAMPHETAMINE-INDUCED STRIATAL MICROGLIA ACTIVATION by MRUDANG MANOJKUMAR SHAH DISSERTATION Submitted to the Graduate School Of Wayne State University, Detroit, Michigan in partial fulfillment of the requirements for the degree of DOCTOR OF PHILOSOPHY 2014 MAJOR: PHARMACEUTICAL SCIENCES Approved by: _____________________________________ -

Amphetamine-Related Drugs Neurotoxicity in Humans and in Experimental Animals: Main Mechanisms
Progress in Neurobiology 155 (2017) 149–170 Contents lists available at ScienceDirect Progress in Neurobiology journal homepage: www.elsevier.com/locate/pneurobio Review article Amphetamine-related drugs neurotoxicity in humans and in experimental animals: Main mechanisms Rosario Moratalla a[1_TD$IF],b,*, Amit Khairnar c, Nicola Simola d, Noelia Granado a,b, Jose Ruben Garcı´a-Montes a,b, Pier Francesca Porceddu d, Yousef Tizabi e, Giulia Costa d, Micaela Morelli d,f,g a Instituto Cajal, Consejo Superior de Investigaciones Cientı´ficas, CSIC, Madrid, Spain b CIBERNED, ISCIII, Madrid, Spain c Applied Neuroscience Research Group, CEITEC – Central European Institute of Technology, Masaryk University, Brno, Czech Republic d Department of Biomedical Sciences, Section of Neuropsychopharmacology, University of Cagliari, Via Ospedale 72, 09124 Cagliari, Italy e Department of Pharmacology, Howard University College of Medicine, Washington, DC, USA f Centre of Excellence for Neurobiology of Dependence, University of Cagliari, Cagliari, Italy g National Research Council (CNR), Institute of Neuroscience, Cagliari, Italy ARTICLE INFO ABSTRACT Article history: Amphetamine-related drugs, such as 3,4-methylenedioxymethamphetamine (MDMA) and metham- Received 25 February 2015 phetamine (METH), are popular recreational psychostimulants. Several preclinical studies have Received in revised form 4 September 2015 demonstrated that, besides having the potential for abuse, amphetamine-related drugs may also elicit Accepted 15 September 2015 neurotoxic and neuroinflammatory effects. The neurotoxic potentials of MDMA and METH to Available online 9 October 2015 dopaminergic and serotonergic neurons have been clearly demonstrated in both rodents and non- human primates. This review summarizes the species-specific cellular and molecular mechanisms Keywords: involved in MDMA and METH-mediated neurotoxic and neuroinflammatory effects, along with the most Dopamine important behavioral changes elicited by these substances in experimental animals and humans. -

Amphetamine Type Substance AKA Amphetamines
Amphetamine Type Substance AKA Amphetamines By Gopyraj Sundararajah Examples of the Amphetamines Amphetamine (phenylisopropanlamine: alpha- methylphenlyethylamine) Methamphetamine (methlyamphetamine) 3,4-methylenedioxymethamphetamine (MDMA or ecstasy) 3,4-Methylenedioxyamphetamine (MDA) 3,4-methylenedioxy-N-ethylamphetamine (MDEA, MDE) 3,4-methylenedioxy-alpha-ethyl-N- methylphenethylamine (MBDB) Ephedrine Pseudoephedrine What Do They Do? Stimulant – It stimulates the central nervous system (nerves and brain) by increasing the amount of certain chemicals in the body Appetite suppressant – This increases heart rate and blood pressure and decreases appetite, among other effects Clinical Use Treat narcolepsy Attention deficit disorder with hyperactivity (ADHD) Other purposes? Methamphetamine Slang Speed Whiz Crystal meth Ice Shabu Pure Base Rock Crank P The nickname "P" is unique to New Zealand. How Is It Taken Snorted (especially powdered 'speed') Smoked ('P', a common variant, is often smoked through a glass pipe) Injected Eaten (in pill form) Inserted anally (shelving) Common Effects Energy and alertness Talkativeness, increased confidence, excitement Difficulty sleeping, Reduced appetite Feelings of power and invincibility Aggression, paranoia, irritability Increased heart rate, breathing and blood pressure Sweating, dry mouth, dilated pupils Increased Use Commonly Results In Compounding paranoia Psychosis Extreme mood swings http://www.hollywoodgrind.com/tag/methamphetamine/ Increased Use Commonly Results In Tweaking Violence – Serious -

UC San Diego Electronic Theses and Dissertations
UC San Diego UC San Diego Electronic Theses and Dissertations Title Consider The Pill: Pharmacentric Readings of Post-WWII American Literature Permalink https://escholarship.org/uc/item/4q62090h Author Farinholt, Rhett Publication Date 2019 Peer reviewed|Thesis/dissertation eScholarship.org Powered by the California Digital Library University of California UNIVERSITY OF CALIFORNIA SAN DIEGO Consider The Pill: Pharmacentric Readings of Post-WWII American Literature A dissertation submitted in partial satisfaction of the requirements for the degree Doctor of Philosophy in Literature by Rhett William Farinholt Committee in charge: Professor Michael Davidson, Co-Chair Professor Meg Wesling, Co-Chair Professor Brian Goldfarb Professor Lisa Lampert-Weissig Professor Wm. Arctander O’Brien 2019 Copyright Rhett William Farinholt, 2019 All rights reserved. The Dissertation of Rhett William Farinholt is approved, and it is acceptable in quality and form for publication on microfilm and electronically: _____________________________________________________________ _____________________________________________________________ _____________________________________________________________ _____________________________________________________________ Co-chair _____________________________________________________________ Co-chair University of California San Diego 2019 iii DEDICATION To my parents, Neal and Melanie, without whose love and inspiration, I would not have been in a position to pursue this project. To my wife, Gina, without whose support and -
The Analysis of Amphetamine-Type Stimulants Using Microchip Capillary
The analysis of amphetamine- type stimulants using microchip capillary electrophoresis Aimee Lloyd A thesis submitted for the Degree of Doctor of Philosophy (Science) University of Technology, Sydney July, 2013 Simplicity is the ultimate sophistication Leonardo da Vinci ii Certificate of authorship and originality I certify that the work in this thesis has not previously been submitted for a degree nor has it been submitted as part of the requirements for a degree except as fully acknowledged in the text. I also certify that the thesis has been written by me. Any help I received in my research work and the preparation of the thesis itself has been acknowledged. In addition, I certify that all the information sources and literature used are indicated in the thesis. Aimee Lloyd 31st July 2013 iii Acknowledgements Many people have supported and guided me throughout this mammoth project. It has been an incredible journey and I would like to thank each and every one of you. The insightful discussions, constructive advice and feedback has greatly influenced my personal and intellectual development and opened my mind to new ideas. I am grateful for the funding sources that allowed me carry out this research and attend various meetings and conferences. To my supervisors, Claude Roux and Philip Doble, thank you for your invaluable advice, patience and support throughout my thesis. I am indebted to you both for giving me the chance to embark on such an exciting research project and for the unique opportunities along the way. Claude, my sincere appreciations go to you for your understanding and ongoing support despite your many other commitments. -

Methylamphetamine Review
METHYLAMPHETAMINE REVIEW A REPORT BY THE ADVISORY COUNCIL ON THE MISUSE OF DRUGS 2005 CONTENTS 1. INTRODUCTION..................................................................................................4 Historical overview ............................................................................................................................ 4 Types of methylamphetamine........................................................................................................... 5 This report.......................................................................................................................................... 5 2. MEDICAL USE OF AMPHETAMINE...............................................................6 3. ILLICIT METHYLAMPHETAMINE................................................................7 Administration, purity, dose and price............................................................................................ 8 Patterns of methylamphetamine use................................................................................................ 9 4. METHYLAMPHETAMINE AND OTHER SUBSTANCE USE .....................9 5. AMPHETAMINE & METHYLAMPHETAMINE IN THE UK....................10 History of amphetamines in the UK............................................................................................... 10 Legal status....................................................................................................................................... 11 Seizures of amphetamines.............................................................................................................. -
Epidemic November 29, 2018 Jim Hall [email protected] 1
Epidemic November 29, 2018 Phases of a Drug Epidemic Plateau 35 30 25 Expansion 20 15 10 Users & Problems X Users 1000 & Problems X 5 0 Year 1 Year 2 Year 3 Year 4 Year 5 Year 6 Year 7 Year 8 Year 9 Yr 10 Incubation Incubation Expansion & Problems # of Users Plateau Decline James N. Hall, Senior Epidemiologist Center for Applied Research on Substance Use and Health Disparities Time Nova Southeastern University Components of Substance Use Disorder Epidemiology Contributing Factors of a Drug Epidemic • Host - The User • Agent – The Substances • Environment - Social, Economic, and Geographic Conditions Contributing Factors – Supply Vectors Contributing Factors – Demand Vectors • Production •Attitudes: • Perceived Harmfulness • Patterns of Trafficking • Perceived Wrongfulness • Price • Acceptance by others • Purity • Desired Effects • Profit • Withdrawal – “Dope Sick” • Public Consensus • Availability • Cost • Poisonous Contamination • Rapid Onset of Action • Access Jim Hall [email protected] 1 Epidemic November 29, 2018 Reoccurring Patterns of Opioid Epidemics: 1880 - 2018 Opioids 1990 - 2018 Reoccurring Heroin & Fentanyls Patterns of 1955 - 1970 Rx Opioids Substance Use 1880 - 1900 Disorder Heroin Epidemics Morphine & Heroin 1880 – 2018 # # of users and level of consequences 1880 1890 1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010 2018 The Morphine Molecule DEFINITION OF OPIOID • Binding to and activating “Similar to opium” the opioid μ receptors in the brain and spine Morphine and similar drugs derived from opium • Principal -
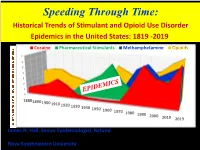
Methamphetamine Opioids
Speeding Through Time: Historical Trends of Stimulant and Opioid Use Disorder Epidemics in the United States: 1819 -2019 Cocaine Pharmaceutical Stimulants Methamphetamine Opioids 7 6 5 4 3 2 1 0 1880 18901900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010 2019 James N. Hall, Senior Epidemiologist, Retired Center for Applied Research on Substance Use and Health Disparities Nova Southeastern University No Relevant Financial Conflicts: Relevant to the content of this educational activity, I do not have any relevant financial conflicts with commercial interest companies to disclose. Phases of a Drug Epidemic Plateau 35 30 25 Expansion 20 15 10 Users & Problems 1000 X 5 0 Year 1 Year 2 Year 3 Year 4 Year 5 Year 6 Year 7 Year 8 Year 9 Yr 10 Incubation Incubation Expansion # of Users # of Users & Problems Plateau Decline Time Contributing Factors of a Drug Epidemic Contributing Factors – Supply Vectors • Production • Patterns of Trafficking • Price • Purity • Profit • Availability • Poisonous Contamination Contributing Factors – Demand Vectors •Attitudes: • Perceived Harmfulness • Perceived Wrongfulness • Acceptance by others • Desired Effects • Withdrawal – “Dope Sick” • Public Consensus • Cost • Rapid Onset of Action • Access Reoccurring Patterns of Substance Use Disorder Epidemics 1880 – 2019 Reoccurring Patterns of Opioid Epidemics: 1880 - 2019 Opioids 1990 - 2019 Heroin & Fentanyls 1955 - 1970 Rx Opioids 1880 - 1920 Heroin Morphine & Heroin # of users and level of consequences level and # users of 1880 1890 1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010 2018 History of Opioids • Opium the first drug from early agricultural civilizations • Assyrians invented slicing the poppy pod • Sumerians - The “Joy Plant” • Egyptians first produced opium as a drug – Thebaine • Greeks • Indian Subcontinent • Medieval Trade spread the drug • 1804 German pharmacist first isolated Morphine • Named after the Greek god of sleep and dreams, Morpheus • 19th Century 330 Wars forced production of Morphine • Used in US Civil War History of Opioids in the U.S. -

From Made in America to Hecho En Sinaloa: a Historical Geography of North American Methamphetamine Networks
From Made in America to Hecho en Sinaloa: A Historical Geography of North American Methamphetamine Networks BY ©2012 Aaron H. Gilbreath Submitted to the graduate degree program in the Department of Geography and the Graduate Faculty of the University of Kansas in partial fulfillment of the requirements for the degree of Doctor of Philosophy. _______________________________________________ Chairperson James R. Shortridge _______________________________________________ Garth Myers _______________________________________________ Terry Slocum _______________________________________________ Barney Warf _______________________________________________ Cheryl Lester Date Defended: 6/4/12 The Dissertation Committee for Aaron H. Gilbreath certifies that this is the approved version of the following dissertation: From Made in America to Hecho en Sinaloa: A Historical Geography of North American Methamphetamine Networks ___________________________________________________ Chairperson James R. Shortridge Date approved: 6/4/12 ii ABSTRACT Most of the major drugs of abuse in the Untied States have a relatively uniform distribution. Their use may cluster in cities, for eXample, but that general pattern tends to repeat itself in every region of the county. This is not true of the stimulant methamphetamine, which today shows a decidedly uneven distribution. Confounding the matter more is the fact that, because it is a synthetic drug, it is theoretically possible to make methamphetamine anywhere. But it is not made everywhere. In fact, for much of its history, -

Mescaline: the Cberrris'try and Ph.Arrnacology of Its Analogs'
Mescaline: The Cberrris'try and Ph.arrnacology of its Analogs' ALEXANDER T. SHULGIN 1483 Shulgin Road, Lafayette, California ABSTRACT.-Although mescaline (3,4,S-trimethoxyphenethylamine, the principal alkaloid of the Peyote plant Lophophora williarnsii) has been extensively explored in man as a hallucinogenic intoxicant, only a few of the natural alkaloids that accom- pany it in nature have been evaluated as chemical individuals. It appears that these congeners do not contribute to the reported action of the intact plant. Synthetic modifications of the structure of mescaline have been more rewarding in the search for relationships between the details of chemical structure and of biological activity. The most throughly investigated analogs are the substituted phenylisopro- pylamines. These carry the carbon skeleton of amphetamine, as is found in natural bases such as ephedrine. Ring substitution arrangements that imitate the peyote alkaloids and the phenylpropenes from the essential oils, have led to a number of hal- lucinogens generally more potent than mescaline. These all reflect some botanical precedent. Other analogs are based largely on changes in the length of the carbon chain, or in the nature of the substituent in the 4-position (para to the aliphatic chain). The shortening of the chain always decreases the observed potency, but any lengthening invariably changes the pharmacological action from hallucinogenesis to relaxants or to psychic energizers. The para-substitution changes involving alkyl groups, halides, or cyclic ethers have led to a retention of mescaline-like activity, but with a consistent increase in potency. The preceding three papers of this symposium have reviewed much of our current knowledge concerning Peyote. -

Determination of Amphetamines-Type Stimulants in Urine Samples Using Microextraction by Packed Sorbent and Gas Chromatography-Mass Spectrometry
UNIVERSIDADE DA BEIRA INTERIOR Ciências Determination of amphetamines-type stimulants in urine samples using microextraction by packed sorbent and gas chromatography-mass spectrometry Sara Patrícia Romão Malaca Dissertação para a obtenção do Grau de Mestre em Bioquímica (2º ciclo de estudos) Orientador: Mestre Tiago Alexandre Pires Rosado Co-orientador: Professora Doutora Maria Eugenia Gallardo Alba Covilhã, outubro de 2018 ii Determination of amphetamines-type stimulants in urine samples using microextraction by packed sorbent and gas chromatography-mass spectrometry Agradecimentos Sou profundamente grata às seguintes pessoas, pelo seu incentivo constante, pela ajuda e inspiração, que foram essenciais não só para a elaboração desta dissertação mas também para a minha vida: Primeiramente aos meus orientadores: Ao Mestre Tiago Rosado, pela confiança que depositou em mim, toda a ajuda e paciência, desde o primeiro dia em que lhe pedi para assistir aos primeiros projetos até agora que finalizo esta etapa. À Doutora Eugenia Gallardo por todo o apoio, a sua amabilidade e todos os conselhos que me deu ao longo destes dois anos. Foi um gosto enorme poder fazer esta caminhada convosco do meu lado, batalhando dia após dia, superando desventuras e celebrando conquistas. Levo muito de vocês comigo. Ao Doutor Mário Barroso, por toda a ajuda prestada ao longo desta jornada. A todos os colegas que de alguma maneira me ajudaram durante este percurso, principalmente na última e mais complicada fase deste trabalho. Às minhas amigas Liliana Fernandes, Daniela Rafain, Joana Tabuaço, Ana Sofia Santos e Inês Neves, somos a prova de que distância não implica ausência e que por muitos anos que passem, amizades feitas na universidade podem de facto ser amizades de uma vida.