Scar Sarcoidosis: a Case Report and Brief Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Extrafacial Granuloma Faciale
Journal of the American Osteopathic College of Dermatology Volume 11, Number 1 SPONSORS: ',/"!,0!4(/,/'9,!"/2!4/29s-%$)#)3 July 2008 34)%&%,,!"/2!4/2)%3s'!,$%2-! www.aocd.org Journal of the American Osteopathic College of Dermatology Journal of the American Osteopathic College of Dermatology 2007-2008 Officers President: Jay Gottlieb, DO President Elect: Donald Tillman, DO First Vice President: Marc Epstein, DO Second Vice President: Leslie Kramer, DO Third Vice President: Bradley Glick, DO Secretary-Treasurer: Jere Mammino, DO (2007-2010) Immediate Past President: Bill Way, DO Trustees: James Towry, DO (2006-2008) Mark Kuriata, DO (2007-2010) Karen Neubauer, DO (2006-2008) David Grice, DO (2007-2010) Sponsors: Global Pathology Laboratory Editors Stiefel Laboratories Jay S. Gottlieb, D.O., F.O.C.O.O. Medicis Stanley E. Skopit, D.O., F.A.O.C.D. James Q. Del Rosso, D.O., F.A.O.C.D. Galderma Editorial Review Board Ronald Miller, D.O. JAOCD Eugene Conte, D.O. Founding Sponsor Evangelos Poulos, M.D. Stephen Purcell, D.O. Darrel Rigel, M.D. !/#$s%)LLINOISs+IRKSVILLE -/ s&!8 Robert Schwarze, D.O. WWWAOCDORG Andrew Hanly, M.D. #/092)'(4!.$0%2-)33)/.WRITTENPERMISSIONMUSTBEOBTAINED Michael Scott, D.O. FROMTHE*OURNALOFTHE!MERICAN/STEOPATHIC#OLLEGEOF$ERMATOLOGY FORCOPYINGORREPRINTINGTEXTOFMORETHANHALFPAGE TABLESORlGURES Cindy Hoffman, D.O. 0ERMISSIONSARENORMALLYGRANTEDCONTINGENTUPONSIMILARPERMISSION Charles Hughes, D.O. FROMTHEAUTHORS INCLUSIONOFACKNOWLEDGEMENTOFTHEORIGINALSOURCE ANDAPAYMENTOFPERPAGE TABLEORlGUREOFREPRODUCEDMATERIAL Bill Way, D.O. 0ERMISSIONFEESAREWAIVEDFORAUTHORSWISHINGTOREPRODUCETHEIROWN Daniel Hurd, D.O. ARTICLES2EQUESTFORPERMISSIONSHOULDBEDIRECTEDTO*!/#$CO!/#$ 0/"OX+IRKSVILLE -/ Mark Lebwohl, M.D. #OPYRIGHTBYTHE*OURNALOFTHE!MERICAN/STEOPATHIC#OLLEGEOF Edward Yob, D.O. $ERMATOLOGY Jere Mammino, D.O. Printed by: Stoyles Graphics Services, Mason City, IA 50401 Schield M. -

A Review of the Evidence for and Against a Role for Mast Cells in Cutaneous Scarring and Fibrosis
International Journal of Molecular Sciences Review A Review of the Evidence for and against a Role for Mast Cells in Cutaneous Scarring and Fibrosis Traci A. Wilgus 1,*, Sara Ud-Din 2 and Ardeshir Bayat 2,3 1 Department of Pathology, Ohio State University, Columbus, OH 43210, USA 2 Centre for Dermatology Research, NIHR Manchester Biomedical Research Centre, Plastic and Reconstructive Surgery Research, University of Manchester, Manchester M13 9PT, UK; [email protected] (S.U.-D.); [email protected] (A.B.) 3 MRC-SA Wound Healing Unit, Division of Dermatology, University of Cape Town, Observatory, Cape Town 7945, South Africa * Correspondence: [email protected]; Tel.: +1-614-366-8526 Received: 1 October 2020; Accepted: 12 December 2020; Published: 18 December 2020 Abstract: Scars are generated in mature skin as a result of the normal repair process, but the replacement of normal tissue with scar tissue can lead to biomechanical and functional deficiencies in the skin as well as psychological and social issues for patients that negatively affect quality of life. Abnormal scars, such as hypertrophic scars and keloids, and cutaneous fibrosis that develops in diseases such as systemic sclerosis and graft-versus-host disease can be even more challenging for patients. There is a large body of literature suggesting that inflammation promotes the deposition of scar tissue by fibroblasts. Mast cells represent one inflammatory cell type in particular that has been implicated in skin scarring and fibrosis. Most published studies in this area support a pro-fibrotic role for mast cells in the skin, as many mast cell-derived mediators stimulate fibroblast activity and studies generally indicate higher numbers of mast cells and/or mast cell activation in scars and fibrotic skin. -

Crohn's Disease-Associated Interstitial Lung Disease Mimicking Sarcoidosis
Case report SARCOIDOSIS VASCULITIS AND DIFFUSE LUNG DISEASES 2016; 33; 288-291 © Mattioli 1885 Crohn’s disease-associated interstitial lung disease mimicking sarcoidosis: a case report and review of the literature Choua Thao1, A Amir Lagstein2, T Tadashi Allen3, Huseyin Erhan Dincer4, Hyun Joo Kim4 1Department of Internal Medicine, University of Nevada School of Medicine Las Vegas, Las Vegas, NV; 2Department of Pathology, Univer- sity of Michigan, Ann Arbor, MI; 3Department of Radiology, University of Minnesota, Minneapolis, MN; 4 Division of Pulmonary, Allergy, Critical Care and Sleep Medicine, University of Minnesota, Minneapolis, MN Abstract. Respiratory involvement in Crohn’s disease (CD) is a rare manifestation known to involve the large and small airways, lung parenchyma, and pleura. The clinical presentation is nonspecific, and diagnostic tests can mimic other pulmonary diseases, posing a diagnostic challenge and delay in treatment. We report a case of a 60-year-old female with a history of CD and psoriatic arthritis who presented with dyspnea, fever, and cough with abnormal radiological findings. Diagnostic testing revealed an elevated CD4:CD8 ratio in the bronchoal- veolar lavage fluid, and cryoprobe lung biopsy results showed non-necrotizing granulomatous inflammation. We describe here the second reported case of pulmonary involvement mimicking sarcoidosis in Crohn’s disease and a review of the literature on the approaches to making a diagnosis of CD-associated interstitial lung disease. (Sarcoidosis Vasc Diffuse Lung Dis 2016; 33: 288-291) Key words: interstitial lung disease, Crohns disease, sarcoidosis, cryoprobe lung biopsy Introduction Moreover, certain diagnostic tests such as bronchoal- veolar lavage (BAL) cell analysis and tissue biopsy Pulmonary involvement in Crohn’s disease (CD) results may mimic other granulomatous lung diseas- is relatively rare and can be difficult to diagnose. -

Urticaria from Wikipedia, the Free Encyclopedia Jump To: Navigation, Search "Hives" Redirects Here
Urticaria From Wikipedia, the free encyclopedia Jump to: navigation, search "Hives" redirects here. For other uses, see Hive. Urticaria Classification and external resourcesICD-10L50.ICD- 9708DiseasesDB13606MedlinePlus000845eMedicineemerg/628 MeSHD014581Urtic aria (or hives) is a skin condition, commonly caused by an allergic reaction, that is characterized by raised red skin wheals (welts). It is also known as nettle rash or uredo. Wheals from urticaria can appear anywhere on the body, including the face, lips, tongue, throat, and ears. The wheals may vary in size from about 5 mm (0.2 inches) in diameter to the size of a dinner plate; they typically itch severely, sting, or burn, and often have a pale border. Urticaria is generally caused by direct contact with an allergenic substance, or an immune response to food or some other allergen, but can also appear for other reasons, notably emotional stress. The rash can be triggered by quite innocent events, such as mere rubbing or exposure to cold. Contents [hide] * 1 Pathophysiology * 2 Differential diagnosis * 3 Types * 4 Related conditions * 5 Treatment and management o 5.1 Histamine antagonists o 5.2 Other o 5.3 Dietary * 6 See also * 7 References * 8 External links [edit] Pathophysiology Allergic urticaria on the shin induced by an antibiotic The skin lesions of urticarial disease are caused by an inflammatory reaction in the skin, causing leakage of capillaries in the dermis, and resulting in an edema which persists until the interstitial fluid is absorbed into the surrounding cells. Urticarial disease is thought to be caused by the release of histamine and other mediators of inflammation (cytokines) from cells in the skin. -

Neurosarcoidosis
CHAPTER 11 Neurosarcoidosis E. Hoitsma*,#, O.P. Sharma} *Dept of Neurology and #Sarcoidosis Management Centre, University Hospital Maastricht, Maastricht, The Netherlands, and }Dept of Pulmonary and Critical Care Medicine, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA. Correspondence: O.P. Sharma, Room 11-900, LACzUSC Medical Center, 1200 North State Street, Los Angeles, CA 90033, USA. Fax: 1 3232262728; E-mail: [email protected] Sarcoidosis is an inflammatory multisystemic disorder. Its cause is not known. The disease may involve any part of the nervous system. The incidence of clinical involvement of the nervous system in a sarcoidosis population is estimated to be y5–15% [1, 2]. However, the incidence of subclinical neurosarcoidosis may be much higher [3, 4]. Necropsy studies suggest that ante mortem diagnosis is made in only 50% of patients with nervous system involvement [5]. As neurosarcoidosis may manifest itself in many different ways, diagnosis may be complicated [2, 3, 6–10]. It may appear in an acute explosive fashion or as a slow chronic illness. Furthermore, any part of the nervous system can be attacked by sarcoidosis, but the cranial nerves, hypothalamus and pituitary gland are more commonly involved [1]. Sarcoid granulomas can affect the meninges, parenchyma of the brain, hypothalamus, brainstem, subependymal layer of the ventricular system, choroid plexuses and peripheral nerves, and also the blood vessels supplying the nervous structures [11, 12]. One-third of neurosarcoidosis patients show multiple neurological lesions. If neurological syndromes develop in a patient with biopsy- proven active systemic sarcoidosis, the diagnosis is usually easy. However, without biopsy evidence of sarcoidosis at other sites, nervous system sarcoidosis remains a difficult diagnosis [13]. -

Fundamentals of Dermatology Describing Rashes and Lesions
Dermatology for the Non-Dermatologist May 30 – June 3, 2018 - 1 - Fundamentals of Dermatology Describing Rashes and Lesions History remains ESSENTIAL to establish diagnosis – duration, treatments, prior history of skin conditions, drug use, systemic illness, etc., etc. Historical characteristics of lesions and rashes are also key elements of the description. Painful vs. painless? Pruritic? Burning sensation? Key descriptive elements – 1- definition and morphology of the lesion, 2- location and the extent of the disease. DEFINITIONS: Atrophy: Thinning of the epidermis and/or dermis causing a shiny appearance or fine wrinkling and/or depression of the skin (common causes: steroids, sudden weight gain, “stretch marks”) Bulla: Circumscribed superficial collection of fluid below or within the epidermis > 5mm (if <5mm vesicle), may be formed by the coalescence of vesicles (blister) Burrow: A linear, “threadlike” elevation of the skin, typically a few millimeters long. (scabies) Comedo: A plugged sebaceous follicle, such as closed (whitehead) & open comedones (blackhead) in acne Crust: Dried residue of serum, blood or pus (scab) Cyst: A circumscribed, usually slightly compressible, round, walled lesion, below the epidermis, may be filled with fluid or semi-solid material (sebaceous cyst, cystic acne) Dermatitis: nonspecific term for inflammation of the skin (many possible causes); may be a specific condition, e.g. atopic dermatitis Eczema: a generic term for acute or chronic inflammatory conditions of the skin. Typically appears erythematous, -

Advances in Seborrheic Keratosis
A CME/CE-Certified Supplement to Original Release Date: December 2018 Advances in Seborrheic Expiration Date: December 31, 2020 Estimated Time To Complete Activity: 1 hour Participants should read the activity information, Keratosis review the activity in its entirety, and complete the online post-test and evaluation. Upon completing this activity as designed and achieving a passing score on FACULTY the post-test, you will be directed to a Web page that will Joseph F. Fowler Jr, MD Michael S. Kaminer, MD allow you to receive your certificate of credit via e-mail Clinical Professor and Director Associate Clinical Professor of Dermatology or you may print it out at that time. Contact and Occupational Yale Medical School The online post-test and evaluation can be accessed Dermatology New Haven, Connecticut at http://tinyurl.com/SebK2018. University of Louisville School of Adjunct Assistant Professor of Medicine Medicine (Dermatology), Warren Alpert Medical School Inquiries about continuing medical education (CME) Louisville, Kentucky of Brown University accreditation may be directed to the University of Providence, Rhode Island Louisville Office of Continuing Medical Education & Professional Development (CME & PD) at cmepd@ louisville.edu or (502) 852-5329. Designation Statement eborrheic keratosis (SK) has been called keratinizing surface.12 They can develop virtually The University of Louisville School of Medicine the “Rodney Dangerfield of skin lesions”— anywhere except for the palms, soles, and mucous designates this Enduring material for a maximum of 9 1.0 AMA PRA Category 1 Credit(s)™. Physicians should it earns little respect (as a clinical concern) membranes, but are most commonly observed claim only the credit commensurate with the extent of Sbecause of its benignity, commonality, usual on the trunk and face.6,13 The tendency to develop their participation in the activity. -

Dermatopathology
Dermatopathology Clay Cockerell • Martin C. Mihm Jr. • Brian J. Hall Cary Chisholm • Chad Jessup • Margaret Merola With contributions from: Jerad M. Gardner • Talley Whang Dermatopathology Clinicopathological Correlations Clay Cockerell Cary Chisholm Department of Dermatology Department of Pathology and Dermatopathology University of Texas Southwestern Medical Center Central Texas Pathology Laboratory Dallas , TX Waco , TX USA USA Martin C. Mihm Jr. Chad Jessup Department of Dermatology Department of Dermatology Brigham and Women’s Hospital Tufts Medical Center Boston , MA Boston , MA USA USA Brian J. Hall Margaret Merola Department of Dermatology Department of Pathology University of Texas Southwestern Medical Center Brigham and Women’s Hospital Dallas , TX Boston , MA USA USA With contributions from: Jerad M. Gardner Talley Whang Department of Pathology and Dermatology Harvard Vanguard Medical Associates University of Arkansas for Medical Sciences Boston, MA Little Rock, AR USA USA ISBN 978-1-4471-5447-1 ISBN 978-1-4471-5448-8 (eBook) DOI 10.1007/978-1-4471-5448-8 Springer London Heidelberg New York Dordrecht Library of Congress Control Number: 2013956345 © Springer-Verlag London 2014 This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifi cally the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfi lms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. Exempted from this legal reservation are brief excerpts in connection with reviews or scholarly analysis or material supplied specifi cally for the purpose of being entered and executed on a computer system, for exclusive use by the purchaser of the work. -

Linear Scleroderma “En Coup De Sabre” Coexisting with Plaque-Morphea
661 J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.74.5.661 on 1 May 2003. Downloaded from SHORT REPORT Linear scleroderma “en coup de sabre” coexisting with plaque-morphea: neuroradiological manifestation and response to corticosteroids I Unterberger, E Trinka, K Engelhardt, A Muigg, P Eller, M Wagner, N Sepp, G Bauer ............................................................................................................................. J Neurol Neurosurg Psychiatry 2003;74:661–664 progression of skin lesions or any neurological abnormalities A 24 year old woman in the 33rd week of pregnancy during follow up. developed progressive neurological complications with On admission the patient was in the 33rd week of right sided hemiparesis in association with the occurrence pregnancy. She was fully oriented, had normal speech, and of linear scleroderma “en coup de sabre” (LSCS) and pre- presented with a right sided hemiparesis (grade 3/5, MRC existing plaque-morphea, already being treated by scale) with a positive Babinski sign on the right. There was no balneophototherapy. Further progression of neurological history of head trauma. symptoms led to a caesarean section with the delivery of a Routine laboratory testing and comprehensive serological healthy child. Brain magnetic resonance imaging (MRI) screening including antineutrophilic cytoplasmic antibodies showed focal T2 signal increases in the left frontoparietal (ANCA), anticardiolipin antibodies, and antibodies against region directly adjacent to the area of LSCS. -

Basal Cell Carcinoma Associated with Non-Neoplastic Cutaneous Conditions: a Comprehensive Review
Volume 27 Number 2| February 2021 Dermatology Online Journal || Review 27(2):1 Basal cell carcinoma associated with non-neoplastic cutaneous conditions: a comprehensive review Philip R Cohen MD1,2 Affiliations: 1San Diego Family Dermatology, National City, California, USA, 2Touro University California College of Osteopathic Medicine, Vallejo, California, USA Corresponding Author: Philip R Cohen, 10991 Twinleaf Court, San Diego, CA 92131-3643, Email: [email protected] pathogenesis of BCC is associated with the Abstract hedgehog signaling pathway and mutations in the Basal cell carcinoma (BCC) can be a component of a patched homologue 1 (PCTH-1) transmembrane collision tumor in which the skin cancer is present at tumor-suppressing protein [2-4]. Several potential the same cutaneous site as either a benign tumor or risk factors influence the development of BCC a malignant neoplasm. However, BCC can also concurrently occur at the same skin location as a non- including exposure to ultraviolet radiation, genetic neoplastic cutaneous condition. These include predisposition, genodermatoses, immunosuppression, autoimmune diseases (vitiligo), cutaneous disorders and trauma [5]. (Darier disease), dermal conditions (granuloma Basal cell carcinoma usually presents as an isolated faciale), dermal depositions (amyloid, calcinosis cutis, cutaneous focal mucinosis, osteoma cutis, and tumor on sun-exposed skin [6-9]. However, they can tattoo), dermatitis, miscellaneous conditions occur as collision tumors—referred to as BCC- (rhinophyma, sarcoidal reaction, and varicose veins), associated multiple skin neoplasms at one site scars, surgical sites, systemic diseases (sarcoidosis), (MUSK IN A NEST)—in which either a benign and/or systemic infections (leischmaniasis, leprosy and malignant neoplasm is associated with the BCC at lupus vulgaris), and ulcers. -
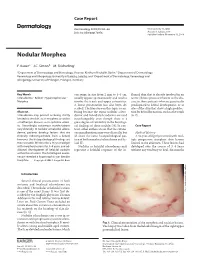
Nodular Morphea
Case Report Dermatology 2009;218:63–66 Received: July 13, 2008 DOI: 10.1159/000173976 Accepted: July 23, 2008 Published online: November 13, 2008 Nodular Morphea a b c F. Kauer J.C. Simon M. Sticherling a b Department of Dermatology and Venerology, Vivantes Klinikum Neukölln, Berlin , Department of Dermatology, c Venerology and Allergology, University of Leipzig, Leipzig , and Department of Dermatology, Venerology and Allergology, University of Erlangen, Erlangen , Germany Key Words can range in size from 2 mm to 4–5 cm, flamed skin that is already involved in an -Scleroderma ؒ Keloid ؒ Hypertrophic scar ؒ usually appear spontaneously and tend to active fibrotic process inherent to the dis Morphea involve the trunk and upper extremities. ease in those patients who are genetically A linear presentation has also been de- predisposed to keloid development, or at scribed. The literature on this topic is con- sites of the skin that show a high predilec- Abstract fusing because the terms ‘nodular sclero- tion for keloid formation, such as the trunk Scleroderma may present as being strictly derma’ and ‘keloidal scleroderma’ are used [6, 7] . limited to the skin, as in morphea, or within interchangeably even though there is a a multiorgan disease, as in systemic sclero- great degree of variability in the histologi- sis. Accordingly, cutaneous manifestations cal findings of these nodules [4] . In con- C a s e R e p o r t vary clinically. In nodular or keloidal sclero- trast, other authors stress that the cutane- derma, patients develop lesions that are ous manifestations may vary clinically, but Medical History clinically indistinguishable from a keloid; all share the same histopathological pat- A 16-year-old girl presented with mul- however, the histopathological findings are tern of both morphea/scleroderma and ke- tiple progressive morpheic skin lesions more variable. -

Treatment Or Removal of Benign Skin Lesions
Treatment or Removal of Benign Skin Lesions Date of Origin: 10/26/2016 Last Review Date: 03/24/2021 Effective Date: 04/01/2021 Dates Reviewed: 10/2016, 10/2017, 10/2018, 04/2019, 10/2019, 01/2020, 03/2020, 03/2021 Developed By: Medical Necessity Criteria Committee I. Description Individuals may acquire a multitude of benign skin lesions over the course of a lifetime. Most benign skin lesions are diagnosed on the basis of clinical appearance and history. If the diagnosis of a lesion is uncertain, or if a lesion has exhibited unexpected changes in appearance or symptoms, a diagnostic procedure (eg, biopsy, excision) is indicated to confirm the diagnosis. The treatment of benign skin lesions consists of destruction or removal by any of a wide variety of techniques. The removal of a skin lesion can range from a simple biopsy, scraping or shaving of the lesion, to a radical excision that may heal on its own, be closed with sutures (stitches) or require reconstructive techniques involving skin grafts or flaps. Laser, cautery or liquid nitrogen may also be used to remove benign skin lesions. When it is uncertain as to whether or not a lesion is cancerous, excision and laboratory (microscopic) examination is usually necessary. II. Criteria: CWQI HCS-0184A Note: **If request is for treatment or removal of warts, medical necessity review is not required** A. Moda Health will cover the treatment and removal of 1 or more of the following benign skin lesions: a. Treatment or removal of actinic keratosis (pre-malignant skin lesions due to sun exposure) is considered medically necessary with 1 or more of the following procedures: i.