Infections Due to Trichosporon Cutaneum, an Uncommon Systemic Pathogen Tom Madhavan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Fungal Infections from Human and Animal Contact
Journal of Patient-Centered Research and Reviews Volume 4 Issue 2 Article 4 4-25-2017 Fungal Infections From Human and Animal Contact Dennis J. Baumgardner Follow this and additional works at: https://aurora.org/jpcrr Part of the Bacterial Infections and Mycoses Commons, Infectious Disease Commons, and the Skin and Connective Tissue Diseases Commons Recommended Citation Baumgardner DJ. Fungal infections from human and animal contact. J Patient Cent Res Rev. 2017;4:78-89. doi: 10.17294/2330-0698.1418 Published quarterly by Midwest-based health system Advocate Aurora Health and indexed in PubMed Central, the Journal of Patient-Centered Research and Reviews (JPCRR) is an open access, peer-reviewed medical journal focused on disseminating scholarly works devoted to improving patient-centered care practices, health outcomes, and the patient experience. REVIEW Fungal Infections From Human and Animal Contact Dennis J. Baumgardner, MD Aurora University of Wisconsin Medical Group, Aurora Health Care, Milwaukee, WI; Department of Family Medicine and Community Health, University of Wisconsin School of Medicine and Public Health, Madison, WI; Center for Urban Population Health, Milwaukee, WI Abstract Fungal infections in humans resulting from human or animal contact are relatively uncommon, but they include a significant proportion of dermatophyte infections. Some of the most commonly encountered diseases of the integument are dermatomycoses. Human or animal contact may be the source of all types of tinea infections, occasional candidal infections, and some other types of superficial or deep fungal infections. This narrative review focuses on the epidemiology, clinical features, diagnosis and treatment of anthropophilic dermatophyte infections primarily found in North America. -

Utility of Miconazole Therapy for Trichosporon Fungemia in Patients with Acute Leukemia
Advances in Microbiology, 2013, 3, 47-51 Published Online December 2013 (http://www.scirp.org/journal/aim) http://dx.doi.org/10.4236/aim.2013.38A008 Utility of Miconazole Therapy for Trichosporon Fungemia in Patients with Acute Leukemia Kazunori Nakase1,2*, Kei Suzuki2, Taiichi Kyo3, Yumiko Sugawara2, Shinichi Kageyama2, Naoyuki Katayama2 1Cancer Center, Mie University Hospital, Tsu, Japan 2Department of Hematology and Oncology, Mie University Graduate School of Medicine, Tsu, Japan 3Fourth Department of Internal Medicine, Hiroshima Red Cross and Atomic-Bomb Survivors Hospital, Hiroshima, Japan Email: [email protected] Received October 15, 2013; revised November 15, 2013; accepted November 21, 2013 Copyright © 2013 Kazunori Nakase et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Invasive trichosporonosis is an extremely rare mycosis, but Trichosporon fungemia (TF) in patients with hematologic malignancies has been increasingly recognized to be a fulminant and highly lethal infection. Although the utility of az- ole therapy has been demonstrated in several observations, little is known about the efficacy of one of azoles, micona- zole (MCZ). To assess its therapeutic role, we retrospectively investigated 6 cases of TF in patients with acute leukemia receiving MCZ containing regimens. Successful outcome was obtained in 4 patients [MCZ + amphotericin B (AmB) in 2, MCZ only and MCZ + fluconazole (FLCZ) + AmB in one each], but not in 2 (MCZ + FLCZ + AmB and MCZ + FLCZ in one each). Although MCZ and AmB exhibited good in vitro activities against isolates from all patients, FLCZ had such finding from only one patient. -

Standard Methods for Fungal Brood Disease Research Métodos Estándar Para La Investigación De Enfermedades Fúngicas De La Cr
Journal of Apicultural Research 52(1): (2013) © IBRA 2013 DOI 10.3896/IBRA.1.52.1.13 REVIEW ARTICLE Standard methods for fungal brood disease research Annette Bruun Jensen1*, Kathrine Aronstein2, José Manuel Flores3, Svjetlana Vojvodic4, María 5 6 Alejandra Palacio and Marla Spivak 1Department of Plant and Environmental Sciences, University of Copenhagen, Thorvaldsensvej 40, 1817 Frederiksberg C, Denmark. 2Honey Bee Research Unit, USDA-ARS, 2413 E. Hwy. 83, Weslaco, TX 78596, USA. 3Department of Zoology, University of Córdoba, Campus Universitario de Rabanales (Ed. C-1), 14071, Córdoba, Spain. 4Center for Insect Science, University of Arizona, 1041 E. Lowell Street, PO Box 210106, Tucson, AZ 85721-0106, USA. 5Unidad Integrada INTA – Facultad de Ciencias Ags, Universidad Nacional de Mar del Plata, CC 276,7600 Balcarce, Argentina. 6Department of Entomology, University of Minnesota, St. Paul, Minnesota 55108, USA. Received 1 May 2012, accepted subject to revision 17 July 2012, accepted for publication 12 September 2012. *Corresponding author: Email: [email protected] Summary Chalkbrood and stonebrood are two fungal diseases associated with honey bee brood. Chalkbrood, caused by Ascosphaera apis, is a common and widespread disease that can result in severe reduction of emerging worker bees and thus overall colony productivity. Stonebrood is caused by Aspergillus spp. that are rarely observed, so the impact on colony health is not very well understood. A major concern with the presence of Aspergillus in honey bees is the production of airborne conidia, which can lead to allergic bronchopulmonary aspergillosis, pulmonary aspergilloma, or even invasive aspergillosis in lung tissues upon inhalation by humans. In the current chapter we describe the honey bee disease symptoms of these fungal pathogens. -

Trichosporon Beigelii Infection Presenting As White Piedra and Onychomycosis in the Same Patient
Trichosporon beigelii Infection Presenting as White Piedra and Onychomycosis in the Same Patient Lt Col Kathleen B. Elmer, USAF; COL Dirk M. Elston, MC, USA; COL Lester F. Libow, MC, USA Trichosporon beigelii is a fungal organism that causes white piedra and has occasionally been implicated as a nail pathogen. We describe a patient with both hair and nail changes associated with T beigelii. richosporon beigelii is a basidiomycetous yeast, phylogenetically similar to Cryptococcus.1 T T beigelii has been found on a variety of mammals and is present in soil, water, decaying plants, and animals.2 T beigelii is known to colonize normal human skin, as well as the respiratory, gas- trointestinal, and urinary tracts.3 It is the causative agent of white piedra, a superficial fungal infection of the hair shaft and also has been described as a rare cause of onychomycosis.4 T beigelii can cause endo- carditis and septicemia in immunocompromised hosts.5 We describe a healthy patient with both white piedra and T beigelii–induced onychomycosis. Case Report A 62-year-old healthy man who worked as a pool maintenance employee was evaluated for thickened, discolored thumb nails (Figure 1). He had been aware of progressive brown-to-black discoloration of the involved nails for 8 months. In addition, soft, light yellow-brown nodules were noted along the shafts of several axillary hairs (Figure 2). Microscopic analysis of the hairs revealed nodal concretions along the shafts (Figure 3). No pubic, scalp, eyebrow, eyelash, Figure 1. Onychomycotic thumb nail. or beard hair involvement was present. Cultures of thumb nail clippings on Sabouraud dextrose agar grew T beigelii and Candida parapsilosis. -

Oral Antifungals Month/Year of Review: July 2015 Date of Last
© Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 | Fax 503-947-1119 Class Update with New Drug Evaluation: Oral Antifungals Month/Year of Review: July 2015 Date of Last Review: March 2013 New Drug: isavuconazole (a.k.a. isavunconazonium sulfate) Brand Name (Manufacturer): Cresemba™ (Astellas Pharma US, Inc.) Current Status of PDL Class: See Appendix 1. Dossier Received: Yes1 Research Questions: Is there any new evidence of effectiveness or safety for oral antifungals since the last review that would change current PDL or prior authorization recommendations? Is there evidence of superior clinical cure rates or morbidity rates for invasive aspergillosis and invasive mucormycosis for isavuconazole over currently available oral antifungals? Is there evidence of superior safety or tolerability of isavuconazole over currently available oral antifungals? • Is there evidence of superior effectiveness or safety of isavuconazole for invasive aspergillosis and invasive mucormycosis in specific subpopulations? Conclusions: There is low level evidence that griseofulvin has lower mycological cure rates and higher relapse rates than terbinafine and itraconazole for adult 1 onychomycosis.2 There is high level evidence that terbinafine has more complete cure rates than itraconazole (55% vs. 26%) for adult onychomycosis caused by dermatophyte with similar discontinuation rates for both drugs.2 There is low -

Histopathology of Important Fungal Infections
Journal of Pathology of Nepal (2019) Vol. 9, 1490 - 1496 al Patholo Journal of linic gist C of of N n e o p ti a a l- u i 2 c 0 d o n s 1 s 0 a PATHOLOGY A m h t N a e K , p d of Nepal a l a M o R e d n i io ca it l A ib ss xh www.acpnepal.com oc g E iation Buildin Review Article Histopathology of important fungal infections – a summary Arnab Ghosh1, Dilasma Gharti Magar1, Sushma Thapa1, Niranjan Nayak2, OP Talwar1 1Department of Pathology, Manipal College of Medical Sciences, Pokhara, Nepal. 2Department of Microbiology, Manipal College of Medical Sciences , Pokhara, Nepal. ABSTRACT Keywords: Fungus; Fungal infections due to pathogenic or opportunistic fungi may be superficial, cutaneous, subcutaneous Mycosis; and systemic. With the upsurge of at risk population systemic fungal infections are increasingly common. Opportunistic; Diagnosis of fungal infections may include several modalities including histopathology of affected tissue Systemic which reveal the morphology of fungi and tissue reaction. Fungi can be in yeast and / or hyphae forms and tissue reactions may range from minimal to acute or chronic granulomatous inflammation. Different fungi should be differentiated from each other as well as bacteria on the basis of morphology and also clinical correlation. Special stains like GMS and PAS are helpful to identify fungi in tissue sections. INTRODUCTION Correspondence: Dr Arnab Ghosh, MD Fungal infections or mycoses may be caused by Department of Pathology, pathogenic fungi which infect healthy individuals or by Manipal College of Medical Sciences, Pokhara, Nepal. -

Two Cases of Scalp White Piedra Caused by Trichosporon Ovoides
Case TTwowo ccasesases ooff sscalpcalp wwhitehite ppiedraiedra causedcaused byby Report TTrichosporonrichosporon ovoidesovoides SSwagatawagata AA.. TTambe,ambe, SS.. RRachitaachita DDhurat,hurat, CChayahaya A.A. KKumarumar1, PPreetireeti TThakare,hakare, NNitinitin LLade,ade, HHemangiemangi Jerajani,Jerajani, MMeenakshieenakshi MathurMathur 1 Departments of Dermatology ABSTRACT and 1Microbiology, Lokmanya Tilak Municipal Medical White piedra is a superÞ cial fungal infection of the hair shaft, caused by Trichosporon beigelii. College and General Hospital, Sion Mumbai - 400 022, India We report two cases of white piedra presenting as brown palpable nodules along the hair shaft with a fragility of scalp hairs. T. beigelii was demonstrated in hair culture of both the patients Address for correspondence: and T. ovoides as a species was conÞ rmed on carbohydrate assimilation test. The Þ rst patient Dr. Swagata Arvind Tambe, responded to oral itraconazole and topical ketoconazole, with a decrease in the palpability of 19/558, Udyan Housing nodules and fragility of scalp hairs at the end of two months. Society, Nehru Nagar, Kurla (East), Key words: White piedra, Carbohydrate assimilation test, Itraconazole, Trichosporon ovoides Mumbai – 400 024, India. E-mail: [email protected] DOI: 10.4103/0378-6323.51256 PMID: 19439885 IINTRODUCTIONNTRODUCTION with fragility for 3 and 2 months, respectively. Both the patients had a history of tying wet hairs after washing. White piedra is a superficial fungal infection of Other hairy parts of the body were not similarly the hair shaft, caused by Trichosporon beigelii, also affected in both. Their family members had no similar known as tinea nodosa, trichosporonosis nodosa involvement. Both had never visited southern parts of and trichomycosis nodularis.[1] Common areas of India or used oils excessively. -

Department of Biological Sciences Redeemer's
DEPARTMENT OF BIOLOGICAL SCIENCES REDEEMER’S UNIVERSITY MCB 313 PATHOGENIC MYCOLOGY DURUGBO ERNEST UZODIMMA (Ph.D.) COURSE OUTLINE 1. Introduction 2. Structure, reproduction and classification of pathogenic Fungi Eg. Aspergillus, Trichphyton spp., Tinea spp.,Yeasts 3.Superficial systematic mycoses and antimycoses 4. Fungal infections ( Candidiasis , Histoplasmosis etc) 5. Laboratory methods of study 5. Pathology and immunology 6. Cultivation techniques in Mycology Structure, Reproduction and Classification of Pathogenic Fungi About 30% of the 100,000 known species of Fungi make a living as parasites, or pathogens , mostly of plants. E. g Cryphonectria parasitica, the Ascomycete fungus causes chestnut blight. Fusarium circinatum causes pith pine canker a diseae that threatens pine worldwide. Puccinia graminis causes black stem rust of wheat. Some of the fungi that attack food crops are toxic to humans for example certain species of the ascomycete mold Aspergillus contaminate improperly stored grain and peanuts by secreting aflatoxins which are carcinogenic. The ascomycete Claviceps purpurea which grows on rye plants forming purple structures called ergots. If diseased rye is milled into flour and consumed it causes ergotism, a condition characterized by gangrene, nervous spasms, burning sensations, hallucinations, and temporary insanity. An epidemic of this around 944 C.E, killed more than 40,000 people in France. Animals are much less susceptible to parasitic fungi than plants. Only about 50 species of fungi are known to parasitize humans and animals . Such fungal infections are mycosis . Skin mycoses includes ringworm. The ascomycetes that causes ringworm can infect almost any skin surface. Most commonly, they grow on the feet, causing the intense itching and blisters known as athlete ’s foot. -

Fungal Infections
FUNGAL INFECTIONS SUPERFICIAL MYCOSES DEEP MYCOSES MIXED MYCOSES • Subcutaneous mycoses : important infections • Mycologists and clinicians • Common tropical subcutaneous mycoses • Signs, symptoms, diagnostic methods, therapy • Identify the causative agent • Adequate treatment Clinical classification of Mycoses CUTANEOUS SUBCUTANEOUS OPPORTUNISTIC SYSTEMIC Superficial Chromoblastomycosis Aspergillosis Aspergillosis mycoses Sporotrichosis Candidosis Blastomycosis Tinea Mycetoma Cryptococcosis Candidosis Piedra (eumycotic) Geotrichosis Coccidioidomycosis Candidosis Phaeohyphomycosis Dermatophytosis Zygomycosis Histoplasmosis Fusariosis Cryptococcosis Trichosporonosis Geotrichosis Paracoccidioidomyc osis Zygomycosis Fusariosis Trichosporonosis Sporotrichosis • Deep / subcutaneous mycosis • Sporothrix schenckii • Saprophytic , I.P. : 8-30 days • Geographical distribution Clinical varieties (Sporotrichosis) Cutaneous • Lymphangitic or Pulmonary lymphocutaneous Renal Systemic • Fixed or endemic Bone • Mycetoma like Joint • Cellulitic Meninges Lymphangitic form (Sporotrichosis) • Commonest • Exposed sites • Dermal nodule pustule ulcer sporotrichotic chancre) (Sporotrichosis) (Sporotrichosis) • Draining lymphatic inflamed & swollen • Multiple nodules along lymphatics • New nodules - every few (Sporotrichosis) days • Thin purulent discharge • Chronic - regional lymph nodes swollen - break down • Primary lesion may heal spontaneously • General health - may not be affected (Sporotrichosis) (Sporotrichosis) Fixed/Endemic variety (Sporotrichosis) • -

Mycologic Disorders of the Skin Catherine A
Mycologic Disorders of the Skin Catherine A. Outerbridge, DVM, MVSc, DACVIM, DACVD Cutaneous tissue can become infected when fungal organisms contaminate or colonize the epidermal surface or hair follicles. The skin can be a portal of entry for fungal infection when the epithelial barrier is breached or it can be a site for disseminated, systemic fungal disease. The two most common cutaneous fungal infections in small animals are dermato- phytosis and Malassezia dermatitis. Dermatophytosis is a superficial cutaneous infection with one or more of the fungal species in the keratinophilic genera Microsporum, Tricho- phyton,orEpidermophyton. Malassezia pachydermatis is a nonlipid dependent fungal species that is a normal commensal inhabitant of the skin and external ear canal in dogs and cats. Malassezia pachydermatis is the most common cause of Malassezia dermatitis. The diagnosis and treatment of these cutaneous fungal infections will be discussed. Clin Tech Small Anim Pract 21:128-134 © 2006 Elsevier Inc. All rights reserved. KEYWORDS dermatophytosis, Malassezia dermatitis, dogs, cats, Microsporum, Trichophyton, Malassezia pachydermatis ver 300 species of fungi have been reported toDermatophytosis be animal O pathogens.1 Cutaneous tissue can become infected when fungal organisms contaminate or colonize the epider- Etiology mal surface or hair follicles. The skin can be a portal of entry Dermatophytosis is a superficial cutaneous infection with for fungal infection when the epithelial barrier is breached or one or more of the fungal species in the keratinophilic genera it can be a site for disseminated, systemic fungal disease. Microsporum, Trichophyton,orEpidermophyton. Dermato- Canine and feline skin and hair coats can be transiently con- phyte genera that infect animals are divided into 3 or 4 taminated with a large variety of saprophytic fungi from the groups based on their natural habitat. -

Studies on Phaeohyphomycosis and Its Causative Agents in China
Jpn. J. Med. Mycol. Vol. 37, 135-141, 1996 ISSN 0916-4804 Review Studies on Phaeohyphomycosis and Its Causative Agents in China Ruoyu Li, Duanli Wang Department of Dermatology, First Hospital of Beijing Medical University, Beijing, China Abstract Until now, 10 cases of phaeohyphomycosis have been reported in China. Their causative agents were as follows: Exophiala dermatitidis (4 cases), E, spinifera (3), E. jeanselmei (1), Alternaria alternata (1) and Veronaeabotryosa (1). The clinical data will be reviewed in this paper. The pathogenic dematiaceous fungi isolated from the phaeohyphomycosis patients were identified carefully and the conidiogenesis of these organisms was studied by using a scanning electron micro- scope. Besides of these, physiological and other studies were also carried out to aid the correct classi- fication and identification. RAPD-PCR technique was applied to the genomic DNA assay of pathogenic black yeasts' and reveled highly polymorphisms in their genomic fingerprints. The ecological studies were carried out and seven species were isolated from the soil and rotting plant materials. Phialophora aerrucosa was the most dominant species in nature in Shandong, China, followed by Exophiala spinifera and Veronaeabotryosa. The pathogenicity of Yeronaeabotryosa and Exophiala spinifera were studied by using both normal and precompromised mice. The results show that both natural and clinical strains of V. botryosa have potential pathogenicity. E. spinifera is neurotropic and its pathogenicity is specially potential in immunodeficient hosts. Key words: Phaeohyphomycosis, dematiaceous fungi, Exophiala spp., Conidiogenesis, RAPD-PCR mycosis as an opportunistic fungal infection, and Introduction dematiaceous yeast-like cells, pseudohyphae-like Dematiaceous fungi represent a group of fungi elements, hyphae of various shapes or any combi- that bear melanin-like pigment on the wall of nation of these forms could be found in tissue. -
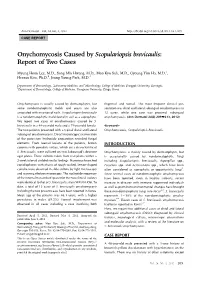
Onychomycosis Caused by Scopulariopsis Brevicaulis Ann Dermatol Vol
Onychomycosis Caused by Scopulariopsis brevicaulis Ann Dermatol Vol. 24, No. 2, 2012 http://dx.doi.org/10.5021/ad.2012.24.2.209 CASE REPORT Onychomycosis Caused by Scopulariopsis brevicaulis: Report of Two Cases Myung Hoon Lee, M.D., Sung Min Hwang, M.D., Moo Kyu Suh, M.D., Gyoung Yim Ha, M.D.1, Heesoo Kim, Ph.D.2, Jeong Young Park, M.D.3 Departments of Dermatology, 1Laboratory Medicine, and 2Microbiology, College of Medicine, Dongguk University, Gyeongju, 3Department of Dermatology, College of Medicine, Yeungnam University, Daegu, Korea Onychomycosis is usually caused by dermatophytes, but fingernail and toenail. The most frequent clinical pre- some nondermatophytic molds and yeasts are also sentation was distal and lateral subungual onychomycosis in associated with invasion of nails. Scopulariopsis brevicaulis 12 cases, while one case was proximal subungual is a nondermatophytic mold found in soil as a saprophyte. onychomycosis. (Ann Dermatol 24(2) 209∼213, 2012) We report two cases of onychomycosis caused by S. brevicaulis in a 48-year-old male and a 79-year-old female. -Keywords- The two patients presented with a typical distal and lateral Onychomycosis, Scopulariopsis brevicaulis subungual onychomycosis. Direct microscopic examination of the potassium hydroxide preparation revealed fungal elements. From toenail lesions of the patients, brown INTRODUCTION colonies with powdery surface, which are a characteristic of S. brevicaulis, were cultured on two Sabouraud’s dextrose Onychomycosis is mainly caused by dermatophytes, but agar plates. Three cultures taken from nail plates within a is occasionally caused by nondermatophytic fungi 2-week interval yielded similar findings. Numerous branched including Scopulariopsis brevicaulis, Aspergillus spp., conidiophores with chains of rough walled, lemon-shaped Fusarium spp.