Antenatal Depression in a Rural District in Uganda: Findings from a Facility-Based Cross-Sectional Study
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Vote:517 Kamuli District Quarter2
Local Government Quarterly Performance Report FY 2020/21 Vote:517 Kamuli District Quarter2 Terms and Conditions I hereby submit Quarter 2 performance progress report. This is in accordance with Paragraph 8 of the letter appointing me as an Accounting Officer for Vote:517 Kamuli District for FY 2020/21. I confirm that the information provided in this report represents the actual performance achieved by the Local Government for the period under review. Date: 11/02/2021 cc. The LCV Chairperson (District) / The Mayor (Municipality) 1 Local Government Quarterly Performance Report FY 2020/21 Vote:517 Kamuli District Quarter2 Summary: Overview of Revenues and Expenditures Overall Revenue Performance Ushs Thousands Approved Budget Cumulative Receipts % of Budget Received Locally Raised Revenues 545,891 373,486 68% Discretionary Government 4,425,320 2,335,957 53% Transfers Conditional Government Transfers 38,103,649 18,539,523 49% Other Government Transfers 1,995,208 612,466 31% External Financing 1,314,664 604,003 46% Total Revenues shares 46,384,732 22,465,434 48% Overall Expenditure Performance by Workplan Ushs Thousands Approved Cumulative Cumulative % Budget % Budget % Releases Budget Releases Expenditure Released Spent Spent Administration 5,566,664 2,817,313 2,271,323 51% 41% 81% Finance 500,261 242,532 192,277 48% 38% 79% Statutory Bodies 915,404 477,769 413,546 52% 45% 87% Production and Marketing 1,755,678 882,304 663,561 50% 38% 75% Health 9,769,288 4,987,922 4,043,308 51% 41% 81% Education 22,602,810 10,376,662 8,850,508 46% 39% 85% -
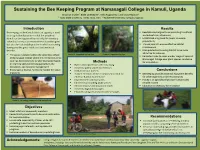
Sustaining the Bee Keeping Program at Namasagali College in Kamuli
Sustaining the Bee Keeping Program at Namasagali College in Kamuli, Uganda Brooklyn Snyder1, Blake Lineweaver2, Mika Rugaramna3, and Grace Nabulo4, 1, 2Iowa State University, Ames, Iowa, USA 3, 4Makerere University, Kampala, Uganda Introduction Results Beekeeping, in the Kamuli district of Uganda, is used . Reestablished original hives according to cultural as an agricultural practice so that the people of and educational influencers Kamuli can be supported by not only the monetary . Established a log book for pupils to ensure value that honey as an entrepreneurial product gives productivity but also the sustainable practice in which consuming . Trained pupils to ensure effective habitat honey provides great nutritional and medicinal maintenance benefits. Manipulated surrounding habitat to be more attractive for colonies . The apiary is located within the secondary school Photo 2). Supported top bar hive Photo 3). Supported log hive . Relocated hives to cover a wider range of space at of Namasagali College where the entrepreneurship Namasagali College near plant species conducive club has direct access to be able to practice hands- Methods for colonization on learning skills concerning agriculture, the . Bated unoccupied hives with cow dung ecosystem, and business management . Created a pulley system for the hives . Encourages a diverse, functional habitat for native . Contacted local farmers Conclusions organisms . Trained members of the entrepreneurial club for . Beekeeping provides essential ecosystem benefits effective habitat maintenance for other organisms and the community . Implemented sunflower plots . Honey is an agricultural product that provides . Identified surrounding plant species reliable income . Cleared invasive and unwanted brush . Education is necessary for innovation . Created a log book for pupils . -

Vote:017 Ministry of Energy and Mineral Development
Vote Performance Report Financial Year 2018/19 Vote:017 Ministry of Energy and Mineral Development QUARTER 1: Highlights of Vote Performance V1: Summary of Issues in Budget Execution Table V1.1: Overview of Vote Expenditures (UShs Billion) Approved Cashlimits Released Spent by % Budget % Budget % Releases Budget by End Q1 by End Q 1 End Q1 Released Spent Spent Recurrent Wage 6.225 1.556 1.556 1.152 25.0% 18.5% 74.1% Non Wage 85.788 16.876 16.876 15.937 19.7% 18.6% 94.4% Devt. GoU 325.227 165.045 165.045 139.862 50.7% 43.0% 84.7% Ext. Fin. 1,339.221 258.273 258.273 360.077 19.3% 26.9% 139.4% GoU Total 417.240 183.477 183.477 156.952 44.0% 37.6% 85.5% Total GoU+Ext Fin 1,756.460 441.750 441.750 517.029 25.1% 29.4% 117.0% (MTEF) Arrears 0.242 0.173 0.173 0.000 71.4% 0.0% 0.0% Total Budget 1,756.702 441.922 441.922 517.029 25.2% 29.4% 117.0% A.I.A Total 0.000 0.000 0.000 0.000 0.0% 0.0% 0.0% Grand Total 1,756.702 441.922 441.922 517.029 25.2% 29.4% 117.0% Total Vote Budget 1,756.460 441.750 441.750 517.029 25.1% 29.4% 117.0% Excluding Arrears Table V1.2: Releases and Expenditure by Program* Billion Uganda Shillings Approved Released Spent % Budget % Budget %Releases Budget Released Spent Spent Program: 0301 Energy Planning,Management & 890.50 253.99 214.55 28.5% 24.1% 84.5% Infrastructure Dev't Program: 0302 Large Hydro power infrastructure 751.03 145.75 285.22 19.4% 38.0% 195.7% Program: 0303 Petroleum Exploration, Development, 57.93 22.14 6.98 38.2% 12.0% 31.5% Production, Value Addition and Distribution and Petrolleum Products Program: -

Impact of Nutrition Education Centers on Food and Nutrition Security in Kamuli District, Uganda Samuel Ikendi Iowa State University
Iowa State University Capstones, Theses and Graduate Theses and Dissertations Dissertations 2019 Impact of nutrition education centers on food and nutrition security in Kamuli District, Uganda Samuel Ikendi Iowa State University Follow this and additional works at: https://lib.dr.iastate.edu/etd Part of the Agriculture Commons Recommended Citation Ikendi, Samuel, "Impact of nutrition education centers on food and nutrition security in Kamuli District, Uganda" (2019). Graduate Theses and Dissertations. 17032. https://lib.dr.iastate.edu/etd/17032 This Thesis is brought to you for free and open access by the Iowa State University Capstones, Theses and Dissertations at Iowa State University Digital Repository. It has been accepted for inclusion in Graduate Theses and Dissertations by an authorized administrator of Iowa State University Digital Repository. For more information, please contact [email protected]. Impact of nutrition education centers on food and nutrition security in Kamuli District, Uganda by Samuel Ikendi A thesis submitted to the graduate faculty in partial fulfillment of the requirements for the degree of MASTER OF COMMUNITY AND REGIONAL PLANNING MASTER OF SCIENCE Co-majors: Community and Regional Planning; Sustainable Agriculture Program of Study Committee: Francis Owusu, Major Professor Carmen Bain Ann Oberhauser The student author, whose presentation of the scholarship herein was approved by the program of study committee, is solely responsible for the content of this thesis. The Graduate College will ensure this thesis is globally accessible and will not permit alterations after a degree is conferred. Iowa State University Ames, Iowa 2019 Copyright © Samuel Ikendi, 2019. All rights reserved. ii DEDICATION To the NECs hosts, NEC Trainers, and my mum Christine Lubaale, may the Gracious Lord reward you all abundantly for your generosity. -

Kamuli District Local Government Performance Assessment Report
Local Government Performance Assessment Kamuli District (Vote Code: 517) Assessment Scores Accountability Requirements 83% Crosscutting Performance Measures 59% Educational Performance Measures 68% Health Performance Measures 65% Water Performance Measures 75% 517 Kamuli District Accountability Requirements 2019 Summary of requirements Definition of compliance Compliance justification Compliant? Annual performance contract Yes LG has submitted an annual performance • From MoFPED’s The Annual Performance Contract for the contract of the forthcoming year by June 30 on inventory/schedule of LG forthcoming year 2020/21 was submitted the basis of the PFMAA and LG Budget submissions of performance on 17thJuly, 2019 and thus adhered to guidelines for the coming financial year. contracts, check dates of the adjusted submission date of submission and issuance of 31stAugust, 2019. receipts and: o If LG submitted before or by due date, then state ‘compliant’ o If LG had not submitted or submitted later than the due date, state ‘non- compliant’ • From the Uganda budget website: www.budget.go.ug, check and compare recorded date therein with date of LG submission to confirm. Supporting Documents for the Budget required as per the PFMA are submitted and available Yes LG has submitted a Budget that includes a • From MoFPED’s inventory Kamuli LG submitted the approved Procurement Plan for the forthcoming FY by of LG budget submissions, Budget Estimates that included a 30th June (LG PPDA Regulations, 2006). check whether: Procurement Plan for the FY 2019/20 on 17thJuly, 2019 thus being within the o The LG budget is adjusted submission date of 31st August, accompanied by a 2019. Procurement Plan or not. -

Emergency Health Fiscal and Growth Stabilization and Development
LIST OF COVID-19 QUARANTINE CENTRES IN WATER AND POWER UTILITIES OPERATION AREAS WATER S/N QUARANTINE CENTRE LOCATION POWER UTILITY UTILITY 1 MASAFU GENERAL HOSPITAL BUSIA UWS-E UMEME LTD 2 BUSWALE SECONDARY SCHOOL NAMAYINGO UWS-E UMEME LTD 3 KATAKWI ISOLATION CENTRE KATAKWI UWS-E UMEME LTD 4 BUKWO HC IV BUKWO UWS-E UMEME LTD 5 AMANANG SECONDARY SCHOOL BUKWO UWS-E UMEME LTD 6 BUKIGAI HC III BUDUDA UWS-E UMEME LTD 7 BULUCHEKE SECONDARY SCHOOL BUDUDA UWS-E UMEME LTD 8 KATIKIT P/S-AMUDAT DISTRICT KATIKIT UWS-K UEDCL 9 NAMALU P/S- NAKAPIRIPIRIT DISTRICT NAMALU UWS-K UEDCL 10 ARENGESIEP S.S-NABILATUK DISTRICT ARENGESIEP UWS-K UEDCL 11 ABIM S.S- ABIM DISTRICT ABIM UWS-K UEDCL 12 KARENGA GIRLS P/S-KARENGA DISTRICT KARENGA UWS-K UMEME LTD 13 NAKAPELIMORU P/S- KOTIDO DISTRICT NAKAPELIMORU UWS-K UEDCL KOBULIN VOCATIONAL TRAINING CENTER- 14 NAPAK UWS-K UEDCL NAPAK DISTRICT 15 NADUNGET HCIII -MOROTO DISTRICT NADUNGET UWS-K UEDCL 16 AMOLATAR SS AMOLATAR UWS-N UEDCL 17 OYAM OYAM UWS-N UMEME LTD 18 PADIBE IN LAMWO DISTRICT LAMWO UWS-N UMEME LTD 19 OPIT IN OMORO OMORO UWS-N UMEME LTD 20 PABBO SS IN AMURU AMURU UWS-N UEDCL 21 DOUGLAS VILLA HOSTELS MAKERERE NWSC UMEME LTD 22 OLIMPIA HOSTEL KIKONI NWSC UMEME LTD 23 LUTAYA GEOFREY NAJJANANKUMBI NWSC UMEME LTD 24 SEKYETE SHEM KIKONI NWSC UMEME LTD PLOT 27 BLKS A-F AKII 25 THE EMIN PASHA HOTEL NWSC UMEME LTD BUA RD 26 ARCH APARTMENTS LTD KIWATULE NWSC UMEME LTD 27 ARCH APARTMENTS LTD KIGOWA NTINDA NWSC UMEME LTD 28 MARIUM S SANTA KYEYUNE KIWATULE NWSC UMEME LTD JINJA SCHOOL OF NURSING AND CLIVE ROAD JINJA 29 MIDWIFERY A/C UNDER MIN.OF P.O.BOX 43, JINJA, NWSC UMEME LTD EDUCATION& SPORTS UGANDA BUGONGA ROAD FTI 30 MAAIF(FISHERIES TRAINING INSTITUTE) NWSC UMEME LTD SCHOOL PLOT 4 GOWERS 31 CENTRAL INN LIMITED NWSC UMEME LTD ROAD PLOT 2 GOWERS 32 CENTRAL INN LIMITED NWSC UMEME LTD ROAD PLOT 45/47 CHURCH 33 CENTRAL INN LIMITED NWSC UMEME LTD RD CENTRAL I INSTITUTE OF SURVEY & LAND PLOT B 2-5 STEVEN 34 NWSC 0 MANAGEMENT KABUYE CLOSE 35 SURVEY TRAINING SCHOOL GOWERS PARK NWSC 0 DIVISION B - 36 DR. -
2018 Annual Report
Sustaining Connections That Matter Center for Sustainable Rural Livelihoods 2018 DONOR IMPACT REPORT A Message from the President In the year 2050, a gathering will Dear People of the Year 2050: take place at the Mpirigiti Rural Training Centre in the Kamuli Greetings from the year 2018! This year we dedicated the Mpirigiti Rural Training Centre. It is a District of Uganda. The purpose wonderful new facility. We trust the passing years have made the Mpirigiti center a hopeful destination of the assembled group will be for many thousands of people — those who have come eager to learn, those who have come willing to to open a time capsule from the serve, and those who have been blessed by working together to pursue a happier, hope-filled future. year 2018. In our current world of 2018, we often talk about “2050” as an important year — a time for which we The time capsule was sealed must direct our energies now to ensure that expanding world populations have enough nourishing this past July when I was food to eat and are able to lead healthy, satisfying lives. “Food is the moral right of all who are born honored to be present to help into this world” — That’s what Norman Borlaug, a famous Iowan, agricultural scientist and Nobel dedicate the new training center Prize laureate, once said. We hope 2050 finds that all people have attained this moral right. for the Center for Sustainable Rural Livelihoods. For nearly 15 Here are the main messages I’d like to share with you: years, we have worked hand- 2018 DONOR IMPACT REPORT 2018 DONOR IMPACT in-hand with the people of the To the people of the Kamuli District in 2050: Sustain our friendship and partnership many years into DS Kamuli District to make their the future. -

A Case of Upland and Paddy Rice in Namasagali Sub-County Kamuli District
Joint proceedings of the 27th Soil Science Society of East Africa and the 6th African Soil Science Society Resource use efficiency in rice based farming systems: A case of upland and paddy rice in Namasagali sub-county Kamuli District J. Mabiriizi Julius and M. Isabirye Faculty of Natural Res. and Environ. Sci, Busitema Univer., Tororo, Uganda [email protected] Abstract Rice is an emerging and one of the important cereal crops grown in Uganda. Being a relatively new crop, farmers are faced with a challenge of effectively utilising resources and their combination for maximum productivity and therefore profit. Therefore the study identified the determinants of efficient rice production in Namasagali sub-county with a backdrop of ensuring food security and enhancing the sustainable use of wetlands. These were attained through the use of a logistic regression and the Cobb- Douglas production function model to find the determinants and the level of technical efficiency respectively. Results show that out of the 11 factors assessed, 7 of them were found significant at 5% level of significance. Land size devoted to rice cultivation was the most significant factor determining technical efficiency of rice cultivation in the area. Others are education level, experience, motive of the farmer, family size, labour and use of ox-plough. However, rice type, fertilizer application, gender and land ownership were found insignificant in determining technical efficiency in the area. The Cobb- Douglas results exhibit that the farmers in Namasagali sub-county are generally technically inefficient due to decreasing returns to scale of production, implying that key factors of production are over- utilized. -
Sffi" ,Ff Er-- 4Y 1.O
1 fl hE PARLIAMENT OF UGANDA REPORT OF THE COMMITTEE ON GOVERNMENT ASSURANCES AND IMPLEMENTATION ON THE STATUS OF IMPLEMENTATION OF GOVERNMENT ASSURANCES IN SECTORS OF HEALTH, IVORKS AND TRANSPORT IN SELECTED DISTRICTS, Lt--t-= OITIIICI| OF THII CLERK TO PARLIAMENT PARLIAMDNT BUILDINGS (f KAMPALA - UGANDA M^.\a,20r8 t V, sffi" ,ff er-- 4y 1.O. INTRODUCTION Committee Mandate 1) In accordance with Rule 176 of the Parliamentary Rules of Procedure 2017, t:ne Commtttee on Government Assurances and implementation is mandated to: (a) record and scrutinize the Assurances, Promrses and Undertakings given by the Presrdent, Vice President, Pnme Minrster and Ministers tn the House from time to time; (b) monitor and evaluate the fullllment of Government Assurances; (c) exercrse such other functions that are not covered by paragraphs (a) and (b) as may be allocated to the Committee by the Speaker from ttme to trme. 2) the Rule further states that, where the time frame rs not given by the Minister, the Committee shall determine the category within whrch rt falls and accordingly determrne the time frame within whrch rt ought to be implemented; The categortes shall rnclude - (, EmergencyAssurances. (ii) Short term Assurances. (rr4 MidtermAssurances. (ir) Long term Assurances. 3) The Chairpcrson oI the Govcrnment Assurances and Implementatton Commrttee sha1l present a report to the House on the Status of the rmplementatron and the extent to which the Assurances, Promises and Undertakings have been Fulfilled, Withdrawn or Broken from time to tlme. 4) the report submrtted under sub rule (3) sha1l be debated by the ou'' and; G6p\ 7 {-f tr s \ ,p1t-' &u 5) the Leader of Government Business shall respond to the issues raised during the debatc. -

Factors Affecting Adherence to National Malaria Treatment
Bawate et al. Malar J (2016) 15:112 DOI 10.1186/s12936-016-1153-5 Malaria Journal RESEARCH Open Access Factors affecting adherence to national malaria treatment guidelines in management of malaria among public healthcare workers in Kamuli District, Uganda Charles Bawate1,2,4* , Sylvia T. Callender‑Carter4, Ben Nsajju4 and Denis Bwayo3 Abstract Background: Malaria remains a major public health threat accounting for 30.4 % of disease morbidity in outpatient clinic visits across all age groups in Uganda. Consequently, malaria control remains a major public health priority in endemic countries such as Uganda. Experiences from other countries in Africa that revised their malaria case manage‑ ment suggest that health workers adherence may be problematic. Methods: A descriptive, cross-sectional design was used and collected information on health system, health workers and patients. Using log-binomial regression model, adjusted prevalence risk ratios (PRRs) and their associated 95 % confidence intervals were determined in line with adherence to new treatment guidelines of parasitological diagnosis and prompt treatment with artemisinin combination therapy (ACT). Results: Nine health centres, 24 health workers and 240 patient consultations were evaluated. Overall adherence to national malaria treatment guidelines (NMTG) was 50.6 % (122/241). It was significantly high at HC III [115 (53 %)] than at HC IV (29 %) [PRR 0.28 (95 % CI 0.148 0.52), p 0.000]. Compared to the nursing aide, the adherence level was 1.57 times higher among= enrolled nurses (p 0.004)= and 1.68 times higher among nursing officers, p 0.238, with statistical significance among the former. No= attendance of facility malaria-specific continuing medical= education (CME) sessions [PRR 1.9 (95 % CI 1.29 2.78), p 0.001] and no display of malaria treatment job aides in consultation rooms [PRR 0.64 (95= % CI 0.4 1.03), p 0.07] was= associated with increased adherence to guidelines with the former showing a statistical= significance and the= association of the latter borderline statistical significance. -

Assessment Form
Local Government Performance Assessment Kamuli District (Vote Code: 517) Assessment Scores Accountability Requirements % Crosscutting Performance Measures 59% Educational Performance Measures 68% Health Performance Measures 65% Water & Environment Performance Measures 75% 517 Accountability Requirements 2019 Kamuli District No. Summary of requirements Definition of compliance Compliance justification Compliant? Annual performance contract 1 Yes LG has submitted an annual • From MoFPED’s The Annual Performance Contract performance contract of the forthcoming inventory/schedule of LG for the forthcoming year 2020/21 year by June 30 on the basis of the submissions of was submitted on 17thJuly, 2019 PFMAA and LG Budget guidelines for performance contracts, and thus adhered to the adjusted the coming financial year. check dates of submission submission date of 31stAugust, and issuance of receipts 2019. and: o If LG submitted before or by due date, then state ‘compliant’ o If LG had not submitted or submitted later than the due date, state ‘non- compliant’ • From the Uganda budget website: www.budget.go.ug, check and compare recorded date therein with date of LG submission to confirm. Supporting Documents for the Budget required as per the PFMA are submitted and available 2 Yes LG has submitted a Budget that includes • From MoFPED’s Kamuli LG submitted the a Procurement Plan for the forthcoming inventory of LG budget approved Budget Estimates that FY by 30th June (LG PPDA submissions, check included a Procurement Plan for Regulations, 2006). whether: the FY 2019/20 on 17thJuly, 2019 thus being within the adjusted o The LG budget is submission date of 31st August, accompanied by a 2019. -

Strengthening TB and HIV&AIDS Responses in East-Central Uganda
S RESP AID ON & SE V S I IN H D E A N S A T B C T E G N N T I R N A E L H U T G G A N N E D R A T S Strengthening TB and HIV&AIDS Responses in East-Central Uganda (STAR-EC) PROGRAM YEAR II QUARTER TWO PROGRESS REPORT January - March, 2010 Funded by the United States Government through the US Agency for International Development under the terms of Agreement No. 617-A-00-09-0000700 THE REPUBLIC OF UGANDA Quarter Two Report, Jan - Mar, 2010 | 01 © 2010 Financial support for this program is provided by the United States Government through USAID, under Co- operative Agreement number 617-A-00-09-00007-00. The views expressed in this document do not necessarily reflect those of USAID. This program is implemented by JSI Research & Training Institute, Inc. in collaboration with World Education’s Bantwana Initiative, Communication for Development Foundation Uganda, mothers2mothers and Uganda Cares. Contents List of Tables .............................................................................................................................................................iii List of Figures ...........................................................................................................................................................iii List of Acronyms .......................................................................................................................................................iv 1.0 INTRODUCTION .......................................................................................................................................1