Strengthening TB and HIV&AIDS Responses in East-Central
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Vote:517 Kamuli District Quarter2
Local Government Quarterly Performance Report FY 2020/21 Vote:517 Kamuli District Quarter2 Terms and Conditions I hereby submit Quarter 2 performance progress report. This is in accordance with Paragraph 8 of the letter appointing me as an Accounting Officer for Vote:517 Kamuli District for FY 2020/21. I confirm that the information provided in this report represents the actual performance achieved by the Local Government for the period under review. Date: 11/02/2021 cc. The LCV Chairperson (District) / The Mayor (Municipality) 1 Local Government Quarterly Performance Report FY 2020/21 Vote:517 Kamuli District Quarter2 Summary: Overview of Revenues and Expenditures Overall Revenue Performance Ushs Thousands Approved Budget Cumulative Receipts % of Budget Received Locally Raised Revenues 545,891 373,486 68% Discretionary Government 4,425,320 2,335,957 53% Transfers Conditional Government Transfers 38,103,649 18,539,523 49% Other Government Transfers 1,995,208 612,466 31% External Financing 1,314,664 604,003 46% Total Revenues shares 46,384,732 22,465,434 48% Overall Expenditure Performance by Workplan Ushs Thousands Approved Cumulative Cumulative % Budget % Budget % Releases Budget Releases Expenditure Released Spent Spent Administration 5,566,664 2,817,313 2,271,323 51% 41% 81% Finance 500,261 242,532 192,277 48% 38% 79% Statutory Bodies 915,404 477,769 413,546 52% 45% 87% Production and Marketing 1,755,678 882,304 663,561 50% 38% 75% Health 9,769,288 4,987,922 4,043,308 51% 41% 81% Education 22,602,810 10,376,662 8,850,508 46% 39% 85% -

FY 2019/20 Vote:517 Kamuli District
LG Approved Workplan Vote:517 Kamuli District FY 2019/20 Foreword In accordance with Section 36 of the Local Government Act (Cap 243), Local Governments prepare appropriate plans and documents in conformity with Central Government guidelines and formats. Pursuant to the foregoing, Kamuli District Local Government has prepared the workplan for the FY2019/20. This document takes into consideration the 5 year District Development Plan for 2015/16 DQGLVWKHODVW\HDURILPSOHPHQWDWLRQRIWKHFXUUHQWSODQ7KH3ODQIRFXVHVRQWKHIROORZLQJNH\VWUDWHJLFREMHFWLYHVImprove household incomes through increased production promote and ensure the rational and sustainable utilization, development and effective management of environment and natural resources for socio-economic development. ECD programmes and LPSURYHPHQWRITXDOLW\HTXLW\UHWHQWLRQUHOHYDQFHDQGHIILFLHQF\LQEDVLFHGXFDWLRQDevelop adequate, reliable and efficient multi modal transport network in the district increasing access to safe water in rural and urban areas increasing sanitation and hygiene levels in rural and urban areas To contribute to the production of a healthy human capital through provision of equitable, safe and sustainable health services. Enhance effective participation of communities in the development process To improve service delivery across all sectors and lower level administrative units. Integration of cross cutting issues during planning, budgeting and implementation of development programs. The district has however continued to experience low/poor service delivery levels manifested by low household incomes, poor education standards, low level of immunization coverage, high maternal mortality rate, poor road network and low access to safe water among others. This district workplan focuses on a number of interventions aimed at addressing some of these challenges above through implementation of sector specific strategies highlight in the annual plans for FY 2019/20. -
Sustaining the Bee Keeping Program at Namasagali College in Kamuli
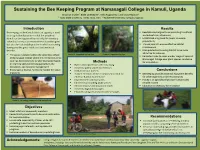
Sustaining the Bee Keeping Program at Namasagali College in Kamuli, Uganda Brooklyn Snyder1, Blake Lineweaver2, Mika Rugaramna3, and Grace Nabulo4, 1, 2Iowa State University, Ames, Iowa, USA 3, 4Makerere University, Kampala, Uganda Introduction Results Beekeeping, in the Kamuli district of Uganda, is used . Reestablished original hives according to cultural as an agricultural practice so that the people of and educational influencers Kamuli can be supported by not only the monetary . Established a log book for pupils to ensure value that honey as an entrepreneurial product gives productivity but also the sustainable practice in which consuming . Trained pupils to ensure effective habitat honey provides great nutritional and medicinal maintenance benefits. Manipulated surrounding habitat to be more attractive for colonies . The apiary is located within the secondary school Photo 2). Supported top bar hive Photo 3). Supported log hive . Relocated hives to cover a wider range of space at of Namasagali College where the entrepreneurship Namasagali College near plant species conducive club has direct access to be able to practice hands- Methods for colonization on learning skills concerning agriculture, the . Bated unoccupied hives with cow dung ecosystem, and business management . Created a pulley system for the hives . Encourages a diverse, functional habitat for native . Contacted local farmers Conclusions organisms . Trained members of the entrepreneurial club for . Beekeeping provides essential ecosystem benefits effective habitat maintenance for other organisms and the community . Implemented sunflower plots . Honey is an agricultural product that provides . Identified surrounding plant species reliable income . Cleared invasive and unwanted brush . Education is necessary for innovation . Created a log book for pupils . -

Medicines Consumer Awareness Campaign Project Report
MEDICINES CONSUMER AWARENESS CAMPAIGN PROJECT REPORT 2017 This report is made possible by the support of the American People through the United States Agency for International Development (USAID). The contents of this report are the sole responsibility of Cardno Emerging Markets USA, Ltd. and do not necessarily reflect the views of USAID or the United States Government. CONSUMER AWARENESS CAMPAIGN PROJECT REPORT Authors: Coalition for Health Promotion and Social Development (HEPS Uganda) Submitted by: Cardno Emerging Markets USA, Ltd. Submitted to: USAID/Uganda Contract No.: AID-617-C-13-00005 DISCLAIMER The author’s views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States Government. Consumer Awareness Campaign Project Report 2 TABLE OF CONTENTS ABBREVIATION........................................................................................................................................................................ 4 ACKNOWLEDGEMENT ........................................................................................................................................................ 5 EXECUTIVE SUMMARY ......................................................................................................................................................... 6 1. BACKGROUND ............................................................................................................................................................. 7 1.1 Introduction -

Vote:017 Ministry of Energy and Mineral Development
Vote Performance Report Financial Year 2018/19 Vote:017 Ministry of Energy and Mineral Development QUARTER 1: Highlights of Vote Performance V1: Summary of Issues in Budget Execution Table V1.1: Overview of Vote Expenditures (UShs Billion) Approved Cashlimits Released Spent by % Budget % Budget % Releases Budget by End Q1 by End Q 1 End Q1 Released Spent Spent Recurrent Wage 6.225 1.556 1.556 1.152 25.0% 18.5% 74.1% Non Wage 85.788 16.876 16.876 15.937 19.7% 18.6% 94.4% Devt. GoU 325.227 165.045 165.045 139.862 50.7% 43.0% 84.7% Ext. Fin. 1,339.221 258.273 258.273 360.077 19.3% 26.9% 139.4% GoU Total 417.240 183.477 183.477 156.952 44.0% 37.6% 85.5% Total GoU+Ext Fin 1,756.460 441.750 441.750 517.029 25.1% 29.4% 117.0% (MTEF) Arrears 0.242 0.173 0.173 0.000 71.4% 0.0% 0.0% Total Budget 1,756.702 441.922 441.922 517.029 25.2% 29.4% 117.0% A.I.A Total 0.000 0.000 0.000 0.000 0.0% 0.0% 0.0% Grand Total 1,756.702 441.922 441.922 517.029 25.2% 29.4% 117.0% Total Vote Budget 1,756.460 441.750 441.750 517.029 25.1% 29.4% 117.0% Excluding Arrears Table V1.2: Releases and Expenditure by Program* Billion Uganda Shillings Approved Released Spent % Budget % Budget %Releases Budget Released Spent Spent Program: 0301 Energy Planning,Management & 890.50 253.99 214.55 28.5% 24.1% 84.5% Infrastructure Dev't Program: 0302 Large Hydro power infrastructure 751.03 145.75 285.22 19.4% 38.0% 195.7% Program: 0303 Petroleum Exploration, Development, 57.93 22.14 6.98 38.2% 12.0% 31.5% Production, Value Addition and Distribution and Petrolleum Products Program: -

Kamuli DLG.Pdf
Local Government Workplan Vote: 517 Kamuli District Structure of Workplan Foreword Executive Summary A: Revenue Performance and Plans B: Summary of Department Performance and Plans by Workplan C: Draft Annual Workplan Outputs for 2016/17 D: Details of Annual Workplan Activities and Expenditures for 2016/17 Page 1 Local Government Workplan Vote: 517 Kamuli District Foreword In accordance with Section 36 of the Local Government Act (Cap 243), Local Governments prepare appropriate plans and documents in conformity with Central Government guidelines and formats. Pursuant to the foregoing, Kamuli District Local Government has prepared this annual workplan and budget for the period 2016/17. This document was developed through a participatory process that brought on board different stakeholders in a bottom up planning approach starting at village level and climaxed by the District Budget conference in which development partners participated among others. This document takes into consideration the District Development Plan II for 2015/16 -2019/20. The Development Plans focuses on the following key strategic objectives; • To improve household incomes and promote food security, • To promote good governance, • Enhancement of local revenue collection using best practices, • Improve the stock and quality of road infrastructure. • Increasing safe water coverage and sanitation in the district, • Increase access, quality and equity of education for girls and boys • Improvement in the quality of health care services, The district has however continued to experience low/poor service delivery levels manifested by low household incomes, poor education standards, low level of immunization coverage, high maternal mortality rate, poor road network and low access to safe water among others. -

WHO UGANDA BULLETIN February 2016 Ehealth MONTHLY BULLETIN
WHO UGANDA BULLETIN February 2016 eHEALTH MONTHLY BULLETIN Welcome to this 1st issue of the eHealth Bulletin, a production 2015 of the WHO Country Office. Disease October November December This monthly bulletin is intended to bridge the gap between the Cholera existing weekly and quarterly bulletins; focus on a one or two disease/event that featured prominently in a given month; pro- Typhoid fever mote data utilization and information sharing. Malaria This issue focuses on cholera, typhoid and malaria during the Source: Health Facility Outpatient Monthly Reports, Month of December 2015. Completeness of monthly reporting DHIS2, MoH for December 2015 was above 90% across all the four regions. Typhoid fever Distribution of Typhoid Fever During the month of December 2015, typhoid cases were reported by nearly all districts. Central region reported the highest number, with Kampala, Wakiso, Mubende and Luweero contributing to the bulk of these numbers. In the north, high numbers were reported by Gulu, Arua and Koti- do. Cholera Outbreaks of cholera were also reported by several districts, across the country. 1 Visit our website www.whouganda.org and follow us on World Health Organization, Uganda @WHOUganda WHO UGANDA eHEALTH BULLETIN February 2016 Typhoid District Cholera Kisoro District 12 Fever Kitgum District 4 169 Abim District 43 Koboko District 26 Adjumani District 5 Kole District Agago District 26 85 Kotido District 347 Alebtong District 1 Kumi District 6 502 Amolatar District 58 Kween District 45 Amudat District 11 Kyankwanzi District -

Jinja District Local Government Councils' Scorecard FY 2018/19
jinja DISTRICT LOCAL GOVERNMENT council SCORECARD assessment FY 2018/19 jinja DISTRICT LOCAL GOVERNMENT council SCORECARD assessment FY 2018/19 L-R: Ms. Rose Gamwera, Secretary General ULGA; Mr. Ben Kumumanya, PS. MoLG and Dr. Arthur Bainomugisha, Executive Director ACODE in a group photo with award winners at the launch of the 8th Local Government Councils Scorecard Report FY 2018/19 at Hotel Africana in Kampala on 10th March 2020 1.0 Introduction 1.2 The Local Government Councils Scorecard Initiative (LGCSCI) This brief was developed from the scorecard report The main building blocks in LGCSCI are the principles titled, “The Local Government Councils Scorecard and core responsibilities of Local Governments FY 2018/19. “The Next Big Steps: Consolidating as set out in Chapter 11 of the Constitution of the Gains of Decentralisation and Repositioning the Republic of Uganda, the Local Governments Act Local Government Sector in Uganda.” The brief (CAP 243) under Section 10 (c), (d) and (e). The provides key highlights of the performance of district scorecard comprises of five parameters based on elected leaders and the Council of Jinja District the core responsibilities of the local government Local Government (JDLG) during FY 2018/19. Councils, District Chairpersons, Speakers and 1.1 About the District Individual Councillors. These are classified into five categories: Financial management and oversight; Jinja District is located approximately 87 kilometres Political functions and representation; Legislation by road, east of Kampala, comprising one of the nine and related functions; Development planning and (9) districts of Busoga region with its Headquarters constituency servicing and Monitoring service located at Busoga Square within Jinja Municipality. -

Impact of Nutrition Education Centers on Food and Nutrition Security in Kamuli District, Uganda Samuel Ikendi Iowa State University
Iowa State University Capstones, Theses and Graduate Theses and Dissertations Dissertations 2019 Impact of nutrition education centers on food and nutrition security in Kamuli District, Uganda Samuel Ikendi Iowa State University Follow this and additional works at: https://lib.dr.iastate.edu/etd Part of the Agriculture Commons Recommended Citation Ikendi, Samuel, "Impact of nutrition education centers on food and nutrition security in Kamuli District, Uganda" (2019). Graduate Theses and Dissertations. 17032. https://lib.dr.iastate.edu/etd/17032 This Thesis is brought to you for free and open access by the Iowa State University Capstones, Theses and Dissertations at Iowa State University Digital Repository. It has been accepted for inclusion in Graduate Theses and Dissertations by an authorized administrator of Iowa State University Digital Repository. For more information, please contact [email protected]. Impact of nutrition education centers on food and nutrition security in Kamuli District, Uganda by Samuel Ikendi A thesis submitted to the graduate faculty in partial fulfillment of the requirements for the degree of MASTER OF COMMUNITY AND REGIONAL PLANNING MASTER OF SCIENCE Co-majors: Community and Regional Planning; Sustainable Agriculture Program of Study Committee: Francis Owusu, Major Professor Carmen Bain Ann Oberhauser The student author, whose presentation of the scholarship herein was approved by the program of study committee, is solely responsible for the content of this thesis. The Graduate College will ensure this thesis is globally accessible and will not permit alterations after a degree is conferred. Iowa State University Ames, Iowa 2019 Copyright © Samuel Ikendi, 2019. All rights reserved. ii DEDICATION To the NECs hosts, NEC Trainers, and my mum Christine Lubaale, may the Gracious Lord reward you all abundantly for your generosity. -

Kamuli District Local Government Performance Assessment Report
Local Government Performance Assessment Kamuli District (Vote Code: 517) Assessment Scores Accountability Requirements 83% Crosscutting Performance Measures 59% Educational Performance Measures 68% Health Performance Measures 65% Water Performance Measures 75% 517 Kamuli District Accountability Requirements 2019 Summary of requirements Definition of compliance Compliance justification Compliant? Annual performance contract Yes LG has submitted an annual performance • From MoFPED’s The Annual Performance Contract for the contract of the forthcoming year by June 30 on inventory/schedule of LG forthcoming year 2020/21 was submitted the basis of the PFMAA and LG Budget submissions of performance on 17thJuly, 2019 and thus adhered to guidelines for the coming financial year. contracts, check dates of the adjusted submission date of submission and issuance of 31stAugust, 2019. receipts and: o If LG submitted before or by due date, then state ‘compliant’ o If LG had not submitted or submitted later than the due date, state ‘non- compliant’ • From the Uganda budget website: www.budget.go.ug, check and compare recorded date therein with date of LG submission to confirm. Supporting Documents for the Budget required as per the PFMA are submitted and available Yes LG has submitted a Budget that includes a • From MoFPED’s inventory Kamuli LG submitted the approved Procurement Plan for the forthcoming FY by of LG budget submissions, Budget Estimates that included a 30th June (LG PPDA Regulations, 2006). check whether: Procurement Plan for the FY 2019/20 on 17thJuly, 2019 thus being within the o The LG budget is adjusted submission date of 31st August, accompanied by a 2019. Procurement Plan or not. -

Emergency Health Fiscal and Growth Stabilization and Development
LIST OF COVID-19 QUARANTINE CENTRES IN WATER AND POWER UTILITIES OPERATION AREAS WATER S/N QUARANTINE CENTRE LOCATION POWER UTILITY UTILITY 1 MASAFU GENERAL HOSPITAL BUSIA UWS-E UMEME LTD 2 BUSWALE SECONDARY SCHOOL NAMAYINGO UWS-E UMEME LTD 3 KATAKWI ISOLATION CENTRE KATAKWI UWS-E UMEME LTD 4 BUKWO HC IV BUKWO UWS-E UMEME LTD 5 AMANANG SECONDARY SCHOOL BUKWO UWS-E UMEME LTD 6 BUKIGAI HC III BUDUDA UWS-E UMEME LTD 7 BULUCHEKE SECONDARY SCHOOL BUDUDA UWS-E UMEME LTD 8 KATIKIT P/S-AMUDAT DISTRICT KATIKIT UWS-K UEDCL 9 NAMALU P/S- NAKAPIRIPIRIT DISTRICT NAMALU UWS-K UEDCL 10 ARENGESIEP S.S-NABILATUK DISTRICT ARENGESIEP UWS-K UEDCL 11 ABIM S.S- ABIM DISTRICT ABIM UWS-K UEDCL 12 KARENGA GIRLS P/S-KARENGA DISTRICT KARENGA UWS-K UMEME LTD 13 NAKAPELIMORU P/S- KOTIDO DISTRICT NAKAPELIMORU UWS-K UEDCL KOBULIN VOCATIONAL TRAINING CENTER- 14 NAPAK UWS-K UEDCL NAPAK DISTRICT 15 NADUNGET HCIII -MOROTO DISTRICT NADUNGET UWS-K UEDCL 16 AMOLATAR SS AMOLATAR UWS-N UEDCL 17 OYAM OYAM UWS-N UMEME LTD 18 PADIBE IN LAMWO DISTRICT LAMWO UWS-N UMEME LTD 19 OPIT IN OMORO OMORO UWS-N UMEME LTD 20 PABBO SS IN AMURU AMURU UWS-N UEDCL 21 DOUGLAS VILLA HOSTELS MAKERERE NWSC UMEME LTD 22 OLIMPIA HOSTEL KIKONI NWSC UMEME LTD 23 LUTAYA GEOFREY NAJJANANKUMBI NWSC UMEME LTD 24 SEKYETE SHEM KIKONI NWSC UMEME LTD PLOT 27 BLKS A-F AKII 25 THE EMIN PASHA HOTEL NWSC UMEME LTD BUA RD 26 ARCH APARTMENTS LTD KIWATULE NWSC UMEME LTD 27 ARCH APARTMENTS LTD KIGOWA NTINDA NWSC UMEME LTD 28 MARIUM S SANTA KYEYUNE KIWATULE NWSC UMEME LTD JINJA SCHOOL OF NURSING AND CLIVE ROAD JINJA 29 MIDWIFERY A/C UNDER MIN.OF P.O.BOX 43, JINJA, NWSC UMEME LTD EDUCATION& SPORTS UGANDA BUGONGA ROAD FTI 30 MAAIF(FISHERIES TRAINING INSTITUTE) NWSC UMEME LTD SCHOOL PLOT 4 GOWERS 31 CENTRAL INN LIMITED NWSC UMEME LTD ROAD PLOT 2 GOWERS 32 CENTRAL INN LIMITED NWSC UMEME LTD ROAD PLOT 45/47 CHURCH 33 CENTRAL INN LIMITED NWSC UMEME LTD RD CENTRAL I INSTITUTE OF SURVEY & LAND PLOT B 2-5 STEVEN 34 NWSC 0 MANAGEMENT KABUYE CLOSE 35 SURVEY TRAINING SCHOOL GOWERS PARK NWSC 0 DIVISION B - 36 DR. -
2018 Annual Report
Sustaining Connections That Matter Center for Sustainable Rural Livelihoods 2018 DONOR IMPACT REPORT A Message from the President In the year 2050, a gathering will Dear People of the Year 2050: take place at the Mpirigiti Rural Training Centre in the Kamuli Greetings from the year 2018! This year we dedicated the Mpirigiti Rural Training Centre. It is a District of Uganda. The purpose wonderful new facility. We trust the passing years have made the Mpirigiti center a hopeful destination of the assembled group will be for many thousands of people — those who have come eager to learn, those who have come willing to to open a time capsule from the serve, and those who have been blessed by working together to pursue a happier, hope-filled future. year 2018. In our current world of 2018, we often talk about “2050” as an important year — a time for which we The time capsule was sealed must direct our energies now to ensure that expanding world populations have enough nourishing this past July when I was food to eat and are able to lead healthy, satisfying lives. “Food is the moral right of all who are born honored to be present to help into this world” — That’s what Norman Borlaug, a famous Iowan, agricultural scientist and Nobel dedicate the new training center Prize laureate, once said. We hope 2050 finds that all people have attained this moral right. for the Center for Sustainable Rural Livelihoods. For nearly 15 Here are the main messages I’d like to share with you: years, we have worked hand- 2018 DONOR IMPACT REPORT 2018 DONOR IMPACT in-hand with the people of the To the people of the Kamuli District in 2050: Sustain our friendship and partnership many years into DS Kamuli District to make their the future.