Kenya Coordinating Mechanism Oversight Field Visit Report for Kwale
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

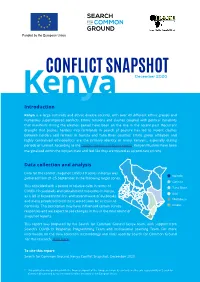
County Urban Governance Tools
County Urban Governance Tools This map shows various governance and management approaches counties are using in urban areas Mandera P Turkana Marsabit P West Pokot Wajir ish Elgeyo Samburu Marakwet Busia Trans Nzoia P P Isiolo P tax Bungoma LUFs P Busia Kakamega Baringo Kakamega Uasin P Gishu LUFs Nandi Laikipia Siaya tax P P P Vihiga Meru P Kisumu ga P Nakuru P LUFs LUFs Nyandarua Tharaka Garissa Kericho LUFs Nithi LUFs Nyeri Kirinyaga LUFs Homa Bay Nyamira P Kisii P Muranga Bomet Embu Migori LUFs P Kiambu Nairobi P Narok LUFs P LUFs Kitui Machakos Kisii Tana River Nyamira Makueni Lamu Nairobi P LUFs tax P Kajiado KEY County Budget and Economic Forums (CBEFs) They are meant to serve as the primary institution for ensuring public participation in public finances in order to im- Mom- prove accountability and public participation at the county level. basa Baringo County, Bomet County, Bungoma County, Busia County,Embu County, Elgeyo/ Marakwet County, Homabay County, Kajiado County, Kakamega County, Kericho Count, Kiambu County, Kilifi County, Kirin- yaga County, Kisii County, Kisumu County, Kitui County, Kwale County, Laikipia County, Machakos Coun- LUFs ty, Makueni County, Meru County, Mombasa County, Murang’a County, Nairobi County, Nakuru County, Kilifi Nandi County, Nyandarua County, Nyeri County, Samburu County, Siaya County, TaitaTaveta County, Taita Taveta TharakaNithi County, Trans Nzoia County, Uasin Gishu County Youth Empowerment Programs in urban areas In collaboration with the national government, county governments unveiled -
Presentation on the 5Th Inter-Regional Meeting Of
PRESENTATION ON THE 5TH INTER‐REGIONAL MEETING OF NATIONAL COMMISSIONS FOR UNESCO TO BE HOSTED IN KENYA, 19‐21 JUNE 2018, DIANI, KENYA By: Dr Evangeline Njoka, MBS Secretary General, Kenya National Commission for UNESCO 11th April, 2018 Where is Kenya? Venue for Meeting • The Leisure Lodge Beach and Golf Resort situated on the World famous Diani Beach on the Kenyan Coast, south of Mombasa. • Diani Beach voted as one of the top ten beaches in Africa in 2017. • Diani is a comfortable and safe area, which regularly hosts national and international conferences, as an alternate for Nairobi and Mombasa. LOCATION OF LEISURE LODGE & GOLF RESORT 42.5 KM from Moi International Airport Approx: 1 h 37 min by road; 15 min from Ukunda Airtrip Kenya Visa Application • Kenyan visa costs about $50 USD • Kenya visa application process automated since April 2015. • Delegates are required to apply online through: http://evisa.go.ke/evisa.html • Inasmuch as the visa takes 2 to 5 working days, one is encouraged to apply in good time. Travelling to Diani, Kenya (1) Visa Application…contd • Passports should be valid for a period of at least six months after the date of arrival. • For some countries visa is not required if the stay is less than 90 day. • Also delegates from some few countries cannot make visa application online, so they must visit the nearest Kenya embassy / consulate. • For more information including on countries exempted, please see https://immigration.ecitizen.go.ke/index.php?id=6 Travelling to Diani, Kenya (2) • Most flights from Europe and Asia fly to Jomo Kenyatta International Airport (JKIA), Nairobi, a Regional hub. -

Second Health Strategic and Investment Plan (Chsip Ii)
MOMBASA COUNTY of HealthDepartment Services SECOND HEALTH STRATEGIC AND INVESTMENT PLAN (CHSIP II) 2018 – 2022 A Healthy and Productive Community Abridged Version August 2018 CONTENTS CONTENTS ii ABBREVIATIONS iii LIST OF FIGURES v LIST OF TABLES 6 Foreword 7 Acknowledgment 8 Executive Summary 9 1 COUNTY INSTITUTIONAL REVIEW 1 1.1 About Mombasa County ........................................................................................................ 1 1.2 Population Demographics...................................................................................................... 3 1.3 County Health Sector............................................................................................................. 3 1.4 Purpose of the Second County Health Sector Strategic and Investment Plan (CHSIP II) 2018-2022 .............................................................................................................................. 4 1.5 County Performance Management Framework ..................................................................... 5 1.6 The Planning Process............................................................................................................. 6 1.7 Mission, Vision and Values ................................................................................................... 7 2 SITUATION ANALYSIS 8 2.1 Summary of County Health Sector Performance 2013/14 – 2017/18 ................................... 8 2.2 Situation Analysis ................................................................................................................. -

Kenya, Groundwater Governance Case Study
WaterWater Papers Papers Public Disclosure Authorized June 2011 Public Disclosure Authorized KENYA GROUNDWATER GOVERNANCE CASE STUDY Public Disclosure Authorized Albert Mumma, Michael Lane, Edward Kairu, Albert Tuinhof, and Rafik Hirji Public Disclosure Authorized Water Papers are published by the Water Unit, Transport, Water and ICT Department, Sustainable Development Vice Presidency. Water Papers are available on-line at www.worldbank.org/water. Comments should be e-mailed to the authors. Kenya, Groundwater Governance case study TABLE OF CONTENTS PREFACE .................................................................................................................................................................. vi ACRONYMS AND ABBREVIATIONS ................................................................................................................................ viii ACKNOWLEDGEMENTS ................................................................................................................................................ xi EXECUTIVE SUMMARY ............................................................................................................................................... xiv 1. INTRODUCTION ............................................................................................................................................. 1 1.1. GROUNDWATER: A COMMON RESOURCE POOL ....................................................................................................... 1 1.2. CASE STUDY BACKGROUND ................................................................................................................................. -

Citizens' Perception of Leadership During COVID-19 Times in Mombasa, Kenya
Citizens’ Perception of Leadership during COVID-19 Times in Mombasa, Kenya Fathima Azmiya Badurdeen To cite this version: Fathima Azmiya Badurdeen. Citizens’ Perception of Leadership during COVID-19 Times in Mombasa, Kenya. 2020, https://mambo.hypotheses.org/2853. halshs-03078567 HAL Id: halshs-03078567 https://halshs.archives-ouvertes.fr/halshs-03078567 Submitted on 16 Dec 2020 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Institut français de recherche en Afrique French Institute for Research in Africa MAMBO! XVII (4), 2020 COVID-19 Special Papers Citizens’ Perception of Leadership during COVID-19 Times in Mombasa, Kenya Fathima AZMIYA BADURDEEN Cite: AZMIYA BADURDEEN, Fathima. 2020. Citizens’ Perception of Leadership during COVID-19 Times in Mombasa, Kenya. Mambo! vol. XVII, no. 4. URL: https://mambo.hypotheses.org/2853 The author: Dr. Fathima Azmiya Badurdeen is a lecturer in Development Studies at the Department of Social Sciences, Technical University of Mombasa, working on issues related to youth, gender and violent extremism. The article is an outcome of the research funded by the French Institute for Research in Africa (IFRA) from April to September 2020. Email: [email protected]. -
CONFLICT SNAPSHOT Kenya December 2020 Introduction
Funded by the European Union CONFLICT SNAPSHOT Kenya December 2020 Introduction Kenya is a large culturally and ethnic diverse country, with over 40 different ethnic groups and numerous superimposed conflicts. Ethnic tensions and clashes coupled with political instability that manifests during the election period have been on the rise in the recent past. Recurrent drought that pushes herders into farmlands in search of pasture has led to violent clashes between herders and farmers in Garissa and Tana River counties. Ethnic group affiliation and highly centralised ethnopolitics are the primary identity of many Kenyans, especially during periods of turmoil. According to the Conflict Analysis of Kenya report, Kenyan Muslims have been marginalised within the Kenyan state and feel like they are treated as second-rate citizens. Data collection and analysis Data for the conflict snapshot COVID-19 series in Kenya was airoi gathered from 21-25 September in the following target zones: arissa This coincided with a period of relative calm in terms of ana iver COVID-19 caseloads and containment measures in Kenya, Kilifi as it fell in between the first and second wave of outbreaks omasa and many people believed there would soon be a return to normalcy. This perception may have influenced certain survey wale responses and we expect to see changes in this in the next round of snapshot reports. This report was prepared by the Search for Common Ground Kenya team, with support from Search’s COVID-19 Response Programming Team and Institutional Learning Team. For more information on the data collection methodology and tools used by Search for Common Ground for this research, click here. -

Mombasa County Crime and Violence Report
MOMBASA COUNTY CRIME AND VIOLENCE RAPID ASSESSMENT MOMBASA COUNTY CRIME AND VIOLENCE RAPID ASSESSMENT Cover photo credit: Andrea Albini | Creative Commons 3.0 Design and copy editing: Laura C. Johnson II Contents Foreword .................................................v Acknowledgements .........................................vi Acronyms ................................................vii 1 Introduction .............................................1 Crime and Violence Prevention in Kenya ...............................3 Crime and Violence Prevention Training ...............................4 County-Level Crime and Violence Prevention ..........................4 Framework for Analysis .............................................7 Goals of the Rapid Assessment ......................................9 Methodology . .9 2 Background: Crime and Violence Trends in Kenya ............13 Boda-Boda-Related Crime and Violence .............................14 Alcohol and Drug Abuse ...........................................14 Sexual and Gender-Based Violence ..................................16 Violence against Children ..........................................16 Radicalization and Recruitment into Violent Extremism ..................17 3 Rapid Assessment of Mombasa County .....................19 Overview of County ...............................................19 Cross-Cutting Drivers of Crime and Violence ..........................20 Dynamics of Crime and Violence ....................................23 Security Interventions .............................................40 -

(Nema)Table of Contents
ENVIR ONMENTAL AND SOCIAL IMPACT ASSESSMENT REPORT (ESIA) AND RESETLEMENT ACTION PLAN (RAP) FOR THE PROPSED MALINDI AIRPORT RUNWAY EXPANSION PROJECT TENDER NO. KAA/OT/MLD/1507/2018/2019 NOVEMBER, 2020 KENYA AIRPORTS AUTHORITY ESIA and RAP report for the proposed Extension of Malindi Airport Runway CERTIFICATION This ESIA study report has been prepared in accordance with the Environmental Management and Coordination Act (EMCA) 1999 and the Environmental (Impact Assessment and Audit) Regulations 2003 for submission to the National Environment Management Authority (NEMA). The following experts conducted the study and prepared this report on behalf of Eco-solutions Limited: FOR Eco Solutions Limited, iPlan Consult (Int’l) Limited, P.O. BOX 20492 – 00100, P.O BOX 28634-00100 NAIROBI, KENYA. NAIROBI. TEL: +254 722 273935. TEL: +254 721891005. Email: [email protected] Email: [email protected] Name Designation NEMA Date & Signature REG. NO. 1. SHADRACK K. MBUTA EIA LEAD EXPERT 6315 2. WALLACE ISABOKE EIA LEAD EXPERT 2622 3. CYNTHIA OTARA ASS. EXPERT 11450 The Proponent; Kenya Airports Authority (KAA), P.O. Box 19001-00501, Nairobi. Signature___________________________ Date_____________________________ Designation: Environment Manager Disclaimer: This ESIA Report is confidential to Kenya Airports Authority (KAA), and any use of the materials hereof should be strictly in accordance with the contractual agreement between Eco-solutions and Kenya Airports Authority (KAA). It is, however, subject to conditions spelt out in the Environmental (Impact Assessment and Audit) Regulations, 2003. Eco Solutions Ltd; iPlan Consult (Int’l) Limited November 2020 2 KENYA AIRPORTS AUTHORITY ESIA and RAP report for the proposed Extension of Malindi Airport Runway EXECUTIVE SUMMARY 1. -

Registered Voters Per Caw for 2017 General Elections
REGISTERED VOTERS PER CAW FOR 2017 GENERAL ELECTIONS NO. OF COUNTY CONST_ CAW_ COUNTY_NAME CONSTITUENCY_NAME CAW_NAME VOTERS POLLING _CODE CODE CODE STATIONS 001 MOMBASA 001 CHANGAMWE 0001 PORT REITZ 17,082 26 001 MOMBASA 001 CHANGAMWE 0002 KIPEVU 13,608 22 001 MOMBASA 001 CHANGAMWE 0003 AIRPORT 16,606 26 001 MOMBASA 001 CHANGAMWE 0004 CHANGAMWE 17,586 29 001 MOMBASA 001 CHANGAMWE 0005 CHAANI 21,449 33 001 MOMBASA 002 JOMVU 0006 JOMVU KUU 22,269 36 001 MOMBASA 002 JOMVU 0007 MIRITINI 16,899 27 001 MOMBASA 002 JOMVU 0008 MIKINDANI 30,139 46 001 MOMBASA 003 KISAUNI 0009 MJAMBERE 22,384 34 001 MOMBASA 003 KISAUNI 0010 JUNDA 23,979 37 001 MOMBASA 003 KISAUNI 0011 BAMBURI 17,685 28 001 MOMBASA 003 KISAUNI 0012 MWAKIRUNGE 4,946 9 001 MOMBASA 003 KISAUNI 0013 MTOPANGA 17,539 28 001 MOMBASA 003 KISAUNI 0014 MAGOGONI 14,846 23 001 MOMBASA 003 KISAUNI 0015 SHANZU 24,772 39 001 MOMBASA 004 NYALI 0016 FRERE TOWN 20,215 33 001 MOMBASA 004 NYALI 0017 ZIWA LA NG'OMBE 20,747 31 001 MOMBASA 004 NYALI 0018 MKOMANI 19,669 31 001 MOMBASA 004 NYALI 0019 KONGOWEA 24,457 38 001 MOMBASA 004 NYALI 0020 KADZANDANI 18,929 32 001 MOMBASA 005 LIKONI 0021 MTONGWE 13,149 23 001 MOMBASA 005 LIKONI 0022 SHIKA ADABU 13,089 21 001 MOMBASA 005 LIKONI 0023 BOFU 18,060 28 001 MOMBASA 005 LIKONI 0024 LIKONI 10,855 17 001 MOMBASA 005 LIKONI 0025 TIMBWANI 32,173 51 001 MOMBASA 006 MVITA 0026 MJI WA KALE/MAKADARA 19,927 34 001 MOMBASA 006 MVITA 0027 TUDOR 20,380 35 001 MOMBASA 006 MVITA 0028 TONONOKA 21,055 36 001 MOMBASA 006 MVITA 0029 SHIMANZI/GANJONI 17,312 33 001 MOMBASA -

Out Patient Facilities for Nhif Supa Cover Baringo County Bomet County Bungoma County Busia County
OUT PATIENT FACILITIES FOR NHIF SUPA COVER BARINGO COUNTY BRANCH No HOSPITAL NAME POSTAL ADDRESS OFFICE 1 TIONYBEI MEDICAL CLINIC 396-30400, KABARNET KABARNET 2 BARINGO DISTRICT HOSPITAL (KABARNET) 21-30400, KABARNET KABARNET 3 REALE MEDICAL CENTRE-KABARNET 4694-30100, ELDORET KABARNET 4 KERIO HOSPITAL LTD 458-30400, KABARNET KABARNET 5 RAVINE GLORY HEALTH CARE SERVICES 612-20103, ELDAMA RAVINE KABARNET 6 ELDAMA RAVINE NURSING HOME 612-20103, ELDAMA RAVINE KABARNET 7 BARNET MEMORIAL MEDICAL CENTRE 490-30400, KABARNET KABARNET BOMET COUNTY BRANCH No HOSPITAL NAME POSTAL ADDRESS OFFICE 1 CHELYMO MEDICAL CENTRE 37-20422 SILIBWET BOMET 2 KAPKOROS HEALTH CENTRE 20400 BOMET BOMET BUNGOMA COUNTY BRANCH No HOSPITAL NAME POSTAL ADDRESS OFFICE 1 CHWELE SUBCOUNTY HOSPITAL 202 - 50202 CHWELE BUNGOMA 2 LUMBOKA MEDICAL SERVICES 1883 - 50200 BUNGOMA BUNGOMA 3 WEBUYE HEALTH CENTRE 25 - WEBUYE BUNGOMA 4 ST JAMES OPTICALS 2141 50200 BUNGOMA 5 NZOIA MEDICAL CENTRE 471 - 50200 BUNGOMA BUNGOMA 6 TRINITY OPTICALS LIMITED PRIVATE BAG BUNGOMA BUNGOMA 7 KHALABA MEDICAL SERVICES 2211- 50200 BUNGOMA BUNGOMA 8 ARARAT MEDICAL CLINIC 332 KIMILILI BUNGOMA 9 SIRISIA SUBDISTRICT HOSPITAL 122 - 50208 SIRISIA BUNGOMA 10 NZOIA MEDICAL CENTRE - CHWELE 471 - 50200 BUNGOMA BUNGOMA 11 OPEN HEART MEDICAL CENTRE 388 - 50202 CHWELE BUNGOMA 12 ICFEM DREAMLAND MISSION HOSPITAL PRIVATE BAG KIMILILI BUNGOMA 13 EMMANUEL MISSION HEALTH CENTRE 53 - 50207 MISIKHU BUNGOMA 14 WEBUYE DISTRICT HOSPITAL 25 - 50205 BUNGOMA 15 ELGON VIEW MEDICAL COTTAGE 1747 - 50200 BUNGOMA BUNGOMA 16 FRIENDS -

County Name County Code Location
COUNTY NAME COUNTY CODE LOCATION MOMBASA COUNTY 001 BANDARI COLLEGE KWALE COUNTY 002 KENYA SCHOOL OF GOVERNMENT MATUGA KILIFI COUNTY 003 PWANI UNIVERSITY TANA RIVER COUNTY 004 MAU MAU MEMORIAL HIGH SCHOOL LAMU COUNTY 005 LAMU FORT HALL TAITA TAVETA 006 TAITA ACADEMY GARISSA COUNTY 007 KENYA NATIONAL LIBRARY WAJIR COUNTY 008 RED CROSS HALL MANDERA COUNTY 009 MANDERA ARIDLANDS MARSABIT COUNTY 010 ST. STEPHENS TRAINING CENTRE ISIOLO COUNTY 011 CATHOLIC MISSION HALL, ISIOLO MERU COUNTY 012 MERU SCHOOL THARAKA-NITHI 013 CHIAKARIGA GIRLS HIGH SCHOOL EMBU COUNTY 014 KANGARU GIRLS HIGH SCHOOL KITUI COUNTY 015 MULTIPURPOSE HALL KITUI MACHAKOS COUNTY 016 MACHAKOS TEACHERS TRAINING COLLEGE MAKUENI COUNTY 017 WOTE TECHNICAL TRAINING INSTITUTE NYANDARUA COUNTY 018 ACK CHURCH HALL, OL KALAU TOWN NYERI COUNTY 019 NYERI PRIMARY SCHOOL KIRINYAGA COUNTY 020 ST.MICHAEL GIRLS BOARDING MURANGA COUNTY 021 MURANG'A UNIVERSITY COLLEGE KIAMBU COUNTY 022 KIAMBU INSTITUTE OF SCIENCE & TECHNOLOGY TURKANA COUNTY 023 LODWAR YOUTH POLYTECHNIC WEST POKOT COUNTY 024 MTELO HALL KAPENGURIA SAMBURU COUNTY 025 ALLAMANO HALL PASTORAL CENTRE, MARALAL TRANSZOIA COUNTY 026 KITALE MUSEUM UASIN GISHU 027 ELDORET POLYTECHNIC ELGEYO MARAKWET 028 IEBC CONSTITUENCY OFFICE - ITEN NANDI COUNTY 029 KAPSABET BOYS HIGH SCHOOL BARINGO COUNTY 030 KENYA SCHOOL OF GOVERNMENT, KABARNET LAIKIPIA COUNTY 031 NANYUKI HIGH SCHOOL NAKURU COUNTY 032 NAKURU HIGH SCHOOL NAROK COUNTY 033 MAASAI MARA UNIVERSITY KAJIADO COUNTY 034 MASAI TECHNICAL TRAINING INSTITUTE KERICHO COUNTY 035 KERICHO TEA SEC. SCHOOL -

Interruption of Electricity Supply
NYANDARUA COUNTY Interruption of AREA: RUMURUTI, MARALAL DATE: Thursday 05.03.2020 TIME: 8.00 A.M. – 5.00 P.M. Electricity Supply Rumuruti Muthaiga, Kinamba Rumuruti, China International, Mugie Farm, Notice is hereby given under rule 27 of the Electric Power Rules Maundu Meri, Churo, Suguta Marmar, Tungamara, Poror, Kisima, Maralal & That the electricity supply will be interrupted as here under: adjacent customers. (It is necessary to interrupt supply periodically in order to facilitate maintenance and upgrade of power lines to the network; to connect new SAMBURU COUNTY customers or to replace power lines during road construction, etc.) AREA: WHOLE OF BARAGOI TOWN DATE: Tuesday 03.03.2020 TIME: 9.00 A.M. – 3.00 P.M. NAIROBI WEST REGION Whole of Baragoi, KDF Barracks, Baragoi Boys, Baragoi Hosp, Bendera Pri Sch & adjacent customers. NAIROBI COUNTY AREA: UPPERHILL NORTH RIFT REGION DATE: Saturday 29.02.2020 TIME: 9.00 A.M. - 5.00 P.M. British High Commission, Bibilia Husema Radio Stn, Part of Upperhill Rd & UASIN GISHU COUNTY adjacent customers. AREA: BARSOMBE, KOKWET DATE: Thursday 05.03.2020 TIME: 9.00 A.M. – 5.00 P.M. AREA: PART OF UPPERHILL Barsombe, Kokwet, Kapsigilai, Kiborom, Kaptiony, Chepterit, Lamaon, Lower DATE: Sunday 01.03.2020 TIME: 9.00 A.M. - 5.00 P.M. Moiben, Cheukta, Chebororwa, Koitugum, Ngeny & adjacent customers. Ragati Rd, Ragati Lane, DPP’s Office, Re Towers, Rahimtulla Building, Mwalimu Towers, Japanese Embassy, Mara Rd, Coca Cola, Kilimanjaro Rd, AREA: MAILI NNE, HURUMA TSC, Longonot Rd, Victoria Tower, Crowne Plaza, Part of Elgon Rd, Geo DATE: Thursday 05.03.2020 TIME: 9.00 A.M.