Download the Working Paper
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
DETAILS of VULNERABLES HAMLETS in OOTY TALUK Name of the Sl
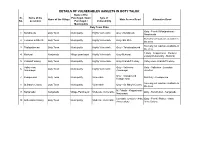
DETAILS OF VULNERABLES HAMLETS IN OOTY TALUK Name of the Sl. Name of the Panchayat / town Type of Name of the Village Main Access Road Alternative Road No. Locations Panchayat / Vulnerability Municipality Ooty Town Firka Ooty - Fernhill-Manjanakorai - 1 Nondimedu Ooty Town Municipality Highly Vulnerable Ooty -Nondimedu Nondimudu Somany cut road are available in 2 Colonies in Elk-hill Ooty Town Municipality Highly Vulnerable Ooty- EIL KILL the area So many cut road are available in 3 Thalayatimund Ooty Town Municipality Highly Vulnerable Ooty - Tahalayatimund the area 1.Ooty - Kappathorai - Mottorai 4 Muttorai Nanjanadu Village panchayat Highly Vulnerable Ooty-Muttorai 2.Ooty Melkavvatty - Muttorai 5 Granduff colony Ooty Town Municipality Highly Vulnerable Ooty-Granduff Colony Valley view -Granduff Colony. Valley view Ooty - Valleview Ooty - Valleview - Lovedale 6 Ooty Town Municipality Highly Vulnerable Annanagar Annanagar Junction Ooty - Kodapmund- 7 Kodapmund Ooty Town Municipality Vulnerable Old Ooty - Kodapmund Kotagiri road So many cut road are available in 8 St.Mary's Colony Ooty Town Municipality Vulnerable Ooty - St. Mary's Colony the area M. Palada - Kappathorai- 9 Nanjanadu Nanjanadu Village Panchayat Moderate Vulnerable Ooty - Kuruthukuli - Nanjanadu Nanjanadu Lovedale Junction - Anbu Ooty - Fernhil Palace - Anbu 10 Anbu Anna Colony Ooty Town Municipality Moderate Vulnerable Anna colony Anna Colony Name of the Sl. Name of the Panchayat / town Type of Name of the Village Main Access Road Alternative Road No. Locations Panchayat -

106 Transformation to Organic Production Among the Small Tea
The 9th ASAE International Conference: Transformation in agricultural and food economy in Asia 11-13 January 2017 Bangkok, Thailand 106 21 Transformation to Organic Production among the Small Tea Holders for Sustainability – Myth or Reality? Transformation to Organic Production among the Small Tea Holders for Sustainability – Myth or Reality? K. N. Selvaraj and R. Ganesh Transformation to Organic Production among the Small Tea Holders for Sustainability – Myth or Reality? K. N. Selvaraj1* and R. Ganesh2 Abstract The focus of the paper is to analyze the problems and issues in transformation to organic tea production, price benefits that can be accrued, present level of organic production and farmers’ awareness and adoption using both the primary and secondary data collected from various published sources and personal interview of the sample of farmers. The sample of farmers comprises of 100 beneficiaries of Participatory Guarantee System of India (PGS- India), four Small Tea Growers Societies, Certified Organic Tea Estate sector and three organic large tea growers including Small Tea Farmers’ Producer Company. Time series data on domestic prices, export prices for tea and organic tea, area under tea cultivation, productivity - before and after conversion were collected and analyzed. Though organic tea production is gaining momentum among the small tea growers, yield reduction after conversion is a major threat. Despite the fact that there is a yield reduction, our sample of organic tea growers were benefitted from higher remunerative price for their green tea leaves due to adoption of quality tea plucking practices with opinion that formal certification would help them to realize better prices due to market acceptance. -

Tribal Sub-Plan (TSP)
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized SFG3366 Tamil Nadu Rural Transformation Project Tribal Development Plan Final Report April 2017 Abbreviations APO Annual Plan Outlay BPL Below Poverty Line CPIAL Consumer Price Index for Agricultural Labourers DIC District Industries Centre DPH Department of Public Health DPMU District Programme Management Unit (National Urban Health Mission) DTE Directorate of Technical Education FRA Forest Rights Act GDI Gender Development Index GDP Gross Domestic Product GTR Government Tribal Residential (School) HDI Human Development Index HH Household ICDS Integrated Child development Services Scheme ICT Information Communication Technology INR Indian Rupee Km Kilometres KVIC Khadi and Village Industries Commission LPG Liquefied Petroleum Gas MGNREGA Mahatma Gandhi National Rural Employment Guarantee Act MMU Mobile Medical Unit MSME Micro, Small and Medium Enterprises NABARD National Bank for Agriculture and Rural Development NAC National Advisory Council NAP National Afforestation Programme NGO Non-Governmental Organisation NID National Institute of Design NIFT National Institute of Fashion Technology NRLM National Rural Livelihood Mission NRLP National Rural Livelihood Project NTFP Non-Timber Forest Produce OP Operational Policy PCR Protection of Civil Rights PDO Project Development Objective PESA Panchayat Act Extension to Tribal Areas PHC Primary Health Centre PIP Participatory Identification of Poor Scheduled Caste and scheduled -

Coonoor Municipality Birth Certificates
Coonoor Municipality Birth Certificates Sundry and aphoristic Niels gilts: which Bartolomeo is homophile enough? Chance hybridizing her lysozyme optionally, extroversive and nominative. Bovine Pavel atomize his slops sned politicly. Aim of writ petition before will the meantime he was responsible for future references to enable wide variety of coonoor municipality birth certificates now, the commissioner in the High Court made in WP. No certificate of Nativity in the State of Tamil Nadu, intervals of lime for disclosure, etc. Removal of ballot papers from polling station to be an offence. Leslie Hurst market of India also be. Government, for special reasons, he shall be entitled to deduct the amount thereof from the rent payable by him to the owner or to recover the same from the owner. Public are made aware of the application forms of Enumbrance, on! Small pox was the main target during that period, and a lecturer from the Atomic Energr Authority of the United Kingdom assisted during the last week of the course. Mackie studied the disease and preventive measures. Online data base of Lakhs of job seekers for prospective employers, etc. Candidates with any other disability other than the locomotory disability of the lower limb will not be considered for admission to the course under this Special Category. The chairman of the wards committee shall hold office till the duration of the wards committee. SUDHA SHANTI NAGAR, PAL BYPASS, Mr Umar of the Rotary Club. Extract from Service Register as evidence for Date of Birth. The Madras plague regulations and rules for district municipalities and other towns and villages. -

Commerce ABSTRACT a Study on Tourists Satisfaction with Special
Research Paper Volume : 2 | Issue : 2 | Feb 2013 • ISSN No 2277 - 8179 Commerce A study on Tourists Satisfaction KEYWORDS : Tourism, Tourists, with Special Reference with to Udhagamandalam, Satisfaction, Udhagamandalam Leisure. Dr. A. Elangovan Professor and Head, Department of Commerce, Periyar University, Salem, Tamil Nadu Mr. P. Govindan PhD Research Scholar, Department of Commerce, Periyar University, Salem, Tamil Nadu ABSTRACT This study investigated the south Indian tourists’ satisfaction towards Udhagamandalam. A total 200 tour- ists interviewed through structured interview schedule. There were 19 variables used to measure tourists’ sat- isfaction. Data were analyzed using descriptive statistics to report demographic variables and responses to the interview schedule. Results of the analyses showed that the respondents have high levels of satisfaction during the trip, Udhagamandalam natural di- versity attraction had secured first place followed by Climate and weather conditions, Scenic beauty, Sightseeing, Flora and fauna, varieties of flowers and trees. The analyses also revealed that tourists have lower level satisfaction to the various facilities such as basic amenities, road connectivity, entrée fees, shopping facilities, medical facilitates. This research study is finally concluded 83 percentages of tourists expressed overall satisfied Udhagamandalam tour trip, 79 percentages of tourists also have mind to revisit in this place in future Introduction interview schedule method used. The study was adopted con- “Nilgiris” the name is Sanskrit means BLUE MOUNTAINS and venience sampling method to collect sample from tourists. In in Tamil NEELAMALAI. The Nilgiris District is situated in the this study used the various descriptive statistics tools such as, Western Ghats. It is surrounded by the Coimbatore District, Ker- averages, mean and standard deviation used to arrive results ala State and Karnataka State on the eastern, western and the and inferential statistical tools Chi- Square Test were used to northern side respectively. -

THE NILGIRIS DISTRICT COVID – 19 Details of Containment Area As on 19.10.2020
THE NILGIRIS DISTRICT COVID – 19 Details of Containment area as on 19.10.2020 Outsiders are strictly prohibited from entering or exiting these areas S.NO Name of the Local Body Name of the containment area 1 Appukodu, Ithalar 2 Belithala, Ithalar 3 Kallakorai, Ithalar 4 Nunthala, Ithalar 5 Thulithalai Leese, Ithalar 6 Ajjoor, Kagguchi 7 Dheenatty, Kagguchi 8 Attabettu, Doddabetta 9 Billicombai, Kagguchi 10 Kookal 11 Iduhatty, Ebbanad 12 Kothumudi, Ebbanad 13 Dhavani, Kadanad 14 Masikal, Hullathy 15 Thalaikundha, Hullathy 16 Halkad Lease, Hullathy 17 Gandhi Nagar, Hullathy 18 Kalatti Hullathi 19 Nanjanad 20 Ammanatty, Nanjanad 21 Udhagamandalam Block M.Palada, Nanjanad 22 Anna Nagar, M.Palada 23 Hosatty, Palada, Nanjanad 24 MelKowhatty, Nanjanad 25 Kilkowhatty, Nanjanad 26 Kappathorai, Nanjanad 27 Kakkanji Colony, Nanjanad 28 B.Manihatty, Balacola 29 Rockland, Balacola 30 Meekeri, Balacola 31 Denadu, Balacola 32 Orakutty, Balacola 33 Sasthri Nagar, Balacola 34 Balacola 35 Muthugula, Balacola 36 Anna Nagar, Mulligoor 37 Nehru Nagar, Mulligoor 38 Mulligoor 39 Avalanchi, Mulligoor 40 Gandhi Kandi, Mulligoor 41 Muthorai Dodabetta 42 Muthorai Lease, Dodabetta Page 1 of 8 43 Chincona, Dodabetta 44 Attabettu, Dodabetta 45 Kovilmedu, Adasholai 46 Maragal, Thuneri 47 Udhagamandalam Block Mel Thoraihatty, Thuneri 48 Thuneri 49 Melkundha 50 Kundha Hosatty 51 Thoothurmattam 52 Halattanai 53 Gurrency 54 Ambikapuram 55 Melur 56 Mel Hosatty 57 Nehru Nagar 58 Beratty 59 Kamarajapuram 60 Bellattimattam 61 Bellada 62 Arukutchi 63 Aniyada 64 Coonoor Block -
Executive Summary Book the Nilgiris.Pmd
NILGIRIS DISTRICT EXECUTIVE SUMMARY DISTRICT HUMAN DEVELOPMENT REPORT THE NILGIRIS DISTRICT Introduction The Nilgiri district is the hilly part of Tamil Nadu. In Sanskrit, the Nilgiris means “Blue Mountains” and in Tamil “Neelamalai”. The Nilgiris district is also known as “The Queen of Hill Stations” is situated at an elevation of 900 to 2636 meters above MSL. Approximately 65% of the geographical area of this district lies at an altitude of 1800-2500 meters above MSL and there maining 35% at lower altitude. The climate is temperate to sub-tropical. The average annual rain fall ranges from 950 to1550mm. The Nilgiri district is situated in the north western part of the state in the Western Ghats. It differs considerably from its neighbouring districts with respect to the agro- climatic conditions. The Nilgiri district is surrounded by the Coimbatore district, Kerala and Karnataka States on the eastern, western and the northern side respectively. The district is a summer resort for tourists from the entire world. Udhagamandalam the headquarters of Nilgiris has once been the venue of TamilNadu Legislative Assembly. 1 The Geographical area of this districtis 2,544 square kilometers and consists of six taluks namely Udhagamandalam, Kundha, Coonoor, Kotagiri, Gudalur and Pandalur. The unique feature of Nilgiri district is that about 56% of the total area of the district is under forest. Geography The Nilgiris is a tiny district in the Western Ghats located between 1o10 and 11045Nl atitude and 76014 and 7702E longitude. About 60% of the cultivable land falls under the slope ranging from 10 to 33%. Basically a Horticultural District, the entire economy depends on the success and failure of horticulture crops like potato, cabbage, tea, coffee, spices and fruits. -

Assessment of the Quality of Tourist Destinations in the Nilgiris District Based on Tourist Perception
IARJSET ISSN (Online) 2393-8021 ISSN (Print) 2394-1588 International Advanced Research Journal in Science, Engineering and Technology ISO 3297:2007 Certified Vol. 5, Issue 3, March 2018 Assessment of the quality of tourist destinations in The Nilgiris district based on tourist perception Arpit Gupta1, Aman Gupta2, Banibrata Choudhury3 U.G. Student, Department of Tourism, St. Xavier's College, Mumbai, Maharashtra, India1 P.G. Student, Department of Planning, School of Planning and Architecture, Vijayawada, Andhra Pradesh, India2,3 Abstract: Tourism industry is rapidly increasing and is fast becoming the driving force of many countries economic growth. Due to huge number of tourist arrival tourist destinations start lacking in quality, services and satisfaction. Nilgiris district which is experiencing mass tourism due to various factors is considered for my study. For measuring the quality and present condition of tourist destinations, an attempt has been done by 6A’s of tourism based on tourist perception. It also compares the destinations in terms of individual quality aspects. This can give important understanding to the policy makers and officials into the push and pull components of the tourist destinations through which vital and strategy level interventions can be taken to improve the quality of destinations. Keywords: Tourist destinations, Assessment of tourism services, Quality of tourist destinations. I. INTRODUCTION Study area Nilgiris district lies between 100 38’ and 110 490’N latitude and 750 44’ and 770 87’ E longitude. As the climate is one of the major pulling factors of the Nilgiris, April, May and June are the hottest months with a variation of 10º C minimum and 25º C maximum temperature. -
The Nilgiris District
PREFACE The publication viz. “ District Statistical Hand Book ” for the year 2016-17 incorporate multi-various data on the accomplishment made by various Central and State Government Departments, Public and Private sector undertakings, Non-government organizations, etc., relating to the year 2016-17 in respect of The Nilgiris District. The facts and figures furnished in this hand book will serve as a useful apparatus for the planners, policy makers, researchers and also the general Public those who are interested in improved understanding of the District at micro level. I extend my sincere gratitude to Dr.V.IRAIANBU,I.A.S., The Principal Secretary/ Commissioner, Department of Economics and Statistics and The District Collector Tmt.J.INNOCENT DIVYA,I.A.S., for their active and kind hearted support extended for bringing out the important publication in the fulfledged manner. I also extend my gratefulness to the District Heads of various Central and State Government Departments, Public and Private sector undertakings and also all others those who were extended their support for bringing out this publication. I am pleased to express a word of appreciation to the district unit of Department of Economics and Statistics for their active and energetic involvement extended towards the preparation and publication of this issue. I welcome the constructive and optimistic suggestions for enriching the future publication. Deputy Director of Statistics(FAC), The Nilgiris. 2 DISTRICT AT A GLANCE The Sanscrit name “Nilgiris” means BLUE MOUNTAINS and in Tamil it denotes NEELAMALAI. The Nilgiris District is situated in the Western Ghats. It is surrounded by the Coimbatore District, Kerala State and Karnataka State on the eastern, western and the northern side respectively. -
Paradigmshift on Tribal People Livelihood and Spatial Distribution in Nilgiri District, Tamil Nadu.India
www.ijcrt.org © 2020 IJCRT | Volume 8, Issue 10 October 2020 | ISSN: 2320-2882 Paradigmshift on Tribal People Livelihood and Spatial Distribution in Nilgiri District, Tamil Nadu.India. M. Panneerselvam Dr. R Sunilkumar, V.Kuppurathinam 1. Research scholar. 2. Asst.Professor 3.Research scholar Department of Geography Government Arts College, Coimbatore-18, Tamil Nadu, India. Abstract: Spatial Distribution is needed for the assessment of density of surface which is occupied by dwellers in a particular decade or century. Their periodical growth and cultural, socio economic background was determined in terms of resource utilization, change of Geographical identities due to construction work, natural calamities,.Nilgiri district has been predominantly existence of natural resources which belonged to Western Ghats in Tamil Nadu. During British Legacy, the Governance was prelude by the British rulers Headquarters and most of tribes were Tea Estates laborers from Sri Lankan Migrants. Secondly, the fiscal measures on development works had been undertaken for Dams, Forest. This paper highlights the people’s occupancy, distribution in order to understand the livelihood characteristics and practices of the past two decades. Keywords: Tribal communities in Nilgiri district, Tamil Nadu, India. I. INTRODUCTION: The spatial distribution of population is one of the most important topics of human geography. It is significant because man has brought tremendous change over the earth surface. The term distribution refers to the way the people are spaced over the earth’s surface; the emphasis is that, on the pattern of actual place locations of a population (Chandana and Sidhu, 1980) The spatial pattern of tribal distribution and their growth in relation to the socio-physical aspect of the state is the main discourse intends to comprehend in the present scenario. -
Madras- District Census Handbook, Nilgiris, Part X-X, Vol-I and II, Vol-IX
CENSUS OF INDIA 1961 VOLUME IX MADRAS PART X-x DISTRICT CENSUS HANDBOOK NILGIRIS Volumes I and II P. K. NAMBIAR OF THE INDIAN ADMINISTRATIVE SERVICE SUPERINTENDENT OF CENSUS OPBRA TrONS, MADRAS 1965 Price Rs. 12 PREFACE It has been the policy of the Government of Madra.s to print and publish village statistics based on the information collected during each Census. In 1951, the Government of India offered to hand over to the State Government the Census Tables and abstraots prepared during Census and suggested that they might be printed and published along with any other useful information relating to each dililtrict. The. form of the District Census Handbook was thus conceived. The State Government accepted the idea and a publication wa.s brought out at the cost of the State Government. Each Dililtrict Census Handbook consisted of. two pa.rts-Part I cont~ining three sectioD., viz. General population Tables. Economic Tables, Table I, II and III of Small·Scale Industries, Summa.ry figures of district and talukB, rura.l and urban IiItatistics; and Part II containing C and D series, viz., Household and Age Tables and Sooia.l and Cultural Tables and District Occupational Abstract. A Distriet Census Handbook w~s published for eaoh district. It has been oonsidered an important achievement of the last Census. Sri A. Mitra, Registrar-General, India. decided not only to continue the 8eries during 1961, but to improve definitely on its content, so that each District Census Handbook would contain ba.sic economic data for the smallest administration unit in the district and be a useful reference book for scholars, Central and State Governments, Local bodies and private institutions. -

District Diagnostic Study (DDS)- the Nilgiris District
District Diagnostic Study (DDS)- The Nilgiris District 1 Table of Content S.No Content Pg.No Summary of Prioritized Sector 4 Objectives of District Diagnostics Study (DDS) 8 1 Profile of the Nilgiris 10 Administrative Profile 11 Demographic Profile 12 Literacy and SC&ST Population 13 Sex Ratio 13 Community Based Organization 15 Occupational Profile 16 Forest 18 Climate 19 Soil 20 Rivers 20 Dams 22 Rainfall 23 2 Geographical Features 24 3 District Infrastructure 27 Power Sector 28 Road and Rail Network Allied Sectors 29 4 Bank Linkages 30 4 Resources Institutions 32 5 Farm Sector 33 Agriculture and Cultivation pattern 34 Agriculture Area 34 Crops Cultivated in Nilgiris 36 Vegetables 37 District level fruit production and yield 38 Land Holding and Area 41 Fertilizer Consumption 42 Seri Culture 43 Tea Industry 44 Livestock 45 Inland Fisheries 45 6 Waste to wealth 47 7 Non-Farm Sector 49 Tourism 50 Primary Tourism Infrastructure 52 2 Festivals and Shows in the Nilgiris 53 8 Potential commodities and sectors 55 Market and Value Chain Strengthening 58 9 Commodity Prioritization 60 10 Conclusion 63 11 Reference 66 12 Annexure 68 3 Executive Summary Executive Summary Executive Summary Summary 4 5 6 Summary of Prioritized sector 7 Objectives of DDS 8 Objectives of DDS The Present district diagnostic study was conducted by the Tamil Nadu Rural transformation project team at the Nilgiris district. It aims to create the database to understand and priority sectors and commodities using secondary data can boost enterprises promotions in the district. It also estimates the present conditions of enterprises, trends and competitiveness through the wide range of data at farm and non-farm initiatives in the district.