District Profile: Sukkur
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
PESA-DP-Sukkur-Sindh.Pdf
Landsowne Bridge, Sukkur “Disaster risk reduction has been a part of USAID’s work for decades. ……..we strive to do so in ways that better assess the threat of hazards, reduce losses, and ultimately protect and save more people during the next disaster.” Kasey Channell, Acting Director of the Disaster Response and Mitigation Division of USAID’s Office of U.S. Foreign Disas ter Ass istance (OFDA) PAKISTAN EMERGENCY SITUATIONAL ANALYSIS District Sukkur September 2014 “Disasters can be seen as often as predictable events, requiring forward planning which is integrated in to broader development programs.” Helen Clark, UNDP Administrator, Bureau of Crisis Preven on and Recovery. Annual Report 2011 Disclaimer iMMAP Pakistan is pleased to publish this district profile. The purpose of this profile is to promote public awareness, welfare, and safety while providing community and other related stakeholders, access to vital information for enhancing their disaster mitigation and response efforts. While iMMAP team has tried its best to provide proper source of information and ensure consistency in analyses within the given time limits; iMMAP shall not be held responsible for any inaccuracies that may be encountered. In any situation where the Official Public Records differs from the information provided in this district profile, the Official Public Records should take as precedence. iMMAP disclaims any responsibility and makes no representations or warranties as to the quality, accuracy, content, or completeness of any information contained in this report. Final assessment of accuracy and reliability of information is the responsibility of the user. iMMAP shall not be liable for damages of any nature whatsoever resulting from the use or misuse of information contained in this report. -

Government of Sindh Road Resources Management (RRM) Froject Project No
FINAL REPORT Mid-Term Evaluation /' " / " kku / Kondioro k I;sDDHH1 (Koo1,, * Nowbshoh On$ Hyderobcd Bulei Pt.ochi 7 godin Government of Sindh Road Resources Management (RRM) Froject Project No. 391-0480 Prepared for the United States Agency for International Development Islamabad, Pakistan IOC PDC-0249-1-00-0019-00 * Delivery Order No. 23 prepared by DE LEUWx CATHER INTERNATIONAL LIMITED May 26, 1993 Table of Contents Section Pafle Title Page i Table of Contents ii List of Tables and Figures iv List of Abbieviations, Acronyms vi Basic Project Identification Data Sheet ix AID Evaluation Summary x Chapter 1 - Introduction 1-1 Chapter 2 - Background 2-1 Chapter 3 - Road Maintenance 3-1 Chapter 4 - Road Rehabilitation 4-1 Chapter 5 - Training Programs 5-1 Chapter 6 - District Revenue Sources 6-1 Appendices: - A. Work Plan for Mid-term Evaluation A-1 - B. Principal Officers Interviewed B-1 - C. Bibliography of Documents C-1 - D. Comparison of Resources and Outputs for Maintenance of District Roads in Sindh D-1 - E. Paved Road System Inventories: 6/89 & 4/93 E-1 - F. Cost Benefit Evaluations - Districts F-1 - ii Appendices (cont'd.): - G. "RRM" Road Rehabilitation Projects in SINDH PROVINCE: F.Y.'s 1989-90; 1991-92; 1992-93 G-1 - H. Proposed Training Schedule for Initial Phase of CCSC Contract (1989 - 1991) H-1 - 1. Maintenance Manual for District Roads in Sindh - (Revised) August 1992 I-1 - J. Model Maintenance Contract for District Roads in Sindh - August 1992 J-1 - K. Sindh Local Government and Rural Development Academy (SLGRDA) - Tandojam K-1 - L. -

Government of Sindh Finance Department
2021-22 Finance Department Government of Sindh 1 SC12102(102) GOVERNOR'S SECRETARIAT/ HOUSE Rs Charged: ______________ Voted: 51,652,000 ______________ Total: 51,652,000 ______________ ____________________________________________________________________________________________ GOVERNOR'S SECRETARIAT ____________________________________________________________________________________________ BUILDINGS ____________________________________________________________________________________________ P./ADP DDO Functional-Cum-Object Classification & Budget NO. NO. Particular Of Scheme Estimates 2021 - 2022 ____________________________________________________________________________________________ Rs 01 GENERAL PUBLIC SERVICE 011 EXECUTIVE & LEGISLATIVE ORGANS, FINANCAL 0111 EXECUTIVE AND LEGISLATIVE ORGANS 011103 PROVINCIAL EXECUTIVE KQ5003 SECRETARY (GOVERNOR'S SECRETARIAT/ HOUSE) ADP No : 0733 KQ21221562 Constt. of Multi-storeyed Flats Phase-II at Sindh Governor's 51,652,000 House, Karachi (48 Nos.) including MT-s A12470 Others 51,652,000 _____________________________________________________________________________ Total Sub Sector BUILDINGS 51,652,000 _____________________________________________________________________________ TOTAL SECTOR GOVERNOR'S SECRETARIAT 51,652,000 _____________________________________________________________________________ 2 SC12104(104) SERVICES GENERAL ADMIN & COORDINATION Rs Charged: ______________ Voted: 1,432,976,000 ______________ Total: 1,432,976,000 ______________ _____________________________________________________________________________ -

Educación, Política Y Valores
1 Revista Dilemas Contemporáneos: Educación, Política y Valores. Http://www.dilemascontemporaneoseducacionpoliticayvalores.com/ Año: VII Número: 2 Artículo no.:119 Período: 1ro de enero al 30 de abril del 2020. TÍTULO: Un análisis empírico de la cerámica esmaltada del sitio de Mansurah. AUTORES: 1. Assist. Prof. Muhammad Hanif Laghari. 2. Dr. Mastoor Fatima Bukhari. RESUMEN: Mansurah fue la primera ciudad árabe establecida en el subcontinente indio entre 712–1025 dC por el gobernador omeya Amr Thaqafi Construido en el Shahdadpur del distrito de Sanghar, Sindh. Durante este período, los gobernantes árabes extendieron el comercio nacional e internacional desde Sindh. La espectroscopia fue utilizada para examinar el material de cultivo excavado y para encontrar el origen de la cerámica esmaltada. Las evidencias empíricas extraídas del material cultural resaltan la composición de la pasta de color utilizada en estos vasos rotos y se preparan utilizando la arena de dos tipos diferentes de rocas como la volcánica y la metamórfica. Este estudio resalta las relaciones árabe-sindh y otros aspectos culturales de esta fase específica de la historia de Sindh, Pakistán. PALABRAS CLAVES: Arqueología, Historia, Geografía, cerámica esmaltada, relación y comercio. TITLE: An empirical analysis of glazed pottery from the site of Mansurah. 2 AUTHORS: 1. Assist. Prof. Muhammad Hanif Laghari. 2. Dr. Mastoor Fatima Bukhari. ABSTRACT: Mansurah was the first Arab city established in the Indian sub-continent between 712–1025 AD by the Umayyad governor ‘Amr Thaqafi Built in the Shahdadpur of District Sanghar, Sindh. During this period, the Arab rulers extended national and international trade from Sindh. The spectroscopy was used to examine the excavated culture material and to find the origin of the glazed pottery. -

Sukkur Barrage Rehabilitation and Modernization Public Disclosure Authorized
Government of Sindh, Pakistan Public Disclosure Authorized Sindh Barrages Improvement Project - Sukkur Barrage Rehabilitation and Modernization Public Disclosure Authorized ENVIRONMENTAL AND SOCIAL ASSESSMENT Public Disclosure Authorized EXECUTIVE SUMMARY Sindh Irrigation Department Public Disclosure Authorized December 2017 Contents List of Acronyms .............................................................................................................. iii 1. Introduction ................................................................................................................. 1 1.1. Background .......................................................................................................... 1 1.2. Sindh Barrages Improvement Project (SBIP)........................................................ 2 1.3. The Environmental and Social Assessment.......................................................... 3 2. Policy, Legal and Administrative Framework ........................................................... 5 2.1. Applicable Legislation and Policies in Sindh, Pakistan ......................................... 5 2.2. Environmental Procedures ................................................................................... 6 2.3. World Bank Safeguard Policies ............................................................................ 6 3. Project Description ................................................................................................... 10 3.1. Description of Sukkur Barrage ........................................................................... -

Spatio-Temporal Flood Analysis Along the Indus River, Sindh, Punjab, KPK and Balochistan Provinces, Pakistan Version 1.0
21 August 2010 FL-2010-000141-PAK Spatio-Temporal Flood Analysis along the Indus River, Sindh, Punjab, KPK and Balochistan Provinces, Pakistan Version 1.0 This map shows daily variation in flood water extent along the Indus rivers in Sindh, Punjab, Balochistan and KPK Index map CHINA Crisis Satellite data : MODIS Terra / Aqua Map Scale for 1:1,000,000 Map prepared by: Supported by: provinces based on time-series MODIS Terra and Aqua datasets from August 17 to August 21, 2010. Resolution : 250m Legend AFGHANISTAN Image date : August 17-21, 2010 025 50 100 Result show that the flood extent is continously increasing during the last 5 days as observed in Shahdad Kot Tehsil Source : NASA of Sindh and Balochistan provinces covering villages of Shahdad, Jamali, Rahoja, Silra. In the Punjab provinces flood has Pre-Flood River Line (2009) ® Kilometres Pre-flood Image : MODIS Terra / Aqua q Airport Map layout designed for A1 Printing (36 x 24 inch) partially increased further in Shujabad Tehsil villages of Bajuwala Tibba, Faizpur, Isanwali, Mulana)as. Over 1000 villages Resolution : 250m Flood Water extent (Aug 17) and 100 towns were identified as severly affected by flood waters and analysis was performed using geospatial database v® Heliport Image date : September 19, 2009 Flood Water extent (Aug 18) received from University of Georgia, google earth and GIS data of NIMA (USGS). Approx. 800 kilometres stretch of Source : NASA p ! Villages/towns PAKISTAN national highway and link roads are submerged or partially inundated by flood water. Flood Water extent (Aug 19) Major airfield Railways IRAN INDIA Baseline Imagery : MODIS Aqua Aug 19, 2010 Ri vers ± Source : NASA Flood Water extent (Aug 20) p Minor airport Rural road Urbanized area This analysis also used Pre river line MODIS data for September 19, 2009 to show identify flood water only. -

Sindh Community Mobilization Program
SINDH COMMUNITY MOBILIZATION PROGRAM Quarterly Progress Report – Year IV, Quarter II (January 1, 2017 – March 31, 2017) Date: April 30, 2017 CMP is made possible by the support of the American People through the U.S. Agency for International Development (USAID). CMP is implemented by International Relief and Development (IRD) under Contract Award No: AID-391-C-13-00006. This report was produced for review by USAID. CMP Year IV, Quarter II Report 1 Table of Contents Table of Contents ................................................................................................................................................ 2 ACRONYMS ........................................................................................................................................................ 3 1. PROGRAM SUMMARY ........................................................................................................................... 6 2. SUMMARY OF ACCOMPLISHMENTS DURNG REPORTING PERIOD....................................... 7 3. STATUS OF THE ACTIVITIES AS PER THE COMPONENTS ......................................................... 9 3.1. Component I: Increase Community Involvement in the GOS Reforms of Merging, Consolidating, and Upgrading Schools ......................................................................................................... 9 3.2. Component II: Improve Community and District Government Coordination for Increased Girls’ Enrollment .......................................................................................................................................... -

Airlift Target Locations, Sindh Province
! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !( ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! (! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! (! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! (! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! !( ! (! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Goth Goth 67°20'E 67°30'E 67°40'E 67°50'E 68°0'E 68°10'E Allahdad 68°20'E Gauhar Goth Firoz Haidarpur 68°30'E 68°40'E ! ! ! ! Khan Khan Wagha ! Goth Nasir Goth Goth Goth Rasul Khan Dasti Dheran Kalati Bakhsh Goth Attar Faqir Khan Wagha Bhangar Goth Abdul 28°20'N ! ! ! ! ! 28°20'N ! ! Goth Ghafur Goth Dur Muhammad Muhammad Goth Goth Husain Goth Nur Goth Dur Jamali Sohnipur Sohbdar Yar Ali Mamal Muhammad Muhammad ! ! ! ! ! ! ! ! ! Bahadarpur ! Bahadarpur ! ! ! Goth Faizabad Chachar Goth Ali Goth ! Goth Data Goth Gulab Bakhsh Sahibdina Tajpur Dang Wah Khan Domki Machhi Khosa Somra Zangipur ! ! Dera ! ! ! ! ! ! ! Dilawarpur Goth Umar Goth Goth Alan Khan Babar Sher Khan Dasti Murad Jamali Tehsil Jhat Pat Tehsil Wasand Goth Khuda Muhammad Jatol Dil Jhal Kator Lohra Bakhsh Murad Odhano ! ! ! ! ! ! ! ! Balach Jacobabad Nasirabad District !(H Goth Rojhan Goth Gul Goth Haji Goth Hasil (! Jan Miral Thul Naubatpur Sathi Kohna Muhammad Khan Domki Khan Domki Muhammad Nau (!H! ! ! ! ! ! ! (!H ! ! ! Gandawa Goth Goth (!H Shah Beg Jani Daman Mundrani Dero Shah Bhambul Tehsil ! ! ! ! ! ! Khanpur -

Ongar: a Source of Chert in Lower Sindh (Pakistan) and Its Bronze Age Exploitation
Ongar: a Source of Chert in Lower Sindh (Pakistan) and Its Bronze Age Exploitation Paolo Biagi Department of Asian and North African Studies, Ca’ Foscari University, Venice, Ca’ Cappello, San Polo 2035, I - 30125 Venezia, Italy e-mail: [email protected] Elisabetta Starnini School of Humanistic Sciences, Department of Historical Studies, University of Torino, via S. Ottavio 20, I - 10124 Torino, Italy e-mail: [email protected] Abstract: This paper summarizes the results of twenty-six years of fieldwork carried out by the Italian Archaeological Expedi- tion in Sindh in search for chert sources, and documenting their exploitation in prehistory at least since the Acheulian Palaeo- lithic to the Bronze Age, Indus Civilization mining areas and workshops. The explorations focused on three main chert sources: the Rohri Hills, Ongar, Daphro and Bekhain Hills, and Jhimpir. They are not the only ones known to date in Sindh that were in- tensively exploited especially during the development of the Indus Civilization. The economic importance of chert exploitation in the Indus Civilization has often been underestimated by most archaeologists. This fact is evident when reading the published narratives about its handicraft, trade and production, although there is little doubt that this raw material played a fundamental role in the economy of the Indus cities, also as main alternative to metal for making well-defined tools for specific handicrafts. The importance of chert exploitation is testified indeed by the impressive archaeological evidence left behind. It consists of chert mines, chipping floors and blade/bladelet workshops, whose preservation is unfortunately challenged by present-day in- dustrial works still underway. -

Analysis on Flood Affected Areas Along the Indus River, Parts Of
! ! ! ! ! ! ! ! 24 August 2010 ! ! ! ! FL-2010-000141-PAK A n a l y s i s o n F l o o d A f f e c t e d A r e a s a l o n g t h e I n d u s R i v e r, P a r t s o f S i n d h P r o v i n c e , P a k i s t a n Version 1.0 ! ! ! ! ! Map Scale 1: 180,000 Index map CHINA ! Map prepared by: Supported! by: ! ! Crisis Satellite data : AVINIR - ALOS Legend 0 5 10 20 AFGHANISTAN ! ! This map presents a preliminary analysis of flood affected areas covering part of Sindh province, Pakistan and is baq®sed Resolution : 10m q® ! ! on AVINIR-ALOS satellite imagerys covering the period of August 23, 2010. ! Image date : August 23, 2010 Flood Inundated Kilometers ! Source : JAXA Map layout designed for A1 Printing 36 x 24 inch) Till August 23, 2010 approx. 3492.08 sq.km are severly affected by flood waters. Over 184 villages and several square Cropland ! GIS Data : Universiyt of Georgia, USA ! ! kilometers of cart road and main roads are partia!lly submerged or severly inundated by flood waters.This analysis was q® Airport Settlements performed using geospatial database received from University of Georgia, google earth for counting villages/towns. Flood Analysis : ICIMOD Settlement PAKISTAN Projection : UTM, 42N, GRS1980 Rivers Railways IRAN INDIA ! This analysis also used Pre-flood river line data from NIMA/USGS to show the extent of flood !water only. -

NATIONAL DRAINAGE PROGRAM (NDP) PROJECT Sindh Province 35° 35° N.W.F.P
65° UZBEK. 70° 75° TAJIKISTAN CHINA TAJIK. PAKISTAN TURKMENISTAN NATIONAL DRAINAGE PROGRAM (NDP) PROJECT Sindh Province 35° 35° N.W.F.P. Approx. Line Peshawar of Control AFGHANISTAN CULTURAL SITES MENTIONED IN REQUEST JAMMU SELECTED BASIN BOUNDARIES ISLAMABAD AND KASHMIR DHANDS AND LAGOONS MENTIONED IN REQUEST DESERTS/HILLS WEIRS/BARRAGES MENTIONED IN REQUEST SELECTED TOWNS Lahore CANALS MENTIONED IN REQUEST MAJOR CITIES PUNJAB Quetta DRAINS MENTIONED IN REQUEST TEHSIL HEADQUARTERS 30° 30° NSDS (shown in SAR but no longer proposed under NDP Project) DISTRICT HEADQUARTERS Area of map PROVINCE HEADQUARTERS BALOCHISTAN RIVERS OR STREAMS PROVINCE BOUNDARIES ISLAMIC REP. OF INDIA IRAN CANALS INTERNATIONAL BOUNDARIES DRAINS SINDH 25 BRANCH/DISTRIBUTARY CANALS 25° Karachi ° AREA WATER BOARDS Arabian Sea BARRAGES 65° 70° 75° 67° 68° 69° 70° 71° This map was produced by the Map Design Unit of The World Bank. The boundaries, colors, denominations and any other information shown Kashmor Guddu Barrage on this map do not imply, on the part of The World Bank Group, any PUNJAB judgment on the legal status of any territory, or any endorsement or Murad acceptance of such boundaries. Unihar Kandh Kot Jacobabad Dil N.W. Canal Hazaro Begari Canal Canal Canal Dy. Feeder Ubauro Begari 28° Khirthar Garhi Khaio Choi Branch Feeder 28° Faizabad Dy. Shikarpur Khanpur Sindh Daharki Ghotki Shahdadkot Garhi Yasin Ghotki Mirpur Mathelo Nujpur Dy. Mithri Dy. Shahdadkot Branch Lakhi Pano Aqil Ratodero Sukkur RBOD (Right Bank Outfall Drain) Miro Khan Branch Sukkur Barrage -
Sukkur District
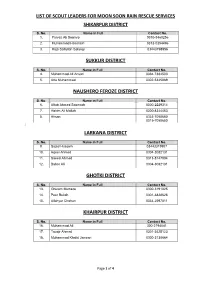
LIST OF SCOUT LEADERS FOR MOON SOON RAIN RESCUE SERVICES SHIKARPUR DISTRICT S. No. Name in Full Contact No. 1. Parvez Ali Soomro 0310-3460256 2. Muhammad Hassnain 0313-0354496 3. Raja Saifullah Solangi 03443798956 SUKKUR DISTRICT S. No. Name in Full Contact No. 4. Muhammad Ali Ansari 0334-7384503 5. Atta Muhammad 0302-5345089 NAUSHERO FEROZE DISTRICT S. No. Name in Full Contact No. 6. Aftab Ahmed Soomrah 0300-2229314 7. Hakim Ali Mallah 0300-8344453 8. Ahsan 0333-7050650 0315-7050650 [ LARKANA DISTRICT S. No. Name in Full Contact No. 9. Sajad Hussain 03443319907 10. Aqeel Ahmed 0304-3082131 11. Saeed Ahmed 0313-8147004 12. Babar Ali 0304-3082131 GHOTKI DISTRICT S. No. Name in Full Contact No. 13. Ghulam Murtaza 0300-3191025 14. Peer Buksh 0301-3828628 15. Allahyar Chohan 0334-2597811 KHAIRPUR DISTRICT S. No. Name in Full Contact No. 16. Muhammad Ali 300-2194041 17. Touqir Ahmed 0301-3425123 18. Muhammad Khalid Janwari 0300-3138664 Page 1 of 4 TANDO ALLAHYAR DISTRICT S. No. Name in Full Contact No. 19. Nooral 0336-3775799 20. Joel 0315-5918990 TANDO MUHAMMAD KHAN S. No. Name in Full Contact No. 21. Shah Nawaz 0333-88859936 22. Muhammad Amir Shaikh 0333-2687290 SHAHEED BENAZIRABAD DISTRICT S. No. Name in Full Contact No. 23. Abdul Razzaq 0300-3235387 0310-3450768 BADIN S. No. Name in Full Contact No. 24. Mir Muhammad Khoso 0301-2000952 25. Muhammad Yousif 0333-2815881 26. Abdul Shakoor 0333-2808034 0301-3614492 JACOBABAD DISTRICT [S. No. Name in Full Contact No. 27. Mukhtar Ahmed 0333-7354748 28.