Dynamic Balance of Ballroom Dancers and Soccer Players
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Las Vegas, Nevada
2021 Toyota U.S. Figure Skating Championships January 11-21, 2021 Las Vegas | The Orleans Arena Media Information and Story Ideas The U.S. Figure Skating Championships, held annually since 1914, is the nation’s most prestigious figure skating event. The competition crowns U.S. champions in ladies, men’s, pairs and ice dance at the senior and junior levels. The 2021 U.S. Championships will serve as the final qualifying event prior to selecting and announcing the U.S. World Figure Skating Team that will represent Team USA at the ISU World Figure Skating Championships in Stockholm. The marquee event was relocated from San Jose, California, to Las Vegas late in the fall due to COVID-19 considerations. San Jose meanwhile was awarded the 2023 Toyota U.S. Championships, marking the fourth time that the city will host the event. Competition and practice for the junior and Championship competitions will be held at The Orleans Arena in Las Vegas. The event will take place in a bubble format with no spectators. Las Vegas, Nevada This is the first time the U.S. Championships will be held in Las Vegas. The entertainment capital of the world most recently hosted 2020 Guaranteed Rate Skate America and 2019 Skate America presented by American Cruise Lines. The Orleans Arena The Orleans Arena is one of the nation’s leading mid-size arenas. It is located at The Orleans Hotel and Casino and is operated by Coast Casinos, a subsidiary of Boyd Gaming Corporation. The arena is the home to the Vegas Rollers of World Team Tennis since 2019, and plays host to concerts, sporting events and NCAA Tournaments. -

Please Welcome Your ISU Skating Awards 2020 Hosts - Tanith and Charlie White
Please welcome your ISU Skating Awards 2020 hosts - Tanith and Charlie White The International Skating Union (ISU) is pleased to announce that Tanith and Charlie White will be the hosts of the inaugural and virtual ISU Skating Awards, which will take place on July 11, 2020 and will be Live Streamed on ISU Skating Awards page from 16:00 CEST. Olympic silver medalist, four-time ISU World Figure Skating medalist, three-time ISU Four Continents Champion and Five-time U.S. Champion with her Ice Dance partner Benjamin Agosto, Tanith is now a respected sports commentator. “We’re so honored to be a part of this brand new show, celebrating the accomplishments of our skating family” Tanith commented “Like all of you, we’ve missed skating these past few months and can’t wait to look back at some of the moments and people who made last season so special.” Charlie is also a former Ice Dancer who skated with Meryl Davis. They were Olympic gold and silver medalists, two-time ISU World Figure Skating Champions, five-time ISU Grand Prix of Figure Skating Champions and three-time ISU Four Continents Figure Skating Champions and six-time U.S. National Champions. “Figure skating at its best offers an opportunity to inspire and unite” said the Olympic Champion “We’re grateful for the chance to show our appreciation for the sport and also remember all that we have to look forward to. “ Tanith and Charlie will host the show from the Detroit Skating Club, an ISU Center of Excellence and the rink where they trained throughout most of their career. -

Carolyn Tonidandel
HERTZ ARENA FIGURE SKATING COACHES Adam Smith Junior Moves, Junior Free skate, Novice Free Dance, Silver Dance, Blues (Pre-Gold). Classically trained in ballet, Off Ice Jumping technique, Russian and American Training. Trained in ice dance by Alexander Zhulin. 2014 - U.S. Adult Figure Skating Championships silver dance gold. Coaching: All levels of Basic Skills, Ice Dance, Moves in the Field, Freestyle, Jumps, Partnering and Stroking. Phone: 239-898-2477 / Email: [email protected] Rate: $35.00 - 30 minutes Diane Myers Has been teaching all phases of figure skating for 40 years. A member of both PSA CER A, and ISI Gold judge, and USFS. BS from Ohio State University. She has coached students in Moves in the Field and Freestyle from beginner thru senior level. Phone: 239-878-0605 / Email: [email protected] Rate: $38.00 – 30 minutes, Beginner Rate: $24.00- 30 minutes Inna Koroleva Is from St. Petersburg Russia. She was a World Universidad Champion. Member of the Russian National /figure skating team and has competed internationally all over the world. 17 years of coaching/ choreography. Is PSA registered Principal star of "Holiday on Ice". Teaches beginner to advanced. Phone: 239-287-2734 / Email: [email protected] Rate: $38.00 – 30 minutes, Beginner Rate: $25.00- 30 minutes Ivan Dimitrov Ivan is a Bulgarian native and is a junior national champion in freestyle, junior Grand Prix and junior world competitor. He is a U.S. Nationals pairs skater. Ivan has 18 years of competitive experience and 14 years of coaching experience. He has coached U.S. Nationals athletes and medalists, as well as assisted in preparations for World’s and Olympian competitors. -

Meryl Davis Dating Charlie
Jun 22, · Meryl Davis and Fedor Andreev tied the knot in an "intimate" outdoor ceremony in the South of France on Saturday night, PEOPLE can exclusively confirm. Jan 15, · Meryl Elizabeth Davis is an American ice dancer. With partner Charlie White, she is the Olympic Champion, a two-time World champion, the Olympic silver medalist, two-time World silver medalist, five-time Grand Prix Final champion and six-time U.S. national champion ().Nationality: American. Apr 25, · Charlie married his wife Tanith Belbin White in the year White marrying Tanith shut all the rumors about White dating Davis. Tanith is a Canadian-American ice dancer and Olympic Program Host for NBC Sports. Although she was born in Canada, she holds dual citizenship and has for the US. Charlie White teamed up with Meryl Davis in Gradually rumors about the duo dating . Meryl Davis (born January 1, ) is an American ice dancer. With partner Charlie White, she is the Olympic champion, the Olympic silver medalist, a two-time (, ) World champion, five-time Grand Prix Final champion (–), three-time Four Continents champion (, , ) and six-time U.S. national champion (–).Birth place: Royal Oak. They're getting married! Dancing With the Stars champ Meryl Davis is engaged to Fedor Andreev, a former figure skater (who also happens to be the son of her longtime coach, Marina Zoueva). She. Charles Allen "Charlie" White Jr. (born October 24, ) is an American ice renuzap.podarokideal.ru partner Meryl Davis, he is the Olympic Champion, the Olympic silver medalist, a two-time (, ) World champion, five-time Grand Prix Final champion (–), three-time Four Continents champion (, , ) and six-time U.S. -
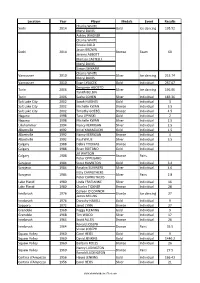
List of All Olympics Prize Winners in Figure Skating in U.S.A
Location Year Player Medals Event Results Charlie WHITE Sochi 2014 Gold Ice dancing 195.52 Meryl DAVIS Ashley WAGNER Charlie WHITE Gracie GOLD Jason BROWN Sochi 2014 Bronze Team 60 Jeremy ABBOTT Marissa CASTELLI Meryl DAVIS Simon SHNAPIR Charlie WHITE Vancouver 2010 Silver Ice dancing 215.74 Meryl DAVIS Vancouver 2010 Evan LYSACEK Gold Individual 257.67 Benjamin AGOSTO Turin 2006 Silver Ice dancing 196.06 Tanith BELBIN Turin 2006 Sasha COHEN Silver Individual 183.36 Salt Lake City 2002 Sarah HUGHES Gold Individual 3 Salt Lake City 2002 Michelle KWAN Bronze Individual 3.5 Salt Lake City 2002 Timothy GOEBEL Bronze Individual 4.5 Nagano 1998 Tara LIPINSKI Gold Individual 2 Nagano 1998 Michelle KWAN Silver Individual 2.5 Lillehammer 1994 Nancy KERRIGAN Silver Individual 2.5 Albertville 1992 Kristi YAMAGUCHI Gold Individual 1.5 Albertville 1992 Nancy KERRIGAN Bronze Individual 4 Albertville 1992 Paul WYLIE Silver Individual 3.5 Calgary 1988 Debra THOMAS Bronze Individual Calgary 1988 Brian BOITANO Gold Individual Jill WATSON Calgary 1988 Bronze Pairs Peter OPPEGARD Sarajevo 1984 Scott HAMILTON Gold Individual 3.4 Sarajevo 1984 Rosalyn SUMNERS Silver Individual 4.6 Kitty CARRUTHERS Sarajevo 1984 Silver Pairs 2.8 Peter CARRUTHERS Lake Placid 1980 Linda FRATIANNE Silver Individual 16 Lake Placid 1980 Charles TICKNER Bronze Individual 28 Colleen O'CONNOR Innsbruck 1976 Bronze Ice dancing 27 James MILLNS Innsbruck 1976 Dorothy HAMILL Gold Individual 9 Sapporo 1972 Janet LYNN Bronze Individual 27 Grenoble 1968 Peggy FLEMING Gold Individual 9 Grenoble -

ISU WORLD FIGURE SKATING CHAMPIONSHIPS ® 2012, Nice
ISU WORLD FIGURE SKATING CHAMPIONSHIPS® 2012 March 26 – April 1, 2012, Nice / France Protocol of the ® ISU World Figure Skating Championships 2012 including preliminary rounds organized by Fédération Française des Sports de Glace with the authorization of the International Skating Union held in Nice / France March 26 – April 1, 2012 The events of the Championships took place at the “Palais des Expositions” an artificial and heated indoor ice surface. Official ISU Sponsors ISU WORLD FIGURE SKATING CHAMPIONSHIPS® 2012 March 26 – April 1, 2012, Nice / France International Skating Union (ISU) Council President: Ottavio Cinquanta Italy 1st Vice President Figure Skating: David M. Dore Canada 2nd Vice President Speed Skating: Jan Dijkema Netherlands Members Figure Skating: Marie Lundmark Finland Junko Hiramatsu Japan Phyllis Howard U.S.A. Tjasa Andrée-Prosenc Slovenia Speed Skating: György Martos Hungary German Panov Russia Lan Li China Roland E. Maillard Switzerland ISU Director General Fredi Schmid Switzerland ISU Chair Sports Directorate Peter Krick Germany ISU Figure Skating Sports Director Krisztina Regöczy Hungary ISU Speed Skating Sports Director Hugo Herrnhof Italy Technical Committees Single & Pair Skating Chairperson: Alexander Lakernik Russia Members: Fabio Bianchetti Italy Rita Zonnekeyn Belgium Susan Lynch Australia Appointed Skater: Patrick Meier Switzerland Appointed Coach: David P. Kirby U.S.A. Ice Dance Chairperson: Halina Gordon-Poltorak Poland Members: Robert Horen U.S.A. Gilles Vandenbroeck France Alla Shekhovtsova Russia Appointed Skater: Sylwia Nowak-Trebacka Poland Appointed Coach: John Dunn Great Britain Synchronized Skating Chairperson: Christopher Buchanan Great Britain Members: Mika Saarelainen Finland Karen Wolanchuk USA Philippe Maitrot France Appointed Skater: Helena Johansson Finland Appointed Coach: Cathy Dalton Canada Official ISU Sponsors ISU WORLD FIGURE SKATING CHAMPIONSHIPS® 2012 March 26 – April 1, 2012, Nice / France ISU Event Officials ISU Representative: Mr. -

Lake Placid Ice Dance Championships Olympic Center, Lake Placid New York August 4 -7, 2004 Report of Skaters from All Clubs
Lake Placid Ice Dance Championships Olympic Center, Lake Placid New York August 4 -7, 2004 Report of Skaters from All Clubs - Standings for the First Dance Intermediate Compulsory Dance Group A - Final Standings 1 Jill Bakker, BKV - The Netherlands 1 Piper Gilles, Broadmoor SC 1 Spencer Barnes, Scarborough FSC 1 Tim McKernan, Broadmoor SC 2 William Avila, Escondido FSC 2 Chloe Wolf, North Atlantic FSC 2 Sara Bailey, Charter Oak FSC 2 Rhys Ainsworth, North Atlantic FSC 3 Alisa Allapach, All Year FSC 3 Gianna Katsaros, Straigsville FSC 3 Michael Amick, Central FL FSC 3 Daniel Witt, Winterhurst FSC 4 Margeaux Annalett, Amherst SC 4 Brin Adams, Granite State FSC 4 Alyssa Arevalo, Individual Member 4 Wayne Roswell, Granite State FSC 5 Molly Elizabeth Bennett, UDFSC 5 Amber Bogart, Stars FSC of TX 5 Kevin Bisson, Acton Vale 5 Robert Cuthbertson, Stars FSC of TX 6 Brin Adams, Granite State FSC 6 Jenna Kaufman-Ross, Garden State FSC 6 Shela Adams, Granite State FSC 6 Marshall Green, SC of Morris 7 Rhys Ainsworth, North Atlantic FSC 7 Bianca Zuckerman, Fairbanks FSC 7 Alisa Allapach, All Year FSC 7 Baxter Norman Burbank, Fairbanks FSC 8 Ashton Blust, Philadelphia SC & HS 8 Casey Smith, Washington FSC 8 Emily Blynn, Philadelphia SC & HS 8 Boris Nouchtaev, Washington FSC 9 Evan Bates, Ann Arbor FSC 9 Rebecca Faye Lerman, City of Palms FSC 9 Jenna Beatty, Atlantic City FSC 9 Jamie Alex Lerman, City of Palms FSC 10 Michael Amick, Central FL FSC 10 Radina Hakim, Central FL FSC 10 Margeaux Annalett, Amherst SC 10 Michael Amick, Central FL FSC - Standings -

Coach Bio Website July 2019
HERTZ ARENA FIGURE SKATING COACHES Alper Ucar Alper graduated from Semmelweiss University in Budapest, Hungary with Physical Education and Biomechanics. He coached in Europe (Holland, Sweden, and Hungary) for over 8 years. Recently he has been coaching Ice Dance at the Detroit skating club and artic ice edge in Canton, Michigan. In 2018 at the Sevilla Congress Alper was appointed by the International Skating Union as an appointed Skater and Ice Dance Technical Committee member. He is an Ice Dance Athlete commissioner with active duty until 2019 World Championships. He is also a National Turkish Technical Specialist in Ice Dance and expertise in Partnering Ice Dance Pattern Dance. With 28 years of competitive experience Alper’s accomplishments include: -Turkish National Champion in freestyle -Balkan Champion in freestyle -International medal winner in freestyle -European and World Champion in freestyle Alper converted to Ice Dance at the age of 24 and became: -National Champion in Ice Dance -2011 Universiade Silver Medalist -Numerous international medals -European and World competitor -2014 Sochi Olympic winter games competitor -2018 Pyeong Chang Olympic winter games competitor Phone: 248-722-4672 / Email: [email protected] Rate: $45 -30 minutes Diane Myers Has been teaching all phases of figure skating for 40 years. A member of both PSA CER A, and ISI Gold judge, and USFS. BS from Ohio State University. She has coached students in Moves in the Field and Freestyle from beginner thru senior level. Phone: 239-878-0605 / Email: [email protected] Rate: $38.00 – 30 minutes, Beginner Rate: $24.00- 30 minutes Ilya Tkachenko Ilya has an Associate of Science, The teacher of physical training and sports from the 2008 School of Olympic reserve – Odintsovo, Moscow region of Russia. -

2019-20 U.S. FIGURE SKATING MEDIA GUIDE Nathan Chen 2019 World Champion Vincent Zhou 2019 World Bronze Medalist TABLE of CONTENTS
2019-20 U.S. FIGURE SKATING MEDIA GUIDE Nathan Chen 2019 World champion Vincent Zhou 2019 World bronze medalist TABLE OF CONTENTS U.S. FIGURE SKATING U.S. Ladies Team .....................31 Marketing & Communications Staff ...... 2 U.S. Men’s Team ......................45 Media Credential Guidelines ............ 3 U.S. Pairs Team ......................63 Headquarters ..........................6 U.S. Ice Dance Team .................75 Figure Skating on Television ............ 7 HISTORY & RESULTS Streaming Figure Skating Online . .8 History of Figure Skating ..............88 Figure Skating by the Numbers .........9 World & U.S. Hall of Fame ............ 90 Figure Skating Record Book .......... 94 VIEWERS GUIDE TO FIGURE SKATING Olympic Winter Games ............... 102 Disciplines ............................ 10 World Championships ................108 Ladies & Men’s .........................11 World Junior Championships ......... 128 Pairs .................................12 Four Continents Championships ...... 138 Ice Dance ............................13 Grand Prix Final. .144 INTERNATIONAL JUDGING SYSTEM Junior Grand Prix Final ...............150 Overview .............................14 Skate America ....................... 156 Judges & Officials .....................15 U.S. Championships .................. 165 Program Components .................16 IJS Best Scores ...................... 185 Calculations ..........................17 U.S. Qualifying Best Scores ........... 189 Scales of Values (SOV) ................18 Skate America Best -

Event 2 (Of 6)
I N T E R N A T I O N A L S K A T I N G U N I O N HEADQUARTERS ADDRESS: CHEMIN DE PRIMEROSE 2 - CH 1007 LAUSANNE - SWITZERLAND TELEPHONE (+41) 21 612 66 66 TELEFAX (+41) 21 612 66 7 E-MAIL: [email protected] February 17, 2014 Sochi 2014 Olympic Winter Games Figure Skating Ice Dance Free Dance The figure skating competition at the 2014 Olympic Winter Games continued in Sochi, Russia, on Monday with the Free Dance. Meryl Davis/Charlie White (USA) dance off with Olympic gold Meryl Davis/Charlie White (USA) danced off with the gold medal at the Sochi 2014 Olympic Winter Games at the Iceberg Skating Palace on Monday, winning the first Olympic Ice Dance gold for the USA. 2010 Olympic champions Tessa Virtue/Scott Moir of Canada earned the silver medal and Russia’s Elena Ilinykh/Nikita Katsalapov claimed the bronze. Performing to "Sherazade", Davis/White impressed the audience and judges with their difficult lifts and fast footwork. The 2013 world champions picked up a level four for all their elements. Their free dance score of 116.63 points was not only a personal best but another highest score as was their total score of 195.52 points. "We're so excited we're kind of in shock a little," Davis said. "I'm not sure what we're feeling. It kind of all came together for us and we're so pleased to be here. We're kind of in disbelief”, she added. “It felt like we had done everything we could from the beginning of this competition, in practice, team event, this event. -

Bring Your Group to See America's Champions and Breakout Stars!
Bring your Group to see America’s Champions and Breakout Stars! In 2017, Stars on Ice brings together a cast of our country’s most decorated and promising young skaters! Olympic Gold Medalists Meryl Davis & Charlie White are joined by World Medalists Ashley Wagner and Madison Chock & Evan Bates, U.S. Champions Gracie Gold, Jeremy Abbott, Adam Rippon, U.S. Bronze Medalists Madison Hubbell & Zachary Donohue and special guests — 2017 U.S. Champions Nathan Chen and Karen Chen in a star-studded event leading up to the 2018 Olympic Games! Seeing Stars on Ice live is an unforgettable experience that is perfect for sharing with your group. Groups of 10 or more can take advantage of discounted ticket pricing and the exclusive benefits listed below that are only available with a group ticket purchase. 2017 GROUP SALES – SPECIAL OFFERS 10+ TICKETS Exclusive $10 discount per ticket on all but on-ice seats 20-49 TICKETS Ticket discount plus two free tickets and one cast-signed poster 50-99 TICKETS Ticket discount, four free tickets, three cast-signed posters and admission for your group to pre-show warm-ups and the ALL-NEW ICEBREAKER session featuring U.S. National Ice Dance Champions and World Medalists Madison Chock & Evan Bates 100+ TICKETS Ticket discount, six free tickets, three cast-signed posters, admission for your group to pre-show warm-ups and the ALL-NEW ICEBREAKER session featuring U.S. National Ice Dance Champions and World Medalists Madison Chock & Evan Bates, a “Welcome” announcement before the show, an autographed Stars on Ice card for each member of your group, and a skater visit during the pre-show warm-up starsonice.com DATE AND CAST SUBJECT TO CHANGE. -

Figure Skating
Figure Skating – Mixed Ice Dancing Medals Won by Countries RankUS RankEuro NOC Gold Silver Bronze Totals 1 1 Soviet Union 3 3 2 8 2 2 Russia 3 3 1 7 3 3 France 1 1 1 3 4 7 United States - 2 1 3 =5 =4 Canada 1 - 1 2 =5 =4 Great Britain 1 - 1 2 =5 =4 Unified Team 1 - 1 2 Most Medals 1 Colleen O'Connor (1976-001) 1 Tanith Belbin (2006-010) 1 Meryl Davis (2010-010) 1 Jim Millns, Jr. (1976-001) 1 Ben Agosto (2006-010) 1 Charlie White (2010-010) Youngest Competitor, USA 15-319 Jessica Joseph (USA-1998, *31 March 1982) 18-064 Rachel Mayer (USA-1992, *12 December 1973) 18-228 Judi Genovesi (USA-1976, *21 June 1957) 19-281 Emily Samuelson (USA-2010, *14 May 1990) 20-269 Elisa Spitz (USA-1984, *17 May 1963) 18-316 Charles Butler (USA-1998, *4 April 1979) 20-048 Michael Seibert (USA-1980, *1 January 1960) 20-352 Kent Weigle (USA-1976, *17 February 1955) 20-361 Evan Bates (USA-2010, *23 February 1989) 22-044 Ryan O'Meara (USA-2006, *5 January 1984) Youngest Medalist, USA 21-224 Tanith Belbin (2006, *11 July 1984) 23-052 Meryl Davis (2010, *1 January 1987) 22-122 Charlie White (2010, *24 October 1987) 24-036 Ben Agosto (2006, *15 January 1982) Oldest Competitor, USA 27-213 Carol Fox (USA-1984, *11 July 1956) 27-035 Elizabeth Punsalan (USA-1998, *9 January 1971) 26-150 Judy Blumberg (USA-1984, *13 September 1957) 25-321 Stacey Smith (USA-1980, *3 April 1954) 25-223 Tanith Belbin (USA-2010, *11 July 1984) 33-049 Charles Sinek (USA-2002, *28 December 1968) 31-118 Jerod Swallow (USA-1998, *18 October 1966) 31-009 Peter Tchernyshev (USA-2002, *6 February 1971) 30-011 Russ Witherby (USA-1992, *3 February 1962) 28-205 Scott Gregory (USA-1988, *31 July 1959) Oldest Medalist, USA 24-054 Colleen O'Connor (1976, *17 December 1951) 23-052 Meryl Davis (2010, *1 January 1987) 27-026 Jim Millns, Jr.