Clinical Evaluation of Oral Diseases
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Lumps and Swellings
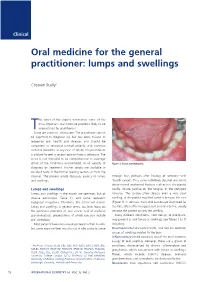
Clinical Oral medicine for the general practitioner: lumps and swellings Crispian Scully 1 his series of five papers summarises some of the most important oral medicine problems likely to be Tencountered by practitioners. Some are common, others rare. The practitioner cannot be expected to diagnose all, but has been trained to recognise oral health and disease, and should be competent to recognise normal variants, and common orofacial disorders. In any case of doubt, the practitioner is advised to seek a second opinion from a colleague. The series is not intended to be comprehensive in coverage either of the conditions encountered, or all aspects of Figure 1: Torus mandibularis. diagnosis or treatment: further details are available in standard texts, in the further reading section, or from the internet. The present article discusses aspects of lumps through fear, perhaps after hearing of someone with and swellings. ‘mouth cancer’. Thus some individuals discover and worry about normal anatomical features such as tori, the parotid Lumps and swellings papilla, foliate papillae on the tongue, or the pterygoid Lumps and swellings in the mouth are common, but of hamulus. The tongue often detects even a very small diverse aetiologies (Table 1), and some represent swelling, or the patient may first notice it because it is sore malignant neoplasms. Therefore, this article will discuss (Figure 1). In contrast, many oral cancers are diagnosed far lumps and swellings in general terms, but later focus on too late, often after being present several months, usually the particular problems of oral cancer and of orofacial because the patient ignores the swelling. -

High Frequency of Allelic Loss in Dysplastic Lichenoid Lesions
0023-6837/00/8002-233$03.00/0 LABORATORY INVESTIGATION Vol. 80, No. 2, p. 233, 2000 Copyright © 2000 by The United States and Canadian Academy of Pathology, Inc. Printed in U.S.A. High Frequency of Allelic Loss in Dysplastic Lichenoid Lesions Lewei Zhang, Xing Cheng, Yong-hua Li, Catherine Poh, Tao Zeng, Robert Priddy, John Lovas, Paul Freedman, Tom Daley, and Miriam P. Rosin Faculty of Dentistry (LZ, Y-HL, CP, RP), University of British Columbia, and BC Cancer Research Centre (MPR), Cancer Control Unit, Vancouver, British Columbia, School of Kinesiology (XC, TZ, MPR), Simon Fraser University, Burnaby, British Columbia, Faculty of Dentistry (JL), Dalhousie University, Halifax, Nova Scotia, and Department of Pathology (TD), University of Western Ontario, London, Ontario, Canada; and The New York Hospital Medical Center of Queens (PF), Flushing, New York SUMMARY: Oral lichen planus (OLP) is a common mucosal condition that is considered premalignant by some, whereas others argue that only lichenoid lesions with epithelial dysplasia are at risk of progressing into oral carcinoma. A recent study from this laboratory used microsatellite analysis to evaluate OLP for loss of heterozygosity (LOH) at loci on three chromosomal arms (3p, 9p, and 17p) (Am J Path 1997;Vol151:Page323-Page327). Loss on these arms is a common event in oral epithelial dysplasia and has been associated with risk of progression of oral leukoplakia to cancer. The data showed that, although dysplastic epithelium demonstrated a high frequency of LOH (40% for mild dysplasia), a significantly lower frequency of LOH was noted in OLP (6%), which is even lower than that in hyperplasia (14%). -

White Lesions of the Oral Cavity and Derive a Differential Diagnosis Four for Various White Lesions
2014 self-study course four course The Ohio State University College of Dentistry is a recognized provider for ADA, CERP, and AGD Fellowship, Mastership and Maintenance credit. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns or complaints about a CE provider may be directed to the provider or to ADA CERP at www.ada.org/goto/cerp. The Ohio State University College of Dentistry is approved by the Ohio State Dental Board as a permanent sponsor of continuing dental education ABOUT this FREQUENTLY asked COURSE… QUESTIONS… Q: Who can earn FREE CE credits? . READ the MATERIALS. Read and review the course materials. A: EVERYONE - All dental professionals in your office may earn free CE contact . COMPLETE the TEST. Answer the credits. Each person must read the eight question test. A total of 6/8 course materials and submit an questions must be answered correctly online answer form independently. for credit. us . SUBMIT the ANSWER FORM Q: What if I did not receive a ONLINE. You MUST submit your confirmation ID? answers ONLINE at: A: Once you have fully completed your p h o n e http://dent.osu.edu/sterilization/ce answer form and click “submit” you will be directed to a page with a . RECORD or PRINT THE 614-292-6737 unique confirmation ID. CONFIRMATION ID This unique ID is displayed upon successful submission Q: Where can I find my SMS number? of your answer form. -

Oral Pigmented Lesions from Brazil
Med Oral Patol Oral Cir Bucal. 2021 May 1;26 (3):e284-91. Oral pigmented lesions from Brazil Journal section: Oral Medicine and Pathology doi:10.4317/medoral.24168 Publication Types: Research Oral pigmented lesions: a retrospective analysis from Brazil Danielle Mendes da Silva Albuquerque 1, John Lennon Silva Cunha 2, Ana Luiza Oliveira Corrêa Roza 3, Lady Paola Aristizabal Arboleda 3, Alan Roger Santos-Silva 4, Marcio Ajudarte Lopes 4, Pablo Agustin Vargas 4, Jacks Jorge 4, Oslei Paes de Almeida 4, Aline Corrêa Abrahão 5, Michelle Agostini 5, Mário José Romañach 5, Bruno Augusto Benevenuto de Andrade 5 1 DDS, MSc. Department of Oral Diagnosis and Pathology, School of Dentistry, Federal University of Rio de Janeiro (UFRJ), Brazil 2 DDS, MSc student. Department of Oral Diagnosis, Piracicaba Dental School, University of Campinas (UNICAMP), SP, Brazil 3 DDS, PhD student. Department of Oral Diagnosis, Piracicaba Dental School, University of Campinas (UNICAMP), SP, Brazil 4 DDS, PhD. Department of Oral Diagnosis, Piracicaba Dental School, University of Campinas (UNICAMP), SP, Brazil 5 DDS, PhD. Department of Oral Diagnosis and Pathology, School of Dentistry, Federal University of Rio de Janeiro (UFRJ), Brazil Correspondence: Department of Oral Diagnosis and Pathology Federal University of Rio de Janeiro School of Dentistry Av. Carlos Chagas Filho 373, Prédio do CCS, Bloco K, 2° andar, Sala 56 Ilha da Cidade Universitária, Rio de Janeiro/RJ. 21.941-902 [email protected] Received: 16/07/2020 Albuquerque DMdS, Cunha JLS, Roza ALOC, Arboleda LPA, Santos- Accepted: 24/08/2020 Silva AR, Lopes MA, et al. Oral pigmented lesions: a retrospective analysis from Brazil. -

Orofacial Granulomatosis
Al-Hamad, A; Porter, S; Fedele, S; (2015) Orofacial Granulomatosis. Dermatol Clin , 33 (3) pp. 433- 446. 10.1016/j.det.2015.03.008. Downloaded from UCL Discovery: http://discovery.ucl.ac.uk/1470143 ARTICLE Oro-facial Granulomatosis Arwa Al-Hamad1, 2, Stephen Porter1, Stefano Fedele1, 3 1 University College London, UCL Eastman Dental Institute, Oral Medicine Unit, 256 Gray’s Inn Road, WC1X 8LD, London UK. 2 Dental Services, King Abdulaziz Medical City-Riyadh, Ministry of National Guard, Riyadh, Saudi Arabia. 3 NIHR University College London Hospitals Biomedical Research Centre, London, UK. Acknowledgments: Part of this work was undertaken at University College London/University College London Hospital, which received a proportion of funding from the Department of Health’s National Institute for Health Research Biomedical Research Centre funding scheme. Conflicts of Interest: The authors declare that they have no affiliation with any organization with a financial interest, direct or indirect, in the subject matter or materials discussed in the manuscript that may affect the conduct or reporting of the work submitted. Authorship: all authors named above meet the following criteria of the International Committee of Medical Journal Editors: 1) Substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; 2) Drafting the article or revising it critically for important intellectual content; 3) Final approval of the version to be published. Corresponding author: Dr. Stefano Fedele DDS, PhD -

Features of Reactive White Lesions of the Oral Mucosa
Head and Neck Pathology (2019) 13:16–24 https://doi.org/10.1007/s12105-018-0986-3 SPECIAL ISSUE: COLORS AND TEXTURES, A REVIEW OF ORAL MUCOSAL ENTITIES Frictional Keratosis, Contact Keratosis and Smokeless Tobacco Keratosis: Features of Reactive White Lesions of the Oral Mucosa Susan Müller1 Received: 21 September 2018 / Accepted: 2 November 2018 / Published online: 22 January 2019 © Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract White lesions of the oral cavity are quite common and can have a variety of etiologies, both benign and malignant. Although the vast majority of publications focus on leukoplakia and other potentially malignant lesions, most oral lesions that appear white are benign. This review will focus exclusively on reactive white oral lesions. Included in the discussion are frictional keratoses, irritant contact stomatitis, and smokeless tobacco keratoses. Leukoedema and hereditary genodermatoses that may enter in the clinical differential diagnoses of frictional keratoses including white sponge nevus and hereditary benign intraepithelial dyskeratosis will be reviewed. Many products can result in contact stomatitis. Dentrifice-related stomatitis, contact reactions to amalgam and cinnamon can cause keratotic lesions. Each of these lesions have microscopic findings that can assist in patient management. Keywords Leukoplakia · Frictional keratosis · Smokeless tobacco keratosis · Stomatitis · Leukoedema · Cinnamon Introduction white lesions including infective and non-infective causes will be discussed -

Orofacial Granulomatosis Presenting As Gingival Enlargement – Report of Three Cases
Open Access Journal of Dentistry & Oral Disorders Case Report Orofacial Granulomatosis Presenting as Gingival Enlargement – Report of Three Cases Savithri V*, Janardhanan M, Suresh R and Aravind T Abstract Department of Oral Pathology & Microbiology, Amrita Orofacial Granulomatosis (OFG) is an uncommon disease characterized School of Dentistry, Amrita VishwaVidyapeetham, Amrita by non-caseating granulomatous inflammation in the oral and maxillofacial University, India region. They present clinically as labial enlargement, perioral and/or mucosal *Corresponding author: Vindhya Savithri, swelling, angular cheilitis, mucosal tags, vertical fissures of lips, lingua plicata, Department of Oral Pathology & Microbiology, Amrita oral ulcerations and gingival enlargement. The term OFG was introduced by School of Dentistry, Amrita VishwaVidyapeetham, Amrita Wiesenfeld in 1985. The diagnosis of OFG is done by the clinical presentation University, India and histological picture and this may be further complicated by the fact that OFG may be the oral manifestation of a systemic condition, such as Crohn’s Received: October 16, 2017; Accepted: November 27, disease, sarcoidosis, or, more rarely, Wegener’s granulomatosis. In addition, 2017; Published: December 04, 2017 several conditions, including tuberculosis, leprosy, systemic fungal infections, and foreign body reactions may show granulomatous inflammation on histologic examination. They have to be excluded out by appropriate investigations. They have to be excluded out by appropriate investigations. -

Amalgam Pigmentation) on the Palatal Mucosa: a Case Report
Open Access Journal of Dentistry & Oral Disorders Case Report Extensive Amalgam Tattoo (Amalgam Pigmentation) on the Palatal Mucosa: A Case Report Fiqhi MK1*, Essaoudi MA2, Khalfi 1L and Khatib KE1 Abstract 1 Department of Plastic, Maxillofacial and Oral Surgery, Introduction: Amalgam tattoo is the most common exogenous oral Mohammed V Military Teaching Hospital, Rabat, pigmentation, caused by traumatic implantation of dental amalgam into soft Morocco tissue. 2Department of Anatomic Pathology, Mohammed V Military Teaching Hospital, Rabat, Morocco Observation: We report a case of large amalgam pigmentation on right hard palate. *Corresponding author: Fiqhi Mohammed Kamal, Department of Plastic, Maxillofacial and Oral Surgery, Discussion: Amalgam tattoo can sometimes be confused with melanotic Mohammed V Military Teaching Hospital, Rabat, lesions, being then biopsied. Once the diagnosis of amalgam tattoos has been Morocco established, the removal of lesions is not necessary, except for esthetic reasons. Received: March 02, 2018; Accepted: April 03, 2018; Keywords: Amalgam tattoo; Oral mucosa; Pigmentation Published: April 10, 2018 Introduction Oral pigmentations may be classified into two major groups on the basis of their clinical appearance: focal and diffuse pigmentations. All pigmented oral cavity lesions should be viewed with suspicion to eliminate a malignant melanoma. This article deals with an extensive amalgam tattoo lesion on palatal mucosa which required a biopsy for a definitive diagnosis. Case Presentation A 56-year-old man with an unremarkable medical history was referred to the department of maxillofacial surgery on suspicion of mucosal melanoma. Clinical examination found a large brown flat macula located on the right hard palate adjacent to a restored tooth 16 with presence of amalgam fillings (Figure 1). -

White Sponge Nevus
Scholars Journal of Applied Medical Sciences (SJAMS) ISSN 2320-6691 (Online) Abbreviated Key Title: Sch. J. App. Med. Sci. ISSN 2347-954X (Print) ©Scholars Academic and Scientific Publisher A Unit of Scholars Academic and Scientific Society, India Dental Medicine www.saspublisher.com White Sponge Nevus: Report of Case And Literature Review Hasni W1,2*, Hassouna MO1, Slim A1, Ben Massoud N1,2, Ben Youssef S1,2, Abdelatif B1,2 1Oral Surgery Unit, Dental Medicine Department, University Hospital Farhat Hached, Sousse, University of Monastir, Tunisia North Africa 2Research Laboratory: Functional and Aesthetic Rehabilitation of Maxillary (LR 12SP10) , Tunisia North Africa Abstract: White sponge nevus (WSN) is a rare benign autosomal dominant disorder. Case Report To date, a few hundred cases have been reported worldwide. It is usually manifested as white, soft, and spongy plaque involving the mucous membrane, predominantly the *Corresponding author oral mucosa. Careful clinical and histopathological examination is recommended to Hasni W exclude other more serious disorder presenting as oral white lesions. Herein, we present the second Tunisian case of oral WSN in an 18-year-old female with no Article History familial background. Current approaches in literature to the diagnosis and treatment Received: 20.10.2018 were also studied. Accepted: 28.10.2018 Keywords: Oral mucosa, Hereditary Mucosal Leukokeratosis, White lesion, white Published: 30.10.2018 sponge nevus. DOI: INTRODUCTION 10.21276/sjams.2018.6.10.88 White sponge nevus (WSN) is a rare, benign condition affecting the mucous membranes. It was first described by Hyde in 1909 but the term WSN was introduced by Canon in 1935 [1, 2].It is an autosomal dominant mucosal disorder that affects non keratinizing stratified epithelia, primarily the oral mucosa. -

Orofacial Granulomatosis: a Review
DOI Number: 10.5958/0974-1283.2019.00181.6 Orofacial Granulomatosis: A Review Saloni Banga1, M K Sunil2, Hina Padaliya1 1Intern, 2Professor and Head of Department, Department of Oral Medicine & Radiology, Teerthanker Mahaveer Dental College & Research Center Moradabad Abstract Orofacial Granulomatosis (OFG) is an uncommon clinicopathological entity characterized clinically by the presence of persistent enlargement of the soft tissues of the oral and maxillofacial region and histologically by non-caseating and non-necrotizing granulomatous inflammation. The term ‘orofacial granulomatosis’ has been introduced to denote the group of various disorders, including Melkersson-Rosenthal syndrome and granulomatous cheilitis and has been noted to be associated with Crohn’s disease, Sarcoidosis and infectious diseases such as Tuberculosis. Although, various etiological agents such as dental materials, food additives and microbial agents have been recommended in the disease process. Treatment of orofacial granulomatosis is by corticosteroids but it’s not so efficient. It is more important to identify the pathogen first to specify the appropriate treatment line. Keywords— orofacial granulomatosis, Melkersson Rosenthal syndrome, crohn,s disease. Introduction Definition and its associated to other granulomatous disorders Orofacial granulomatosis term was introduced by Wiesenfeld in 19851. Granulomatosis is any condition Orofacial granulomatosis is an uncommon disorder1 characterized by the formation of multiple nodules or but is increasingly recognized. Orofacial granulomatosis granulomas in soft tissues. It encompasses Melkersson (as defined by Wiesenfeld in 1985) is the specific Rosenthal syndrome and Cheilitis granulomatosa1. histological finding of granulomas in mucosal or skin The true prevalence of this disease is unknown but is biopsies taken from the mouth or face in the absence suggested to be 0.8% (Mahler and Kiesewetter, 1996)3. -

Nurses' Knowledge, Attitude and Practice Toward Mouth
ISSN 2394-7330 International Journal of Novel Research in Healthcare and Nursing Vol. 3, Issue 3, pp: (1-15), Month: September - December 2016, Available at: www.noveltyjournals.com NURSES’ KNOWLEDGE, ATTITUDE AND PRACTICE TOWARD MOUTH HYGIENE AMONG CRITICAL ILL PATIENTS 1Samira Ebrahim Aboalizm, 2Zeinab Abdel Aziz Kasemy 1Lecturer of Medical surgical nursing department-Faculty of nursing- Menoufia University 2Lecturer of Public Health& Community Medicine- Faculty of Medicine - Menoufia University Abstract: Background: Mouth cleanliness is very important for critical patients in hospital; it is usually the accountability of nurses with adequate information for mouth hygiene, guiding principle and rate of performance oral needed to prevent spread of infection. Aim: The aim of this study was to assess nurses’ knowledge, attitude and practice toward oral care among critical ill patients. Subjects & méthod: Research design: Descriptive research was utilized. Setting: intensive care units at Menoufia University Hospital. Subjects: convenience sample of all nurses working in intensive care units; 100 nurses at Menoufia University. Tools: One tool was utilized for data collection: 1-Structure interview questionnaire schedule: It consists of 5 parts. Part I: demographic characteristics, Part 2: knowledge questionnaire sheet, Part 3: - mouth hygiene practice sheet, Part 4: - attitudes regarding mouth hygiene, Part 5: Types and frequency of oral care: Results: more than half of the group had lack of time to practice of mouth hygiene. More than half (64%) of nurses had good knowledge and (16%) of the nurses had not any knowledge about oral care. The higher majority of nurses were agreeing that mouth hygiene was very important to ventilate patients. -

Pigmented Lesions of the Oral Mucosa
Assistant Professor Dr : Ameena Ryhan Lecture 1 Pigmented Lesions of the Oral Mucosa Endogenous Pigmentation ❒❒ Focal Melanocytic Pigmentation 1. Freckle/Ephelis 2. Oral/Labial Melanotic Macule 3. Oral Melanoacanthoma 4. Melanocytic Nevus 5. Malignant Melanoma ❒❒ Multifocal/Diffuse Pigmentation 1. Physiologic Pigmentation 2. Drug-Induced Melanosis 3. Smoker’s Melanosis 4. Postinflammatory (Inflammatory) Hyperpigmentation 5. Melasma (Chloasma) ❒❒ Melanosis Associated with Systemic or Genetic Disease 1. Hypoadrenocorticism (Adrenal Insufficiency or Addison’s Disease) 2. Cushing’s Syndrome/Cushing’s Disease 3. Hyperthyroidism (Graves’ Disease) 4. Primary Biliary Cirrhosis 5. Vitamin B12 (Cobalamin) Deficiency 6. Peutz–Jeghers Syndrome 7. Café au Lait Pigmentation 8. HIV/AIDS-Associated Melanosis ❒❒ Idiopathic Pigmentation 1. Laugier–Hunziker Pigmentation ❒❒ Treatment of Mucocutaneous Melanosis ❒❒ Depigmentation 1. Vitiligo ❒❒ Hemoglobin and Iron-Associated Pigmentation 1. Ecchymosis 2. Purpura/Petechiae 3. Hemochromatosis Exogenous Pigmentation 1. Amalgam Tattoo 2. Graphite Tattoos 3. Ornamental Tattoos 4. Medicinal Metal-Induced Pigmentation 5. Heavy Metal Pigmentation 6. Drug-Induced Pigmentation 7. Hairy Tongue 1 Assistant Professor Dr : Ameena Ryhan Lecture 1 Healthy oral soft tissues present a typical pink to red hue with slight topographical variations of color. This chromatic range is due to the interaction of a number of tissues that compose the mucosal lining: The presence or absence of keratin on the surface epithelium The quantity, superficial or deep location of blood vessels in the subjacent stroma, The existence of lobules of adipocytes, The absence of melanin pigmentation in the basal cell layer of the epithelium. Although oral and perioral pigmentation may be physiologic in nature, particularly in individuals with dark skin complexion, in the course of disease, the oral mucosa and perioral tissues can assume a variety of discolorations, including brown, blue, gray, and black.