Management of Complicated Diverticulitis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Point-Of-Care Ultrasound to Assess Anuria in Children
CME REVIEW ARTICLE Point-of-Care Ultrasound to Assess Anuria in Children Matthew D. Steimle, DO, Jennifer Plumb, MD, MPH, and Howard M. Corneli, MD patients to stay abreast of the most current advances in medicine Abstract: Anuria in children may arise from a host of causes and is a fre- and provide the safest, most efficient, state-of-the-art care. Point- quent concern in the emergency department. This review focuses on differ- of-care US can help us meet this goal.” entiating common causes of obstructive and nonobstructive anuria and the role of point-of-care ultrasound in this evaluation. We discuss some indications and basic techniques for bedside ultrasound imaging of the CLINICAL CONSIDERATIONS urinary system. In some cases, as for example with obvious dehydration or known renal failure, anuria is not mysterious, and evaluation can Key Words: point-of-care ultrasound, anuria, imaging, evaluation, be directed without imaging. In many other cases, however, diagnosis point-of-care US can be a simple and helpful way to assess urine (Pediatr Emer Care 2016;32: 544–548) volume, differentiate urinary retention in the bladder from other causes, evaluate other pathology, and, detect obstructive causes. TARGET AUDIENCE When should point-of-care US be performed? Because this imag- ing is low-risk, and rapid, early use is encouraged in any case This article is intended for health care providers who see chil- where it might be helpful. Scanning the bladder first answers the dren and adolescents in acute care settings. Pediatric emergency key question of whether urine is present. -

Diverticular Abscess Presenting As a Strangulated Inguinal Hernia: Case Report and Review of the Literature
Ulster Med J 2007; 76 (2) 107-108 Presidential Address 107 Case Report Diverticular Abscess Presenting as a Strangulated Inguinal Hernia: Case Report and review of the literature. S Imran H Andrabi, Ashish Pitale*, Ahmed AS El-Hakeem Accepted 22 December 2006 ABSTRACT noted nausea, anorexia and increasing abdominal pain. She had no previous history of any surgery or trauma and was on Potentially life threatening diseases can mimic a groin hernia. warfarin for atrial fibrillation. We present an unusual case of diverticulitis with perforation and a resulting abscess presenting as a strangulated inguinal hernia. The features demonstrated were not due to strangulation of the contents of the hernia but rather pus tracking into the hernia sac from the peritoneal cavity. The patient underwent sigmoid resection and drainage of retroperitoneal and pericolonic abscesses. Radiological and laboratory studies augment in reaching a diagnosis. The differential diagnosis of inguinal swellings is discussed. Key Words: Diverticulitis, diverticular perforation, diverticular abscess, inguinal hernia INTRODUCTION The association of complicated inguinal hernia and diverticulitis is rare1. Diverticulitis can present as left iliac fossa pain, rectal bleeding, fistulas, perforation, bowel obstruction and abscesses. Our patient presented with a diverticular perforation resulting in an abscess tracking into the inguinal canal and clinically masquerading as a Fig 2. CT scan showing inflammatory changes with strangulated inguinal hernia. The management warranted an stranding of the subcutaneous fat in the left groin and a exploratory laparotomy and drainage of pus. large bowel diverticulum CASE REPORT On admission, she had a tachycardia (pulse 102 beats/min) and a temperature of 37.5OC. -

Overactive Bladder: What You Need to Know Whiteboard Animation Transcript with Shawna Johnston, MD and Emily Stern, MD
Obstetrics and Gynecology – Overactive Bladder: What You Need to Know Whiteboard Animation Transcript with Shawna Johnston, MD and Emily Stern, MD Overactive bladder (OAB) is a symptom-based disease state, which includes urinary frequency, nocturia, and urgency, with or without urgency incontinence. Symptoms of a urinary tract infection (UTI) are similar but additionally include dysuria (painful voiding) and hematuria. OAB tends to be a chronic progressive condition, while UTI symptoms are acute and may be associated with fever and malaise. In patients whose symptoms are unclear, urinalysis and urine culture may help rule out infection. If symptoms point to OAB, you should rule out: 1. Neurological disorders, such as multiple sclerosis, dementia, parkinson’s disease, and stroke. 2. Medical disorders such as diabetes, and 3. Prolapse, as women with obstructed voiding, usually from advanced prolapse, can have symptoms that mimic those of OAB. It is important to delineate how OAB symptoms affect a patient’s quality of life. Women with OAB are often socially isolated and sleep poorly. On history, pay attention to lifestyle factors such as caffeine and fluid intake, environmental triggers, and medications that may worsen symptoms like diuretics. Cognitive impairment and diabetes can influence OAB symptoms. Estrogen deficiency worsens OAB symptoms, so menopausal status and hormone use are important to note. Physical exam includes a screening sacral neurologic exam, an assessment for pelvic organ prolapse and a cough stress test to rule out stress urinary incontinence. On pelvic exam, look for signs of estrogen deficiency. Investigations include urinalysis, urine culture, and a post-void residual volume measurement. -

Dysuria White Paper
CASE STUDY SUMMARY Management of Dysuria for BPH Surgical Procedures Ricardo Gonzalez, M.D. Medical Director of Voiding Dysfunction at Houston Metro Urology, Houston, Texas Dysuria following Benign Prostatic approach, concentrating on one area without Hyperplasia (BPH) Procedures ‘jumping around.’ Keep the laser at .5 mm away from the tissue when using the GreenLight PV® Transient dysuria following surgical treatment system; and 3 mm or less for the GreenLight of benign prostatic hyperplasia (BPH) is not an HPS® and GreenLight XPS® systems. Care must uncommon occurrence regardless of treatment. also be taken at the bladder neck: Identify Many factors may contribute to dysuria after the UOs and trigone, use lower power these procedures, including irritation from the (60-80 watts) and avoid directing energy introduction of the cystoscope; the degree of into the bladder.” tissue necrosis; the surgical modality utilized; the surgical technique employed; and the patient’s condition. This paper will focus on Pre-and Post-Operative Management both pre-procedural as well as post-procedural of Dysuria management of irritative symptoms related to Dr. Ricardo Gonzalez is an expert in the surgical BPH procedures. treatment of BPH with the GreenLight Laser System. “I spend considerable time Contributors to Dysuria educating patients on what to expect after Ricardo Gonzalez, M.D., Medical Director of surgical treatment of BPH, including dysuria,” Voiding Dysfunction at Houston Metro Urology says Dr. Gonzalez. “Proper patient education states, “Inefficient surgical technique can encour- will prevent many unnecessary phone calls age coagulative necrosis, which may increase from patients.” inflammation. This is more likely to be the case Dr. -

Urinary System Diseases and Disorders
URINARY SYSTEM DISEASES AND DISORDERS BERRYHILL & CASHION HS1 2017-2018 - CYSTITIS INFLAMMATION OF THE BLADDER CAUSE=PATHOGENS ENTERING THE URINARY MEATUS CYSTITIS • MORE COMMON IN FEMALES DUE TO SHORT URETHRA • SYMPTOMS=FREQUENT URINATION, HEMATURIA, LOWER BACK PAIN, BLADDER SPASM, FEVER • TREATMENT=ANTIBIOTICS, INCREASE FLUID INTAKE GLOMERULONEPHRITIS • AKA NEPHRITIS • INFLAMMATION OF THE GLOMERULUS • CAN BE ACUTE OR CHRONIC ACUTE GLOMERULONEPHRITIS • USUALLY FOLLOWS A STREPTOCOCCAL INFECTION LIKE STREP THROAT, SCARLET FEVER, RHEUMATIC FEVER • SYMPTOMS=CHILLS, FEVER, FATIGUE, EDEMA, OLIGURIA, HEMATURIA, ALBUMINURIA ACUTE GLOMERULONEPHRITIS • TREATMENT=REST, SALT RESTRICTION, MAINTAIN FLUID & ELECTROLYTE BALANCE, ANTIPYRETICS, DIURETICS, ANTIBIOTICS • WITH TREATMENT, KIDNEY FUNCTION IS USUALLY RESTORED, & PROGNOSIS IS GOOD CHRONIC GLOMERULONEPHRITIS • REPEATED CASES OF ACUTE NEPHRITIS CAN CAUSE CHRONIC NEPHRITIS • PROGRESSIVE, CAUSES SCARRING & SCLEROSING OF GLOMERULI • EARLY SYMPTOMS=HEMATURIA, ALBUMINURIA, HTN • WITH DISEASE PROGRESSION MORE GLOMERULI ARE DESTROYED CHRONIC GLOMERULONEPHRITIS • LATER SYMPTOMS=EDEMA, FATIGUE, ANEMIA, HTN, ANOREXIA, WEIGHT LOSS, CHF, PYURIA, RENAL FAILURE, DEATH • TREATMENT=LOW NA DIET, ANTIHYPERTENSIVE MEDS, MAINTAIN FLUIDS & ELECTROLYTES, HEMODIALYSIS, KIDNEY TRANSPLANT WHEN BOTH KIDNEYS ARE SEVERELY DAMAGED PYELONEPHRITIS • INFLAMMATION OF THE KIDNEY & RENAL PELVIS • CAUSE=PYOGENIC (PUS-FORMING) BACTERIA • SYMPTOMS=CHILLS, FEVER, BACK PAIN, FATIGUE, DYSURIA, HEMATURIA, PYURIA • TREATMENT=ANTIBIOTICS, -

Chapter 31: Lower Urinary Tract Conditions in Elderly Patients
Chapter 31: Lower Urinary Tract Conditions in Elderly Patients Damon Dyche and Jay Hollander William Beaumont Hospital, Royal Oak, Michigan As our population ages, the number of patients pre- uroflow/urodynamic studies, and cystoscopy. Com- senting to their primary care physicians with uro- mon transurethral treatment modalities include re- logic problems is significantly increasing. Urologic section, laser ablation, and microwave or radiofre- issues are the third most common type of complaint quency therapy. in patients 65 yr of age or older and account for at There are two major approaches of medical ther- least a part of 47% of office visits.1 One of the most apy for prostatic outflow obstruction: relaxing the predominant urologic problems in elderly persons, prostate smooth muscle tissue or decreasing glan- ␣ and the focus of this chapter, is lower urinary tract dular volume. 1-adrenergic blockade relaxes the symptoms (LUTS). There are several disease pro- smooth muscle fibers of the prostatic stroma and cesses that can lead to LUTS, as well as a number of can significantly improve urine flow. Because ␣ consequences. In this chapter, we will give a brief blockade can also have significant cardiovascular ␣ overview of the major issues as they relate to elderly side effects, 1 selective medications were devel- persons. oped to specifically target the urinary system. Com- mon nonselective agents include terazosin and dox- azosin; selective medications are tamsulosin and BENIGN PROSTATIC HYPERPLASIA AND alfuzosin. 5-␣ reductase inhibitors block the con- LUTS version of testosterone 3 DHT, which is a potent stimulator of prostatic glandular tissue. This reduc- The prostate surrounds the male urethra between tion in local androgen stimulation results in a pro- the bladder neck and urinary sphincter like a gressive decrease in prostatic volume over a period doughnut. -

Urinary Retention in Women Workshop Chair: David Castro-Diaz, Spain 07 October 2015 08:30 - 11:30
W16: Urinary Retention in Women Workshop Chair: David Castro-Diaz, Spain 07 October 2015 08:30 - 11:30 Start End Topic Speakers 08:30 08:45 Urinary retention in women: concepts and pathophysiology David Castro-Diaz 08:45 08:50 Discussion All 08:50 09:05 Evaluation Tufan Tarcan 09:05 09:10 Discussion All 09:10 09:30 Conservative management Cristina Naranjo-Ortiz 09:30 09:35 Discussion All 09:35 09:55 Medical and surgical management Christopher Chapple 09:55 10:00 Discussion All 10:00 10:30 Break None 10:30 11:20 Typical clinical cases discussion All 11:20 11:30 Take home messages David Castro-Diaz Aims of course/workshop Urinary retention in women is rare and diverse. Diagnostic criteria are not agreed and epidemiology is not well known. Forms of urinary retention in women include: complete retention, incomplete or insufficient emptying and elevated post-void residual. It may be acute or chronic, symptomatic or asymptomatic. Etiology is multifactorial including anatomic or functional bladder outlet obstruction and bladder dysfunction related to neurological diseases, diabetes mellitus, aging, pharmacotherapy, pain and infective/inflammatory disease and idiopathic or unknown aetiology. This workshop will analyse and discuss physiopathology, evaluation and management of urinary retention in women from an integral, practical and evidence based approach. Learning Objectives 1. Identify urinary retention in women, its etiology and risk factors. 2. Carry out proper diagnosis of urinary retention in women as well as its relationship with risk and influent factors. 3. Properly manage female acute and chronic acute and chronic urinary retention with the different approaches including conservative, medical and surgical therapies. -

MANAGEMENT of ACUTE ABDOMINAL PAIN Patrick Mcgonagill, MD, FACS 4/7/21 DISCLOSURES
MANAGEMENT OF ACUTE ABDOMINAL PAIN Patrick McGonagill, MD, FACS 4/7/21 DISCLOSURES • I have no pertinent conflicts of interest to disclose OBJECTIVES • Define the pathophysiology of abdominal pain • Identify specific patterns of abdominal pain on history and physical examination that suggest common surgical problems • Explore indications for imaging and escalation of care ACKNOWLEDGEMENTS (1) HISTORICAL VIGNETTE (2) • “The general rule can be laid down that the majority of severe abdominal pains that ensue in patients who have been previously fairly well, and that last as long as six hours, are caused by conditions of surgical import.” ~Cope’s Early Diagnosis of the Acute Abdomen, 21st ed. BASIC PRINCIPLES OF THE DIAGNOSIS AND SURGICAL MANAGEMENT OF ABDOMINAL PAIN • Listen to your (and the patient’s) gut. A well honed “Spidey Sense” will get you far. • Management of intraabdominal surgical problems are time sensitive • Narcotics will not mask peritonitis • Urgent need for surgery often will depend on vitals and hemodynamics • If in doubt, reach out to your friendly neighborhood surgeon. Septic Pain Sepsis Death Shock PATHOPHYSIOLOGY OF ABDOMINAL PAIN VISCERAL PAIN • Severe distension or strong contraction of intraabdominal structure • Poorly localized • Typically occurs in the midline of the abdomen • Seems to follow an embryological pattern • Foregut – epigastrium • Midgut – periumbilical • Hindgut – suprapubic/pelvic/lower back PARIETAL/SOMATIC PAIN • Caused by direct stimulation/irritation of parietal peritoneum • Leads to localized -
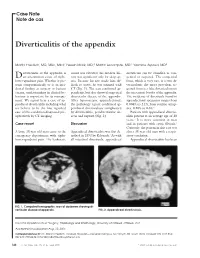
Diverticulitis of the Appendix
Case Note Note de cas Diverticulitis of the appendix Martin Friedlich, MD, MSc, MEd;* Neesh Malik, MD;† Martin Lecompte, MD;† Yasmine Ayroud, MD‡ iverticulitis of the appendix is count was elevated; his medical his- diverticula can be classified as con- Dan uncommon cause of right- tory was significant only for sleep ap- genital or acquired. The congenital lower-quadrant pain. Whether it pre- nea. Because his size made him dif- form, which is very rare, is a true di- sents symptomatically or is an inci- ficult to assess, he was scanned with verticulum; the more prevalent ac- dental finding at surgery or barium CT (Fig. 1). The scan confirmed ap- quired form is a false diverticulum on enema, understanding its clinical be- pendicitis, but also showed suspected the mesenteric border of the appendix. haviour is important for its manage- diverticular disease of the appendix. The incidence of diverticula found in ment. We report here a case of ap- After laparoscopic appendectomy, appendectomy specimens ranges from pendiceal diverticulitis including what the pathology report confirmed ap- 0.004% to 2.1%; from routine autop- we believe to be the first reported pendiceal diverticulosis complicated sies, 0.20% to 0.6%.2 case of this condition diagnosed pre- by diverticulitis, peridiverticular ab- Patients with appendiceal divertic- operatively by CT imaging. scess and rupture (Fig. 2). ulitis present at an average age of 38 years.3 It is more common in men Case report Discussion and in patients with cystic fibrosis.2 Curiously, the patient in this case was A large 38-year-old man came to the Appendiceal diverticulitis was first de- also a 38-year-old man with a respir- emergency department with right- scribed in 1893 by Kelynack.1 As with atory condition. -
Colonic Gallstone Obstruction
Advances in Clinical Medical Research and Healthcare Delivery Volume 1 Issue 1 Inaugural Issue Article 4 2021 Colonic Gallstone Obstruction Abdoulaziz Toure M.D Arnot Ogden Medical Center, [email protected] Mitchell Witkowski LECOM, [email protected] Vithal Vernenkar D.O Newark Wayne Community Hospital, [email protected] Brian Watkins MD, MS, FACS Newark Wayne Community Hospital, [email protected] Prasad V. Penmetsa M.D Rochester General Hospital, [email protected] Follow this and additional works at: https://scholar.rochesterregional.org/advances Part of the Health and Medical Administration Commons, Medical Education Commons, and the Medical Specialties Commons Recommended Citation Toure A, Witkowski M, Vernenkar V, Watkins B, Penmetsa PV. Colonic Gallstone Obstruction. Advances in Clinical Medical Research and Healthcare Delivery. 2021; 1(1). doi: 10.53785/2769-2779.1005. This Article is brought to you for free and open access by RocScholar. It has been accepted for inclusion in Advances in Clinical Medical Research and Healthcare Delivery by an authorized editor of RocScholar. ISSN: 2769-2779 Colonic Gallstone Obstruction Abstract This report discusses a case of a 79-year-old Caucasian female who presented with large bowel obstruction. A significant TC findings of cholecystocolic fistula and an impacted gallstone at the junction of the descending and sigmoid colon. We present a case of colonic gallstone obstruction that was treated with endoscopic lithotripsy. This interventional approach is effective in stable elderly patients with high surgical risk and in patients with significant comorbidities. Keywords gallstone complication, Cholecystocolic fistula, colonic gallstones, large bowel gallstones, gallstone ileus This article is available in Advances in Clinical Medical Research and Healthcare Delivery: https://scholar.rochesterregional.org/advances/vol1/iss1/4 Toure et al.: Colonic Gallstone Obstruction Background Gallstone ileus is a rare complication of cholelithiasis. -
Office Evaluation of Overactive Bladder: 4 Easy Steps
■ OBGMANAGEMENT BY MICKEY KARRAM, MD, and STEVE KLEEMAN, MD Office evaluation of overactive bladder: 4 easy steps Urgency, frequency, and urge incontinence can usually be diagnosed and managed without sophisticated urodynamic testing. 66-year-old woman complains of uri- Revised terminology nary urgency, frequency, and inconti- ne of the most notable changes in the Anence, and estimates that she voids 15 Oterms used to describe lower urinary tract or more times within a typical 24-hour period. dysfunction, proposed by the International So far, she has lost only small amounts of Continence Society,3 is organization of the ter- urine—because she hurries to void at the first minology into 3 categories: symptoms, signs, sense of urgency—but she is distressed and and urodynamic observations. worried that she will have a major accident. Symptoms are now defined to more closely Sound familiar? Overactive bladder affects 17 reflect the way the patient perceives her to 33 million US women.1 Thanks to greater problem, and are set forth without specifying awareness and openness, more women today are the volume of urine required for a diagnosis of seeking medical help for their troubling symptoms, “abnormal” sensation or urgency. although only a fraction have done so up to now.2 Signs can be observed by the physician, such Ob/Gyns who are prepared to quickly evaluate the as leakage of urine when the patient coughs. problem and initiate effective management can Urodynamic observations are made dur- help restore the quality of life these patients ing urodynamic studies. enjoyed before onset of symptoms. This article: Overall, the new and revised terms are • reviews the pathophysiology of “overactive relatively vague to allow for patient-to-patient bladder”; variability. -

Urogenital Disorders 12
Urogenital disorders 12 In this chapter, five urogenital disorders are discussed that occur more often in patients with Sjögren's Table 12.1 Examples of causes of overactive syndrome than in the general population. These bladder symptoms disorders are: - detrusor overactivity 1. overactive bladder syndrome (overactive bladder syndrome, OAB) 2. interstitial cystitis/bladder pain syndrome - urinary tract infections 3. non-bacterial prostatitis - drugs (side-effects) 4. vulvodynia - bladder cancer; prostate cancer 5. dyspareunia - benign prostatic hyperplasia - stones in the bladder - constipation 1. Overactive bladder syndrome - pelvic organ prolapse - bladder injury Overactive bladder (OAB) syndrome is the term used to - nerve damage describe the symptom complex of urinary urgency with - neurological diseases (multiple sclerosis, or without urge incontinence, usually with frequency Parkinson’s disease, spinal cord lesions, spina and nocturia, in the absence of any sign of infection or bifida, stroke) other identifiable cause of the symptoms.36 Symptoms of overactive bladder may also have identifiable causes quality of life and patients may feel a sense of shame OAB with incontinence is currently referred to and embarrassment, in particular in OAB wet.9 as OAB wet, in contrast to OAB dry when there is no The diagnosis of OAB is based on symptoms and incontinence. does not require invasive tests. Careful questioning The symptoms of OAB are primarily due to about symptoms is important in achieving a differential involuntary contractions of the detrusor muscle during diagnosis (table 12.2). The most common differential the filling phase of the micturition cycle. These diagnosis is a urinary tract infection but in a small contractions, when observed during urodynamic number of cases bladder cancer is underlying the studies, are termed detrusor overactivity and are symptoms of OAB.