Diverticular Disease-Related Colitis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Umbilical Hernia with Cholelithiasis and Hiatal Hernia
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Springer - Publisher Connector Yamanaka et al. Surgical Case Reports (2015) 1:65 DOI 10.1186/s40792-015-0067-8 CASE REPORT Open Access Umbilical hernia with cholelithiasis and hiatal hernia: a clinical entity similar to Saint’striad Takahiro Yamanaka*, Tatsuya Miyazaki, Yuji Kumakura, Hiroaki Honjo, Keigo Hara, Takehiko Yokobori, Makoto Sakai, Makoto Sohda and Hiroyuki Kuwano Abstract We experienced two cases involving the simultaneous presence of cholelithiasis, hiatal hernia, and umbilical hernia. Both patients were female and overweight (body mass index of 25.0–29.9 kg/m2) and had a history of pregnancy and surgical treatment of cholelithiasis. Additionally, both patients had two of the three conditions of Saint’s triad. Based on analysis of the pathogenesis of these two cases, we consider that these four diseases (Saint’s triad and umbilical hernia) are associated with one another. Obesity is a common risk factor for both umbilical hernia and Saint’s triad. Female sex, older age, and a history of pregnancy are common risk factors for umbilical hernia and two of the three conditions of Saint’s triad. Thus, umbilical hernia may readily develop with Saint’s triad. Knowledge of this coincidence is important in the clinical setting. The concomitant occurrence of Saint’s triad and umbilical hernia may be another clinical “tetralogy.” Keywords: Saint’s triad; Cholelithiasis; Hiatal hernia; Umbilical hernia Background of our knowledge, no previous reports have described the Saint’s triad is characterized by the concomitant occur- coexistence of umbilical hernia with any of the three con- rence of cholelithiasis, hiatal hernia, and colonic diverticu- ditions of Saint’s triad. -

Diverticulosis Beyond the Basics.Xps
Patient education: Diverticular disease (Beyond the Basics) - UpToDate Page 1 of 10 Official reprint from UpToDate® www.uptodate.com ©2017 UpToDate® The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment. Always seek the advice of your own physician or other qualified health care professional regarding any medical questions or conditions. The use of UpToDate content is governed by the UpToDate Terms of Use. ©2017 UpToDate, Inc. All rights reserved. Patient education: Diverticular disease (Beyond the Basics) Author: John H Pemberton, MD Section Editor: J Thomas Lamont, MD Deputy Editor: Shilpa Grover, MD, MPH All topics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Dec 2016. | This topic last updated: Sep 16, 2015. DIVERTICULAR DISEASE OVERVIEW — A diverticulum is a pouch-like structure that can form through points of weakness in the muscular wall of the colon (ie, at points where blood vessels pass through the wall) (figure 1). Diverticulosis affects men and women equally. The risk of diverticular disease increases with age. It occurs throughout the world but is seen more commonly in developed countries. WHAT IS DIVERTICULAR DISEASE? Diverticulosis — Diverticulosis merely describes the presence of diverticula. Diverticulosis is often found during a test done for other reasons, such as flexible sigmoidoscopy, colonoscopy, or barium enema. Most people with diverticulosis have no symptoms and will remain symptom free for the rest of their lives. (See 'Diverticular disease prognosis' below.) A person with diverticulosis may have diverticulitis, or diverticular bleeding. -

Diverticular Abscess Presenting As a Strangulated Inguinal Hernia: Case Report and Review of the Literature
Ulster Med J 2007; 76 (2) 107-108 Presidential Address 107 Case Report Diverticular Abscess Presenting as a Strangulated Inguinal Hernia: Case Report and review of the literature. S Imran H Andrabi, Ashish Pitale*, Ahmed AS El-Hakeem Accepted 22 December 2006 ABSTRACT noted nausea, anorexia and increasing abdominal pain. She had no previous history of any surgery or trauma and was on Potentially life threatening diseases can mimic a groin hernia. warfarin for atrial fibrillation. We present an unusual case of diverticulitis with perforation and a resulting abscess presenting as a strangulated inguinal hernia. The features demonstrated were not due to strangulation of the contents of the hernia but rather pus tracking into the hernia sac from the peritoneal cavity. The patient underwent sigmoid resection and drainage of retroperitoneal and pericolonic abscesses. Radiological and laboratory studies augment in reaching a diagnosis. The differential diagnosis of inguinal swellings is discussed. Key Words: Diverticulitis, diverticular perforation, diverticular abscess, inguinal hernia INTRODUCTION The association of complicated inguinal hernia and diverticulitis is rare1. Diverticulitis can present as left iliac fossa pain, rectal bleeding, fistulas, perforation, bowel obstruction and abscesses. Our patient presented with a diverticular perforation resulting in an abscess tracking into the inguinal canal and clinically masquerading as a Fig 2. CT scan showing inflammatory changes with strangulated inguinal hernia. The management warranted an stranding of the subcutaneous fat in the left groin and a exploratory laparotomy and drainage of pus. large bowel diverticulum CASE REPORT On admission, she had a tachycardia (pulse 102 beats/min) and a temperature of 37.5OC. -

Diverticular Disease of the Colon
® ® GasTroenTerology DepArTmenT Diverticular Disease of the Colon WHAT is DiverTiculosis? Diverticulosis refers to the presence of small out-pouchings (called diverticula) or sacs that can develop in the lining of the gastrointestinal tract. While diverticula can be present anywhere in the entire digestive tract, they are most common on the left side of the large intestine, the area known as the descending and sigmoid colon (Figure 1). HoW common is DiverTiculosis? Diverticulosis is a common disorder especially in older people. The condition is rarely seen in people under the age of 30 and is most common in those over 60. Both men and women are equally affected. What cAuses DiverTiculosis? Figure 1 No one knows for certain why diverticulosis develops; however, a few theories have been suggested. Some experts believe that abnormal contraction and spasm (resulting in intermittent high pressure in the colon) may cause diverticula to form in a weak spot of the intestinal wall. Low fiber diets may play a role in the development of diverticulosis. In rural Africa where diet is high in roughage, diverticulosis is rare. There also appears to be a genetic predisposition to diverticulosis, that is, if your parent or grandparent had diverticulosis you may develop it as well. What Are the sympToms of DiverTiculosis Most patients with diverticulosis have no symptoms. Many will never know they have the condition until it is discovered during an endoscopic or radiographic (X-ray) examination. While most people have no symptoms, some individuals may experience pain or discomfort in the left lower abdomen, bloating, and/or change in bowel habits. -
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis
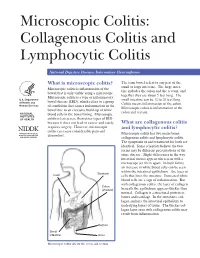
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis National Digestive Diseases Information Clearinghouse What is microscopic colitis? The term bowel refers to any part of the small or large intestine. The large intes- Microscopic colitis is inflammation of the tine includes the colon and the rectum, and bowel that is only visible using a microscope. together they are about 5 feet long. The Microscopic colitis is a type of inflammatory U.S. Department small intestine can be 12 to 20 feet long. bowel disease (IBD), which refers to a group of Health and Colitis means inflammation of the colon. Human Services of conditions that causes inflammation in the Microscopic colitis is inflammation of the bowel due to an excessive build-up of white colon and rectum. NATIONAL blood cells in the bowel lining. Microscopic INSTITUTES OF HEALTH colitis is less severe than other types of IBD because it does not lead to cancer and rarely What are collagenous colitis requires surgery. However, microscopic and lymphocytic colitis? colitis can cause considerable pain and Microscopic colitis has two main forms: discomfort. collagenous colitis and lymphocytic colitis. The symptoms of and treatment for both are identical. Some scientists believe the two forms may be different presentations of the same disease. Slight differences in the way intestinal tissues appear when seen with a microscope set them apart. In both forms, an increase in white blood cells can be seen within the intestinal epithelium—the layer of Stomach Liver cells that lines the intestine. Increased white blood cells are a sign of inflammation. But with collagenous colitis, the layer of collagen Colon (shaded) beneath the epithelium appears thicker than normal. -

Gastritides: Diagnostic Evaluation of Multifaceted Conditions
Gastritides: Diagnostic Evaluation of Multifaceted Conditions Gregory Y. Lauwers, MD Senior Member H. Lee Moffitt Cancer Center & Research Institute Tampa, FL [email protected] Changing epidemiology of gastritis (Autoimmune) (Chemical Reactive) Vieith M. Bayreuth Clinic data based on 1,333 389 cases Prevalence of Reactive Gastropathy and H. Pylori Gastritis H. Pylori Reactive Gastropathy Maguilnik I. AP&T 2012;36 • Urease activity: Biopsies (CLO-test) breath test • Serology • Stool antigen IF NEGATIVE • Sampling error -- Antibiotic monotherapy (e.g., other infections) • PPI (decreased # of bacteria; shift from antrum to prox. stomach) • Focally Enhanced Gastritis (IBD) Treated H. pylori gastritis H. Heilmannii • Low prevalence • (0.3-0.7% in devped countries) • Household pets • Mild inflammation • H. felis: • severe chronic active gastritis Autoimmune Atrophic Gastritis • Autosomal dominant inheritance • Confined to corpus and fundus • Immune – mediated injury (autoantibodies) – Loss of parietal cells – Gland atrophy – Metaplasia: pseudopyloric and intestinal types Autoimmune Gastritis SYN Treponema pallidum NK-Cell enteropathy NK-Cell enteropathy CD3 CD56 Granzyme EBV Gastritis EBV gastritis EBER Russell Body Gastritis IgG Lymphocytic gastritis •0.83% of unselected biopsies •1.7% to 4.5% of inflamed biopsies >25 IELs/ 100 epith cells (N:1-9) AJSP 1999;23. •Pan gastric:76% - Fundus:18% - Antrum:6% LYMPHOCYTIC GASTRITISCD3 • H. pylori: 30-40% [pan gastric or corpus predominant] • Celiac sprue: 26.4-38% [typically antral] • Crohn disease:1.5% • non GSE autoimmune disease: 4% • Neoplasia (gastric cancer; lymphoma):4% • Drugs (Ticlopidine, Ticlid®):1% • HIV • No clinical association in 20-28% of the cases… a seasonal tendency (fall) was noted AJSP 1999;23. Personal data: 346 cases (age range 1-87 years, mean age 51 years). -

A 51-Year-Old Man with Gastric Cancer and Lung Nodules
T h e new england journal o f medicine case records of the massachusetts general hospital Founded by Richard C. Cabot Nancy Lee Harris, m.d., Editor Eric S. Rosenberg, m.d., Associate Editor Jo-Anne O. Shepard, m.d., Associate Editor Alice M. Cort, m.d., Associate Editor Sally H. Ebeling, Assistant Editor Christine C. Peters, Assistant Editor Case 29-2007: A 51-Year-Old Man with Gastric Cancer and Lung Nodules Edward T. Ryan, M.D., Suzanne L. Aquino, M.D., and Richard L. Kradin, M.D. Presentation of Case Dr. Allison L. McDonough (Internal Medicine): A 51-year-old man with a history of From the Division of Infectious Disease gastric cancer was admitted to the hospital because of a new pulmonary lesion. (E.T.R.) and the Departments of Radiology (S.L.A.) and Pathology (R.L.K.), Massa- The patient had been in good health until approximately 5 years before admis- chusetts General Hospital; and the De- sion, when he had a decreased appetite and epigastric discomfort; evaluation at partments of Medicine (E.T.R.), Radiology another facility revealed a hiatal hernia, gastroesophageal reflux, and a duodenal (S.L.A.), and Pathology (R.L.K.), Harvard Medical School. ulcer. Testing for Helicobacter pylori was positive. Omeprazole and metoclopramide were administered, and the hiatal hernia was surgically repaired. Pain, persistent N Engl J Med 2007;357:1239-46. gastroesophageal reflux, and weight loss developed approximately 2.5 years before Copyright © 2007 Massachusetts Medical Society. admission. A primary care physician at this hospital prescribed combination therapy (lansoprazole, amoxicillin, and clarithromycin) for 2 weeks to treat the H. -

1. Pathology of the Stomach. Ileus. Vascular Diseases of the Bowels and the Peritoneum
1. Pathology of the stomach. Ileus. Vascular diseases of the bowels and the peritoneum. PATHOLOGY OF THE STOMACH Stomach mucosa • Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric glands in the antrum. • The surface mucous cells and the cardiac and pyloric glands secrete mucus which protects the stomach from self- digestion. • In fundic glands, the chief cells secrete pepsinogen; the parietal cells secrete HCl, bicarbonate, and intrinsic factor, and the endocrine cells release histamine. • Pyloric endocrine cells secrete gastrin, somatostatine, etc. Glossary • Gastritis - inflammation of the gastric mucosa associated with gastric mucosal injury • Gastropathy - epithelial cell damage and regeneration without associated inflammation • Erosion - circumscribed necrosis-induced defect of mucosa that does not cross the muscularis mucosae • Ulcer - the defect extends beyond the mucosa ACUTE GASTRITIS Pathogenesis Common condition, induced by acute damage to the gastric mucosa due to • alcohol, NSAIDs (nonsteroidal anti-inflammatory drugs, e.g., aspirin) or steroids • stress situations, e.g., severe burns, hypothermia, shock, CNS trauma, etc. • Helicobacter pylori infection Pathological features • Hemorrhagic-erosive inflammation of gastric mucosa affecting the entire stomach (pangastritis) or the antrum of stomach (antral gastritis) • Mucosal hyperemia, punctate hemorrhages, multiple erosions • + Acute ulcers: anywhere in the -

Ischaemic Colitis: Practical Challenges and Evidence-Based Recommendations For
Ischaemic Colitis: Practical Challenges and Evidence-Based Recommendations for Management Alexander Hung1*, Tom Calderbank1*, Mark A Samaan1, Andrew A Plumb2, George Webster1 Author affiliations 1Department of Gastroenterology, University College London Hospitals, London, UK 2Department of Radiology, University College London Hospitals, London, UK *Authors contributed equally Correspondence to Mark A Samaan Department of Gastroenterology University College London Hospitals 250 Euston Road London NW1 2PG [email protected] Running title Ischaemic Colitis Management Word count 3212 Key Words Ischaemic colitis, colonic ischaemia ABSTRACT Ischaemic colitis (IC) is a common condition with rising incidence and, in severe cases, a high mortality rate. Its presentation, severity and disease behaviour can vary widely and there exists significant heterogeneity in treatment strategies and resultant outcomes. In this article we explore practical challenges in the management of IC and where available, make evidence-based recommendations for its management based on a comprehensive review of available literature. An optimal approach to initial management requires early recognition of the diagnosis followed by prompt and appropriate investigation. Ideally, this should involve the input of both gastroenterology and surgery. CT with intravenous and oral contrast is the imaging modality of choice. It can support a clinical diagnosis, define the severity and distribution of ischaemia and has prognostic value. In all but fulminant cases, this should be followed (within 48 hours) by lower GI endoscopy to reach the distal-most extent of the disease, providing endoscopic (and histological) confirmation. The mainstay of medical management is conservative/supportive treatment, with bowel rest, fluid resuscitation and antibiotics. Specific laboratory, radiological and endoscopic features are recognised to correlate with more severe disease, higher rates of surgical intervention and ultimately worse outcomes. -

MANAGEMENT of ACUTE ABDOMINAL PAIN Patrick Mcgonagill, MD, FACS 4/7/21 DISCLOSURES
MANAGEMENT OF ACUTE ABDOMINAL PAIN Patrick McGonagill, MD, FACS 4/7/21 DISCLOSURES • I have no pertinent conflicts of interest to disclose OBJECTIVES • Define the pathophysiology of abdominal pain • Identify specific patterns of abdominal pain on history and physical examination that suggest common surgical problems • Explore indications for imaging and escalation of care ACKNOWLEDGEMENTS (1) HISTORICAL VIGNETTE (2) • “The general rule can be laid down that the majority of severe abdominal pains that ensue in patients who have been previously fairly well, and that last as long as six hours, are caused by conditions of surgical import.” ~Cope’s Early Diagnosis of the Acute Abdomen, 21st ed. BASIC PRINCIPLES OF THE DIAGNOSIS AND SURGICAL MANAGEMENT OF ABDOMINAL PAIN • Listen to your (and the patient’s) gut. A well honed “Spidey Sense” will get you far. • Management of intraabdominal surgical problems are time sensitive • Narcotics will not mask peritonitis • Urgent need for surgery often will depend on vitals and hemodynamics • If in doubt, reach out to your friendly neighborhood surgeon. Septic Pain Sepsis Death Shock PATHOPHYSIOLOGY OF ABDOMINAL PAIN VISCERAL PAIN • Severe distension or strong contraction of intraabdominal structure • Poorly localized • Typically occurs in the midline of the abdomen • Seems to follow an embryological pattern • Foregut – epigastrium • Midgut – periumbilical • Hindgut – suprapubic/pelvic/lower back PARIETAL/SOMATIC PAIN • Caused by direct stimulation/irritation of parietal peritoneum • Leads to localized -

Ischemic Colitis Caused by Polycythemia Vera: a Case Report and Literature Review
EXPERIMENTAL AND THERAPEUTIC MEDICINE 16: 3663-3667, 2018 Ischemic colitis caused by polycythemia vera: A case report and literature review SHASHA ZHANG1, RUIXUE LAI1, XUEQING GAO1, YUFEI ZHAO1, YUE ZHAO2, JIANHUA WU3 and ZHANJUN GUO1 Departments of 1Rheumatology and Immunology, and 2Gastroenterology and Hepatology, 3Animal Center, The Fourth Hospital of Hebei Medical University, Shijiazhuang, Hebei 050011, P.R. China Received January 16, 2018; Accepted August 10, 2018 DOI: 10.3892/etm.2018.6638 Abstract. Polycythemia vera (PV) is a chronic myeloproliferative Ischemic colitis (IC) can be described as an ischemic disease disorder originating from hematopoietic stem cells and of the colon, which results from decreased blood flow due to complicated by thrombosis and bleeding. This report describes a various causes that leads to intestinal wall ischemia, injury or case of ischemic colitis (IC) caused by PV and includes a review necrosis (3). The risk factors for IC mainly include diabetes, of the relevant literature. The patient was a 59-year-old male hypertension, dyslipidemia, peripheral vascular disease, with a history of PV who presented with abdominal pain and aspirin administration, and digoxin or constipation-inducing hematochezia. Colonoscopy and histopathological examination medications (4). The main clinical manifestations include results indicated suspected ischemic bowel disease. Following abdominal pain, diarrhea, and hematochezia (5). A reliable experimental anticoagulant therapy for 7 days, the patient no diagnosis of IC depends on the comprehensive evaluation of longer experienced abdominal pain and hematochezia had clinical symptoms, biochemical tests, radiological examina- resolved. Colonoscopy review showed no obvious anomalies tions, and endoscopic assessments (6). In certain cases, PV 1 month later. -

Colonic Ischemia 9/21/14, 9:02 PM
Colonic ischemia 9/21/14, 9:02 PM Official reprint from UpToDate® www.uptodate.com ©2014 UpToDate® Colonic ischemia Authors Section Editors Deputy Editor Peter Grubel, MD John F Eidt, MD Kathryn A Collins, MD, PhD, FACS J Thomas Lamont, MD Joseph L Mills, Sr, MD Martin Weiser, MD All topics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Aug 2014. | This topic last updated: Aug 25, 2014. INTRODUCTION — Intestinal ischemia is caused by a reduction in blood flow, which can be related to acute arterial occlusion (embolic, thrombotic), venous thrombosis, or hypoperfusion of the mesenteric vasculature causing nonocclusive ischemia. Colonic ischemia is the most frequent form of intestinal ischemia, most often affecting the elderly [1]. Approximately 15 percent of patients with colonic ischemia develop gangrene, the consequences of which can be life-threatening, making rapid diagnosis and treatment imperative. The remainder develops nongangrenous ischemia, which is usually transient and resolves without sequelae [2]. However, some of these patients will have a more prolonged course or develop long-term complications, such as stricture or chronic ischemic colitis. The diagnosis and treatment of patients can be challenging since colonic ischemia often occurs in patients who are debilitated and have multiple medical problems. The clinical features, diagnosis, and treatment of ischemia affecting the colon and rectum will be reviewed here. Acute and chronic intestinal ischemia of the small intestine are discussed separately. (See "Acute mesenteric ischemia" and "Chronic mesenteric ischemia".) BLOOD SUPPLY OF THE COLON — The circulation to the large intestine and rectum is derived from the superior mesenteric artery (SMA), inferior mesenteric artery (IMA), and internal iliac arteries (figure 1).