Acute Sigmoid Colon Diverticulitis Axial CECT Image Shows Inflamed Sigmoid Colon Diverticula with Adjacent Stranding and Edema
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Retained Fecaliths After Laparoscopic Appendectomy Disappearing Spontaneously with Non-Operative Management
IJCRI 2013;4(11):650–653. Katagiri et al. 650 www.ijcasereportsandimages.com CASE REPORT OPEN ACCESS Retained fecaliths after laparoscopic appendectomy disappearing spontaneously with non-operative management Hideki Katagiri, Mai Ishitani, Takashi Sakamoto, Yasuo Yoshinaga, Tadao Kubota, Akira Miyabe ABSTRACT ********* Introduction: Intra-abdominal abscess after doi:10.5348/ijcri-2013-11-402-CR-16 laparoscopic appendectomy is a well-known complication. In cases of perforated appendicitis, the frequency of postoperative intra-abdominal abscess formation can be up to 20%. However, intra-abdominal abscess due to retained fecaliths INTRODUCTION has rarely been reported. A retained fecalith following appendectomy is a rare complication A fecalith is often detected in cases of acute and it has been reported that retained fecaliths appendicitis. It can drop pre- or intraoperatively into the should be removed immediately after their peritoneal cavity [1]. The frequency of retained fecaliths diagnosis because of its potential to cause after appendectomy is unknown and only a few case abscess. We present a rare case of retained reports have been published [2]. Postoperative abscess fecaliths after laparoscopic appendectomy which after appendectomy is a well-known complication and, in disappeared spontaneously with non-operative cases of perforated appendicitis, the frequency can be up management. to 20% [3]. A retained fecalith can cause intra-abdominal abscess and the abscess often relapses despite adequate Keywords: Retained fecaliths, Laparoscopic drainage [4]. Previous reports recommended the removal appendectomy, Intra-abdominal abscess of complicated fecaliths after diagnosis. We present a very rare case of retained fecaliths after laparoscopic ********* appendectomy which disappeared spontaneously with non-operative management. Katagiri H, Ishitani M, Sakamoto T, Yoshinaga Y, Kubota T, Miyabe A. -

Intussusception of the Appendix: New Trends and Comprehensive Analysis of 140 Case Reports Barbara Wexelman
Yale University EliScholar – A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 7-9-2009 Intussusception of the Appendix: New trends and comprehensive analysis of 140 case reports Barbara Wexelman Follow this and additional works at: http://elischolar.library.yale.edu/ymtdl Recommended Citation Wexelman, Barbara, "Intussusception of the Appendix: New trends and comprehensive analysis of 140 case reports" (2009). Yale Medicine Thesis Digital Library. 469. http://elischolar.library.yale.edu/ymtdl/469 This Open Access Thesis is brought to you for free and open access by the School of Medicine at EliScholar – A Digital Platform for Scholarly Publishing at Yale. It has been accepted for inclusion in Yale Medicine Thesis Digital Library by an authorized administrator of EliScholar – A Digital Platform for Scholarly Publishing at Yale. For more information, please contact [email protected]. Intussusception of the Appendix: New trends and comprehensive analysis of 140 case reports A THESIS SUBMITTED TO THE YALE UNIVERSITY SCHOOL OF MEDICINE IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF MEDICINE BY BARBARA A. WEXELMAN 2008 Barbara Wexelman 1 ABSTRACT Title: INTUSSUSCEPTION OF THE APPENDIX: NEW TRENDS AND COMPREHENSIVE ANALYSIS OF 140 PUBLISHED CASE REPORTS. Barbara A. Wexelman, Cassius Ochoa Chaar, and Walter Longo. Section of Colorectal Surgery, Department of Surgery, Yale University, School of Medicine, New Haven, CT. Statement of Purpose: This paper uses 139 published case reports to understand the demographic, diagnostic, and treatment trends of intussusception of the appendix. Methods: Using the PubMed literature search engine to find all English references of “intussusception” and “appendix”, and reviewing those that contained actual case reports of intussusception of the appendix, we analyzed the demographics, presentation, diagnostic methods, surgical treatment, and histology from 140 articles representing data from 181 patients. -

Twisted Bowels: Intestinal Obstruction Blake Briggs, MD Mechanical
Twisted Bowels: Intestinal obstruction Blake Briggs, MD Objectives: define bowel obstructions and their types, pathophysiology, causes, presenting signs/symptoms, diagnosis, and treatment options, as well as the complications associated with them. Bowel Obstruction: the prevention of the normal digestive process as well as intestinal motility. 2 overarching categories: Mechanical obstruction: More common. physical blockage of the GI tract. Can be complete or incomplete. Complete obstruction typically is more severe and more likely requires surgical intervention. Functional obstruction: diffuse loss of intestinal motility and digestion throughout the intestine (e.g. failure of peristalsis). 2 possible locations: Small bowel: more common Large bowel All bowel obstructions have the potential risk of progressing to complete obstruction Mechanical obstruction Pathophysiology Mechanical blockage of flow à dilation of bowel proximal to obstruction à distal bowel is flattened/compressed à Bacteria and swallowed air add to the proximal dilation à loss of intestinal absorptive capacity and progressive loss of fluid across intestinal wall à dehydration and increasing electrolyte abnormalities à emesis with excessive loss of Na, K, H, and Cl à further dilation leads to compression of blood supply à intestinal segment ischemia and resultant necrosis. Signs/Symptoms: The goal of the physical exam in this case is to rule out signs of peritonitis (e.g. ruptured bowel). Colicky abdominal pain Bloating and distention: distention is worse in distal bowel obstruction. Hyperresonance on percussion. Nausea and vomiting: N/V is worse in proximal obstruction. Excessive emesis leads to hyponatremic, hypochloremic metabolic alkalosis with hypokalemia. Dehydration from emesis and fluid shifts results in dry mucus membranes and oliguria Obstipation: severe constipation or complete lack of bowel movements. -

Diverticular Abscess Presenting As a Strangulated Inguinal Hernia: Case Report and Review of the Literature
Ulster Med J 2007; 76 (2) 107-108 Presidential Address 107 Case Report Diverticular Abscess Presenting as a Strangulated Inguinal Hernia: Case Report and review of the literature. S Imran H Andrabi, Ashish Pitale*, Ahmed AS El-Hakeem Accepted 22 December 2006 ABSTRACT noted nausea, anorexia and increasing abdominal pain. She had no previous history of any surgery or trauma and was on Potentially life threatening diseases can mimic a groin hernia. warfarin for atrial fibrillation. We present an unusual case of diverticulitis with perforation and a resulting abscess presenting as a strangulated inguinal hernia. The features demonstrated were not due to strangulation of the contents of the hernia but rather pus tracking into the hernia sac from the peritoneal cavity. The patient underwent sigmoid resection and drainage of retroperitoneal and pericolonic abscesses. Radiological and laboratory studies augment in reaching a diagnosis. The differential diagnosis of inguinal swellings is discussed. Key Words: Diverticulitis, diverticular perforation, diverticular abscess, inguinal hernia INTRODUCTION The association of complicated inguinal hernia and diverticulitis is rare1. Diverticulitis can present as left iliac fossa pain, rectal bleeding, fistulas, perforation, bowel obstruction and abscesses. Our patient presented with a diverticular perforation resulting in an abscess tracking into the inguinal canal and clinically masquerading as a Fig 2. CT scan showing inflammatory changes with strangulated inguinal hernia. The management warranted an stranding of the subcutaneous fat in the left groin and a exploratory laparotomy and drainage of pus. large bowel diverticulum CASE REPORT On admission, she had a tachycardia (pulse 102 beats/min) and a temperature of 37.5OC. -

Delayed Presentation of a Retained Fecalith
Open Access Case Report DOI: 10.7759/cureus.15919 Delayed Presentation of a Retained Fecalith Fawwad A. Ansari 1 , Muhammad Ibraiz Bilal 1 , Muhammad Umer Riaz Gondal 1 , Mehwish Latif 2 , Nadeem Iqbal 2 1. Medicine, Shifa International Hospital, Islamabad, PAK 2. Gastroenterology, Shifa International Hospital, Islamabad, PAK Corresponding author: Fawwad A. Ansari, [email protected] Abstract A fecalith is a common cause of acute appendicitis, and laparoscopic surgery is the mainstay of its management. Literature review shows that a fecalith may be retained in the gut following a laparoscopic appendectomy in some rare cases. In most cases, the fecalith becomes symptomatic with time due to the formation of an abscess, fistulous tract, or inflammation of the appendicular stump (stump appendicitis). We report a case of retained appendicular fecalith presenting with symptoms similar to acute appendicitis, 15 years after laparoscopic appendectomy. Categories: Gastroenterology, General Surgery Keywords: colonoscopy, acute appendicitis, appendectomy, fecalith, right iliac fossa pain, complications Introduction A fecalith is a hard stony mass of feces in the intestinal tract. Fecal impaction occurs when a large amount of fecal matter gets compacted and cannot get evacuated spontaneously [1]. In its extreme form, fecal impaction can lead to the formation of a fecalith due to the hardening of fecal material that forms a mass separate from other bowel contents [2]. It can occur in any part of the intestine [1]. Most often, a fecalith arises in the colon (mostly sigmoid) or rectum and very rarely in the small intestine [2]. Here we present a case of a retained appendicular fecalith in a patient who presented with an acute abdomen. -

Clinical Acute Abdominal Pain in Children
Clinical Acute Abdominal Pain in Children Urgent message: This article will guide you through the differential diagnosis, management and disposition of pediatric patients present- ing with acute abdominal pain. KAYLEENE E. PAGÁN CORREA, MD, FAAP Introduction y tummy hurts.” That is a simple statement that shows a common complaint from children who seek “M 1 care in an urgent care or emergency department. But the diagnosis in such patients can be challenging for a clinician because of the diverse etiologies. Acute abdominal pain is commonly caused by self-limiting con- ditions but also may herald serious medical or surgical emergencies, such as appendicitis. Making a timely diag- nosis is important to reduce the rate of complications but it can be challenging, particularly in infants and young children. Excellent history-taking skills accompanied by a careful, thorough physical exam are key to making the diagnosis or at least making a reasonable conclusion about a patient’s care.2 This article discusses the differential diagnosis for acute abdominal pain in children and offers guidance for initial evaluation and management of pediatric patients presenting with this complaint. © Getty Images Contrary to visceral pain, somatoparietal pain is well Pathophysiology localized, intense (sharp), and associated with one side Abdominal pain localization is confounded by the or the other because the nerves associated are numerous, nature of the pain receptors involved and may be clas- myelinated and transmit to a specific dorsal root ganglia. sified as visceral, somatoparietal, or referred pain. Vis- Somatoparietal pain receptors are principally located in ceral pain is not well localized because the afferent the parietal peritoneum, muscle and skin and usually nerves have fewer endings in the gut, are not myeli- respond to stretching, tearing or inflammation. -

Abdominal Pain
10 Abdominal Pain Adrian Miranda Acute abdominal pain is usually a self-limiting, benign condition that irritation, and lateralizes to one of four quadrants. Because of the is commonly caused by gastroenteritis, constipation, or a viral illness. relative localization of the noxious stimulation to the underlying The challenge is to identify children who require immediate evaluation peritoneum and the more anatomically specific and unilateral inner- for potentially life-threatening conditions. Chronic abdominal pain is vation (peripheral-nonautonomic nerves) of the peritoneum, it is also a common complaint in pediatric practices, as it comprises 2-4% usually easier to identify the precise anatomic location that is produc- of pediatric visits. At least 20% of children seek attention for chronic ing parietal pain (Fig. 10.2). abdominal pain by the age of 15 years. Up to 28% of children complain of abdominal pain at least once per week and only 2% seek medical ACUTE ABDOMINAL PAIN attention. The primary care physician, pediatrician, emergency physi- cian, and surgeon must be able to distinguish serious and potentially The clinician evaluating the child with abdominal pain of acute onset life-threatening diseases from more benign problems (Table 10.1). must decide quickly whether the child has a “surgical abdomen” (a Abdominal pain may be a single acute event (Tables 10.2 and 10.3), a serious medical problem necessitating treatment and admission to the recurring acute problem (as in abdominal migraine), or a chronic hospital) or a process that can be managed on an outpatient basis. problem (Table 10.4). The differential diagnosis is lengthy, differs from Even though surgical diagnoses are fewer than 10% of all causes of that in adults, and varies by age group. -

Amyand's Hernia: Report of Two Cases and a Review
CASE REPORT Hastal›klar› Dergisi &Journal of Diseases of the Colon and Rectum Amyand’s Hernia: Report of Two Cases and a Review of the Literature Amyand F›t›¤›nda ‹ki Olgu ve Literatürün Gözden Geçirilmesi ÜMRAN MUSLU, ÖMER ARDA ÇET‹NKAYA T.C. Sa¤l›k Bakanl›¤› Alaca Devlet Hastanesi, Genel Cerrahi Bölümü, Alaca, Çorum-Türkiye ÖZET ABSTRACT Amyand f›t›¤› adland›rmas› inguinal f›t›k kesesi içerisinde The designation “Amyand’s” in association with a hernia rüptüre appendiks vermiformisi tan›mlamak için Claudius is used for Amyand's name to any hernia was used for Amyand ilk kez appendektomiyi uygulad›¤›nda a ruptured appendix found in an inguinal hernia sac kullan›lmaktayd›. Daha sonralar›, inguinal f›t›k keseleri based on the recognition that Claudius Amyand was the içerisinde inflame olsun ya da olmas›n appendiks first to perform an appendectomy. Recently, inguinal vermiformis bulunmas› durumuna Amyand f›t›¤› hernias containing the appendix,both inflamed and not, denilmeye bafllanm›flt›r. F›t›k defektinin kontamine have been called Amyand hernia. Roughly only 0.1% alanlarda sentetik veya biyosentetik yamalar ile onar›m› of inguinal hernias contain an inflamed appendix. The halen tart›flmal›d›r. Sa¤laml›k, esneklik, konuk doku repair of such defects with mesh grafts is still debatable kompatibilitesi ve enfeksiyonlardan korunma yetene¤i due to unresolved suspicion of contamination. Strength, ideal bir yaman›n tan›m› olmal›d›r. Pek çok sentetik ve flexibility, host tissue compatibility and ability to avoid biyolojik yama dokusu tüm dünyada kullan›lmas›na infections should characterize an ideal mesh. -

MANAGEMENT of ACUTE ABDOMINAL PAIN Patrick Mcgonagill, MD, FACS 4/7/21 DISCLOSURES
MANAGEMENT OF ACUTE ABDOMINAL PAIN Patrick McGonagill, MD, FACS 4/7/21 DISCLOSURES • I have no pertinent conflicts of interest to disclose OBJECTIVES • Define the pathophysiology of abdominal pain • Identify specific patterns of abdominal pain on history and physical examination that suggest common surgical problems • Explore indications for imaging and escalation of care ACKNOWLEDGEMENTS (1) HISTORICAL VIGNETTE (2) • “The general rule can be laid down that the majority of severe abdominal pains that ensue in patients who have been previously fairly well, and that last as long as six hours, are caused by conditions of surgical import.” ~Cope’s Early Diagnosis of the Acute Abdomen, 21st ed. BASIC PRINCIPLES OF THE DIAGNOSIS AND SURGICAL MANAGEMENT OF ABDOMINAL PAIN • Listen to your (and the patient’s) gut. A well honed “Spidey Sense” will get you far. • Management of intraabdominal surgical problems are time sensitive • Narcotics will not mask peritonitis • Urgent need for surgery often will depend on vitals and hemodynamics • If in doubt, reach out to your friendly neighborhood surgeon. Septic Pain Sepsis Death Shock PATHOPHYSIOLOGY OF ABDOMINAL PAIN VISCERAL PAIN • Severe distension or strong contraction of intraabdominal structure • Poorly localized • Typically occurs in the midline of the abdomen • Seems to follow an embryological pattern • Foregut – epigastrium • Midgut – periumbilical • Hindgut – suprapubic/pelvic/lower back PARIETAL/SOMATIC PAIN • Caused by direct stimulation/irritation of parietal peritoneum • Leads to localized -

Problems in Family Practice Acute Abdominal Pain in Children
dysuria. The older child may start bed wetting with or without dysuria. A problems in Family Practice drop of fresh, clean unspun urine will usually reveal pyuria, but in the early case relatively few white blood cells may be seen compared to gross bacillu- Acute Abdominal Pain ria. The infection may have underlying urinary tract abnormality, stone, in Children hydronephrosis, polycystic kidney or renal neoplasms. The IVP is important Hyman Shrand, M D in detecting these underlying prob lems. Cambridge, M assachusetts 4. Viral Hepatitis. Malaise, anorexia, abdominal pain, and tenderness over Acute abdominal pain in children is a common and challenging prob the liver occur with hepatitis A or B. lem for the family physician. The many causes of this problem require Later, patients who become jaundiced a systematic approach to making the diagnosis and planning specific have dark urine and pale stools. In therapy. A careful history and physical examination, together with a teenagers, “needle tracks” suggest sy ringe transmitted Type B (H.A.A.) small number of selected laboratory studies, provide a rational basis hepatitis. Youngsters with infectious for effective management in most cases. This paper reviews the more mononucleosis may present as hepati common causes of acute abdominal pain in children with special em tis. phasis on their clinical differentiation. 5. Upper Respiratory Tract. Strepto coccal pharyngitis, a common cause of Abdominal pain in a child is always followed by vomiting is more likely an vomiting and abdominal pain, can be an emergency. The primary physician intra-abdominal disorder. recognized by looking at the throat must identify a “medical” cause in or with confirmatory throat culture. -
Diverticulitis of the Appendix
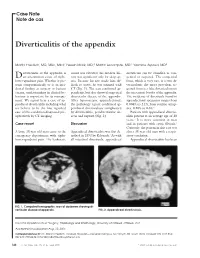
Case Note Note de cas Diverticulitis of the appendix Martin Friedlich, MD, MSc, MEd;* Neesh Malik, MD;† Martin Lecompte, MD;† Yasmine Ayroud, MD‡ iverticulitis of the appendix is count was elevated; his medical his- diverticula can be classified as con- Dan uncommon cause of right- tory was significant only for sleep ap- genital or acquired. The congenital lower-quadrant pain. Whether it pre- nea. Because his size made him dif- form, which is very rare, is a true di- sents symptomatically or is an inci- ficult to assess, he was scanned with verticulum; the more prevalent ac- dental finding at surgery or barium CT (Fig. 1). The scan confirmed ap- quired form is a false diverticulum on enema, understanding its clinical be- pendicitis, but also showed suspected the mesenteric border of the appendix. haviour is important for its manage- diverticular disease of the appendix. The incidence of diverticula found in ment. We report here a case of ap- After laparoscopic appendectomy, appendectomy specimens ranges from pendiceal diverticulitis including what the pathology report confirmed ap- 0.004% to 2.1%; from routine autop- we believe to be the first reported pendiceal diverticulosis complicated sies, 0.20% to 0.6%.2 case of this condition diagnosed pre- by diverticulitis, peridiverticular ab- Patients with appendiceal divertic- operatively by CT imaging. scess and rupture (Fig. 2). ulitis present at an average age of 38 years.3 It is more common in men Case report Discussion and in patients with cystic fibrosis.2 Curiously, the patient in this case was A large 38-year-old man came to the Appendiceal diverticulitis was first de- also a 38-year-old man with a respir- emergency department with right- scribed in 1893 by Kelynack.1 As with atory condition. -
Colonic Gallstone Obstruction
Advances in Clinical Medical Research and Healthcare Delivery Volume 1 Issue 1 Inaugural Issue Article 4 2021 Colonic Gallstone Obstruction Abdoulaziz Toure M.D Arnot Ogden Medical Center, [email protected] Mitchell Witkowski LECOM, [email protected] Vithal Vernenkar D.O Newark Wayne Community Hospital, [email protected] Brian Watkins MD, MS, FACS Newark Wayne Community Hospital, [email protected] Prasad V. Penmetsa M.D Rochester General Hospital, [email protected] Follow this and additional works at: https://scholar.rochesterregional.org/advances Part of the Health and Medical Administration Commons, Medical Education Commons, and the Medical Specialties Commons Recommended Citation Toure A, Witkowski M, Vernenkar V, Watkins B, Penmetsa PV. Colonic Gallstone Obstruction. Advances in Clinical Medical Research and Healthcare Delivery. 2021; 1(1). doi: 10.53785/2769-2779.1005. This Article is brought to you for free and open access by RocScholar. It has been accepted for inclusion in Advances in Clinical Medical Research and Healthcare Delivery by an authorized editor of RocScholar. ISSN: 2769-2779 Colonic Gallstone Obstruction Abstract This report discusses a case of a 79-year-old Caucasian female who presented with large bowel obstruction. A significant TC findings of cholecystocolic fistula and an impacted gallstone at the junction of the descending and sigmoid colon. We present a case of colonic gallstone obstruction that was treated with endoscopic lithotripsy. This interventional approach is effective in stable elderly patients with high surgical risk and in patients with significant comorbidities. Keywords gallstone complication, Cholecystocolic fistula, colonic gallstones, large bowel gallstones, gallstone ileus This article is available in Advances in Clinical Medical Research and Healthcare Delivery: https://scholar.rochesterregional.org/advances/vol1/iss1/4 Toure et al.: Colonic Gallstone Obstruction Background Gallstone ileus is a rare complication of cholelithiasis.