Inter-District Variation in Health Services in Uttar Pardesh
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

List of Examination Centres for Even Semester Exam 2011 – 12 (MAY-2012) Sr
List of Examination Centres For Even Semester Exam 2011 – 12 (MAY-2012) Sr. Code, Name and Address of List of Institutions whose student shall appear at the examination Code of Nodal Centre No. Examination Centres Centres for Theory Examination to which examination centre is attached 1 2 3 4 5 1 (001) Anand Engineering 1. (002) Faculty Of Engineering & Technology, Agra B. Tech 001 Agra College, Agra College, Agra 2. (006) Agra Public Institute Of Technology & B.Phar Computer Education (Deptt. Of Pharmacy), Agra 3. (243) College Of Pharmacy Agra, Agra B.Phar 4. (314) Sai Nath College Of Pharmacy,Agra B.Phar 5. (617) Uttam Institute Of Management Studies,Agra MBA 6. (659) Heritage Institute Of Hotel & Tourism,Agra BHMCT 2 (003)Babu Mohan Lal Arya 1. (004) R.B.S.College, Faculty Of Engg.& B.Tech 001 Agra Smarak Engg. College, Agra Technology,Agra Agra 2. (278) Aryan Institute Of Management And Computer MBA Studies,Agra 3. (338) K. P. Engineering College ,Agra B.Tech, MBA 4. (436) K. P. College Of Management,Agra MBA 3. (004) R.B.S.College, Faculty Of 1. (001) Anand Engineering College, Agra B.Tech, 001 Agra Engg. & Technology,Agra MBA,MCA 4. (005) Raja Balwant Singh 1. (003) Babu Mohan Lal Arya Smarak Engg. College, B.Tech, MBA 001 Agra College,Agra Agra 5. (064) Hindustan College Of 1. (317) Dhanwantri Institute Of Pharmacy,Mathura B.Phar 001 Agra Science & Technology, Mathura 2. (366) Nikhil Institute Of Engineering & B.Tech, MBA Management,Mathura 3. (394) College Of Business Studies,Agra MBA 4. -

Regional Office - U.P
Regional Office - U.P. Pollution Control Board, Ghaziabad S.No. Name And Address Of The Products Hazardous HW Generating Streams HW Generation In Total Quantity Of HW In MTA (10) Remark Unit Manufactured In Waste (HW) As Per MTA As Per Quantity Of MTA Generating HW Process As Sch. 1 Sch. 2 Sch. 1 Sch. 2 Generation Landfillable Recyclable Incinerable Per Schedule In MTA 1 1 2 3 4 5 6 7 8 9=7+810 11 Closed Unit 1 BHAGWATI PHOSPH&ELEC 12 12.5 0.9 0.9 0.9000 0.0000 0.0000 SELF ENTERPRISES, PL(Ni&Cr) CLOSED S-28, SITE-4, SBD JOB WORK BASIS 2 F.M. PARTS & BREAK DISC 15 15.3 0 0 0.0000 0.0000 0.0000 SELF COMPONENT (P0 LTD, 31 CLOSED A LONI RD I.A. MOHAN NGR. 3 REINZ TALBROS LTD. , GASKET 15 15.3 0 0 0.0000 0.0000 0.0000 CLOSED 19,LONI Rd.MOHAN NGR JOINTING 4 GOOD LUCK INDUSTRY, H.F. ACID 17 17.1 120 120 120.0000 0.0000 0.0000 SELF CLOED 122, A.I.A., MOHAN NGR. 10 MT/D OWN REASONS 5 PANKAJ CHEMICALS, 80, H.F. ACID 17 17.1 0 0 0.0000 0.0000 0.0000 CLOSED R.I.A., MOHAN NGR., 6 ARISTRO PRINTERS P PRINTING OF 21 21.1 0.6 0.6 0.0000 0.0000 0.6000 SELF LTD., E-64, S.S. OF G.T. PAPERS CLOSED ROAD. 7 ASIA CHEMICAL, G.T. PAINTS & 21 21.1 6 6 0.0000 6.0000 0.0000 SELF ROAD, VARNISH CLSOED 8 ADDI INDUSTRIES, C-227, FABRIC 24 24.2 6 6 6.0000 0.0000 0.0000 SELF B.S. -
S. No. Name & Address of Unit Regional Office Status of Authorisati
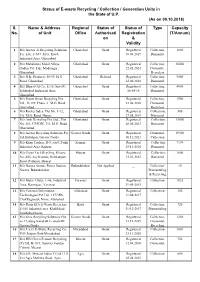
Status of E-waste Recycling / Collection / Generation Units in the State of U.P. (As on 09.10.2018) S. Name & Address Regional Status of Status of Type Capacity No. of Unit Office Authorisati Registration (T/Annum) on & Validity 1 M/s Auctus -E Recycling Solutions Ghaziabad Grant Registered Collection, 1800 Pvt. Ltd., F-637, M.G. Road, 30.08.2019 Dismantle Industrial Area, Ghaziabad. 2 M/s Mahaluxmi Metal Alloys Ghaziabad Grant Registered Collection, 30000 (India) Pvt. Ltd., Modinagar, 22.05.2023 Dismantle, Ghaziabad. Recyclers 3 M/s N.K. Products, 58-59, M.G. Ghaziabad Refused Registered Collection, 9000 Road, Ghaziabad. 22.06.2016 Dismental 4 M/s Bharat Oil Co., E-18, Site-IV, Ghaziabad Grant Registered Collection, 4000 Sahibabad, Industrial Area, 16-05-18 Dismental Ghaziabad. 5 M/s Planet Green Recycling Pvt. Ghaziabad Grant Registered Collection, 1500 Ltd., G-129, Phase -1, M.G. Road, 23.08.2018 Dismental, Ghaziabad. Recyclers 6 M/s Rocket Sales, Plot No. 1-12, Ghaziabad Grant Registered Collection,, 300 I/A, M.G. Raod, Hapur. 27.08.2019 Dismental 7 M/s Arsh Recycling Pvt. Ltd., Plot Ghaziabad Grant Registered Collection, 15000 No. 203, UPSDIC, I/A, M.G. Road, 20.06.2023 Dismental Ghaziabad. 8 M/s Auctus Recycling Solutions Pvt. Greater Noida Grant Registered Dismental, 19500 Ltd.Habibpur, Greater Noida. 06.12.2021 Callection 9 M/s Khan Traders, B-5, site4, Panki Kanpur Grant Registered Collection, 7190 Industrial Area, Kanpur. 15-11-2020 Dismental 10 M/s Green Tech Rcycling, Khasra Meerut Grant Registered Collection, 1800 No.-645, Acchraunds, Bahdaurpur 12.01.2022 Dismental Road, Partapur, Meerut . -
Sanctioned Map List Zone-6
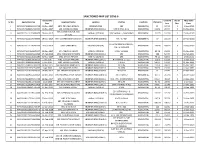
SANCTIONED MAP LIST ZONE-6 Sanctioned Covered No Of Map Valid Sr No Application No Applicant Name Location Plot No Land Use Plot Area Date Area Floor Upto 1 MAP20171109121911720 10-Nov-2017 MRS. PRIYANKA MONGA INDIRAPURAM 389 RESIDENTIAL 90 197.15 3 9-Nov-2022 2 MAP20171109142426703 13-Nov-2017 MR. ARVIND SHARMA INDIRAPURAM (ZONE-6) NITI KHAND -2/ 62 RESIDENTIAL 111.56 257.73 3 14-Nov-2022 MR. SHASHANK JAIN AND 3 MAP20171111125606300 20-Nov-2017 VAISHALI (ZONE-6) 9/8, VAISHALI , GHAZIABAD RESIDENTIAL 194.75 512.56 3 19-Nov-2022 OTHERS 4 MAP20171111175043893 18-Nov-2017 MR. GOVIND SINGH BANGARI INDIRAPURAM (ZONE-6) N.K..-3 / 584 RESIDENTIAL 87 201.03 3 19-Nov-2022 IIC-62 ASHIRWAD VAISHALI, 5 MAP20171114105744423 14-Nov-2017 MRS. VEENA RANI VAISHALI (ZONE-6) RESIDENTIAL 156.98 308.94 3 13-Nov-2022 HIG , GHAZIABAD 6 MAP20171114160841207 15-Nov-2017 MR. ASHWANI KUMAR VAISHALI (ZONE-6) 1-252, VAISHALI RESIDENTIAL 89.18 216.22 3 15-Nov-2022 7 MAP20171122125126890 17-Feb-2018 MRS. RAJKUMAR MADWAL INDIRAPURAM (ZONE-6) 242 RESIDENTIAL 200 524.55 3 19-Feb-2023 8 MAP20171123204400483 30-Nov-2017 MRS. SHASHI PRABHA VAISHALI (ZONE-6) 499 RESIDENTIAL 79.43 189.65 3 2-Dec-2022 9 MAP20171201160626023 5-Dec-2017 MRS. SUDESH MADDAN INDIRAPURAM (ZONE-6) NITI KHAND -2 / 135 RESIDENTIAL 259.1 622.09 3 6-Dec-2022 10 MAP20171201193526043 6-Dec-2017 MRS. ZARINA KHATOON VAISHALI (ZONE-6) III-A/253 RESIDENTIAL 146.23 178.32 3 21-Dec-2022 11 MAP20171209151908113 15-Dec-2017 MR. -

Quarantine Centres in Uttar Pradesh
Quarantine Centres in Uttar Pradesh Contact Name of Room Contact Person(Go Hotel/ Rate(including Person vt. Sl. Quarantin meals and (Hotel/Ce Contact official in No. District Type: e Centre: Email Phone taxes) ntre) Number Charge) Contact no. Remarks 1 GAUTAM On YMCA 8287773820 Category 1:0 YMCA 8287773820 Central AC are BUDDHA Payment Centralize Category 2:0 Centralize not permitted NAGAR d) Category d) 3:Single: 1500/- Double: 2000/- 2 GHAZIABAD On Yes Guest Category Yes Guest 0 P N Dixit 8858784527 Contact details Payment House 1:2000 House not available 3 GHAZIABAD On World Category World 0 P N Dixit 8858784527 Contact details Payment Square 1:3000 Square not available Hotel Hotel 4 LUCKNOW On VGS Category 1:0 VGS 0 Payment Category 2:0 Category 3:Single: 999.00 Double: 1400.00 5 GHAZIABAD On Vatsal Category Vatsal 0 P N Dixit 8858784527 Contact details Payment Hotel 1:1000 Hotel not available 6 GHAZIABAD On Vaishnav Category Vaishnav 0 P N Dixit 8858784527 Contact details Payment Hotel 1:3000 Hotel not available 7 LUCKNOW On Tusharth Category 1:0 Tusharth 0 Payment Inn Inn 7 LUCKNOW On Tusharth Tusharth 0 Payment Inn Category 2:0 Inn Category 3:Single: 999.00 Double: 1400.00 8 GAUTAM On Treebo 9810532571 Category 1:0 Treebo 9810532571 BUDDHA Payment Swag18 Category 2:0 Swag18 NAGAR window Category window & 3:Single: & split) 1500/- split) Double: 2000/- 9 GHAZIABAD On The Category The 0 P N Dixit 8858784527 Contact details Payment Grand 1:2000 Grand not available Place Place 10 LUCKNOW On The Category 1:0 The 0 Payment Golden -
Meerut Zone, Opposite Ccs University, Mangal Pandey Nagar, Meerut
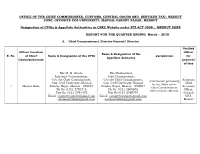
OFFICE OF THE CHIEF COMMISSIONER, CUSTOMS, CENTRAL GOODS AND SERVICES TAX:: MEERUT ZONE, OPPOSITE CCS UNIVERSITY, MANGAL PANDEY NAGAR, MEERUT Designation of CPIOs & Appellate Authorities in CBEC Website under RTI ACT 2005 :: MEERUT ZONE REPORT FOR THE QUARTER ENDING March – 2018 A. Chief Commissioner/ Director General/ Director Notified Office/ Location Officer Name & Designation of the S. No. of Chief Name & Designation of the CPIO Jurisdiction for Appellate Authority Commissionerate payment of fees Shri R. K. Gupta, Shri Roshan Lal, Assistant Commissioner, Joint Commissioner O/o the Chief Commissioner, O/o the Chief Commissioner, Assistant Information pertaining Opp. CCS University, Mangal Opp. CCS University, Mangal Chief to the Office of the 1 Meerut Zone Pandey Nagar, Meerut - 250004 Pandey Nagar, Meerut - 250004 Accounts Chief Commissioner, Ph No: 0121-2792745 Ph No: 0121-2600605 Officer, Meerut Zone, Meerut. Fax No: 0121-2761472 Fax No:0121-2769707 Central Email: [email protected] Email: [email protected] GST, [email protected] [email protected] Meerut B. Commissioner/ Addl. Director General Notified S. Commission Name & Designation of the officer for Name & Designation of the CPIO Jurisdiction No. erate Appellate Authority payment of fees Areas falling Shri Kamlesh Singh Shri Roshan Lal Joint Commissioner under the Assistant Chief Assistant Commissioner Districts of Accounts O/o the Commissioner, Office of the Commissioner of Central Meerut, Officer, Office Central GST Commissionerate Goods & Services Tax, Baghpat, of the Central GST Meerut, Opp. CCS University, Commissionerate: Meerut, Opposite: Muzaffarnagar, Commissioner Meerut Mangal Pandey Nagar, Meerut. Saharanpur, 1 Chaudhary Charan Singh University, of Central Commissione Fax No: 0121-2792773 Shamli, Goods & Mangal Pandey Nagar, Meerut- rate Amroha, Services Tax, 250004 Moradabad, Commissionera Bijnore and te: Meerut Ph No: 0121-2600605 Rampur in the Fax No:0121-2769707 State of Uttar Pradesh. -
U.P.S.R.T.C. Time Table of Volvo & Scania Services (UP DATED up TO
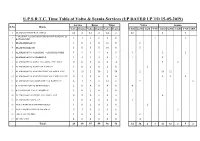
U.P.S.R.T.C. Time Table of Volvo & Scania Services (UP DATED UP TO 15-05-2019) Service Buses Trips Volvo Scania S.No Route Volvo Scania Volvo Scania Volvo Scania LKO GZB AGR VNS LKO GZB AGR VNS SRE 1 ALAMBAGH TO PRAYAGRAJ 12 2 12 2 24 4 12 2 0 VARANASI-AZAMGARH-GORAKHAPUR-SONAULI- 2 1 1 1 1 2 2 1 1 KATHMANDU 3 DELHI-DEHRADUN 8 0 8 0 16 0 8 4 DELHI-RISHIKESH 5 0 5 0 10 0 5 5 ALAMBAGH TO VARANASI VIA PRATAPGARH 3 4 3 4 6 8 3 2 2 6 ALAMBAGH TO GORAKHPUR 1 2 1 2 2 4 1 2 7 ALAMBAGH TO AGRA VIA AGRA EXP. WAY 0 6 0 6 0 12 4 2 8 ALAMBAGH TO AGAR VIA KANPUR 1 0 2 0 2 0 2 9 ALAMBAGH TO ANAND VIHAR VIA AGRA EXP 1 15 2 30 2 30 2 18 12 10 ALAMBAGH TO ANAND VIHAR VIA YAMUNA EXP. 0 3 0 6 0 6 2 2 2 11 ALAMBAGH TO KAUSHAMBI VIA BAREILLY 6 1 7 2 12 2 7 2 12 KAISHARBAGH TO DEHRADOON 2 0 4 0 4 0 4 13 KAISARBAGH TO KATHGODAM 1 0 2 0 2 0 2 14 ALAMBAGH TO JAIPUR VIA AGRA EXP 0 2 0 4 0 4 4 15 ALAMBAGH TO BALLIA 1 0 2 0 2 0 2 16 AGRA-HARIDWAR-DEHERADOON 1 0 2 0 2 0 2 17 AGRA-NOIDA-SARAI KALE KHAN 0 3 0 2 0 6 2 18 DELHI-RUPAIDIHA 1 0 2 0 2 0 2 19 DELHI-AGRA 4 0 4 0 8 0 4 Total 48 39 57 59 96 78 24 28 4 1 34 14 4 5 2 1 Up - ALAMBAGH TO PRAYAGRAJ SL. -

District Baghpt
BASE LINE SURVEY IN THE MINORITY CONCENTRATED DISTRICTS OF UTTAR PRADESH (A Report of Baghpat District) Sponsored by: Ministry of Minority Affairs Government of India New Delhi Study conducted by: Dr. R. C. TYAGI GIRI INSTITUTE OF DEVELOPMENT STUDIES SECTOR-O, ALIGANJ HOUSING SCHEME LUCKNOW-226 024 CONTENTS Title Page No DISTRICT MAP – BAGHPAT vi EXECUTIVE SUMMARY vii-xi CHAPTER I: OUTLINE OF THE STUDY 1 -3 1.1 About the study 1 1.2 Objective of the study 2 1.3 Methodology and Sample design 2 1.4 Tools 3 CHAPTER II: DEVELOPMENT STATUS IN BAGHPAT DISTRICT 4-18 2.1 Introduction 4 2.2 Demographic Status 6 2.3 Demographic Status by Religion 6 2. 4 Structure and Growth in Employment 7 2.5 Unemployment 8 2.6 Land Use Pattern 9 2.7 Coverage of Irrigation and Sources 9 2.8 Productivity of Major Crops 10 2.9 Livestock 10 2.10 Industrial Development 11 2.11 Development of Economic Infrastructure 12 2.12 Rural Infrastructure 13 2.13 Educational Infrastructure 13 2.14 Health Infrastructure 14 2.15 Housing Amenities in Baghpat District 15 2.16 Sources of Drinking Water 16 2.17 Sources of Cooking Fuel 17 2.18 Income and Poverty Level 18 CHAPTER III: DEVELOPMENT STATUS AT THE VILLAGE LEVEL 19-31 3.1 Population 19 3.2 Occupational Pattern 19 3.3 Land use Pattern 20 3.4 Sources of Irrigation 20 3.5 Roads and Electricity 21 3.6 Drinking Water 22 3.7 Toilet Facility 22 3.8 Educational Facility 22 3.9 Students Enrollments 23 3.10 Physical Structure of Schools 23 3.11 Private Schools and Preferences of the People for Schools 24 3.12 Health Facility 25 3.13 -
S.No. Districts Pin Code 1 Ghaziabad 201010 2
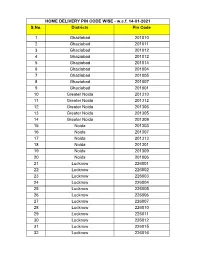
HOME DELIVERY PIN CODE WISE - w.e.f. 14-01-2021 S.No. Districts Pin Code 1 Ghaziabad 201010 2 Ghaziabad 201011 3 Ghaziabad 201012 4 Ghaziabad 201012 5 Ghaziabad 201014 6 Ghaziabad 201004 7 Ghaziabad 201005 8 Ghaziabad 201007 9 Ghaziabad 201001 10 Greater Noida 201310 11 Greater Noida 201312 12 Greater Noida 201306 13 Greater Noida 201305 14 Greater Noida 201309 15 Noida 201303 16 Noida 201307 17 Noida 201313 18 Noida 201301 19 Noida 201309 20 Noida 201006 21 Lucknow 226001 22 Lucknow 226002 23 Lucknow 226003 24 Lucknow 226004 25 Lucknow 226005 26 Lucknow 226006 27 Lucknow 226007 28 Lucknow 226010 29 Lucknow 226011 30 Lucknow 226012 31 Lucknow 226015 32 Lucknow 226016 33 Lucknow 226018 34 Lucknow 226020 35 Lucknow 226022 36 Lucknow 226024 HOME DELIVERY PIN CODE WISE - w.e.f. 14-01-2021 S.No. Districts Pin Code 37 Meerut 250001 38 Meerut 250001 39 Meerut 250002 40 Meerut 250003 41 Meerut 250004 42 Meerut 250005 43 Meerut 250103 44 Meerut 250104 45 Meerut 250110 46 Meerut 250205 47 Agra 282007 48 Agra 282001 49 Agra 282002 50 Agra 282003 51 Agra 282004 52 Agra 282005 53 Agra 282006 54 Agra 282007 55 Agra 282008 56 Agra 282009 57 Agra 282010 58 Varanasi 231304 59 Varanasi 221001 60 Varanasi 221002 61 Varanasi 221003 62 Varanasi 221004 63 Varanasi 221005 64 Varanasi 221006 65 Varanasi 221007 66 Varanasi 221008 67 Varanasi 221010 68 Varanasi 221011 69 Varanasi 221101 70 Varanasi 221103 71 Varanasi 221104 72 Varanasi 221105 73 Varanasi 221106 74 Varanasi 221107 75 Varanasi 221108 76 Varanasi 221110 77 Varanasi 221112 78 Varanasi 221115 79 Varanasi -
S.NO Code ADDRESS Area City
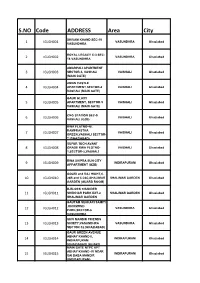
S.NO Code ADDRESS Area City SHIVAM KHAND SEC-19 VASUNDHRA Ghaziabad 1 IGLGH001 VASUNDHRA ROYAL LEGACY C-3 SEC- VASUNDHRA Ghaziabad 2 IGLGH002 18 VASUNDHRA AMARPALI APARTMENT 3 IGLGH003 SECTOR-3, VASHALI VAISHALI Ghaziabad (MAIN GATE) AMAN CASTLE 4 IGLGH004 APARTMENT SECTOR-4 VAISHALI Ghaziabad VASHALI (MAIN GATE) GAUR GLAXY 5 IGLGH005 APARTMENT, SECTOR-5 VAISHALI Ghaziabad VASHALI (MAIN GATE) CNG STATION SEC-9 VAISHALI Ghaziabad 6 IGLGH006 VASHALI (GZB) RWA FLATNO-48, RAMPRASTHA 7 IGLGH007 VAISHALI Ghaziabad GREEN,VASHALI SECTOR- 7 (GHAZIABAD) SUPER TECH AVANT 8 IGLGH008 GRADE RWA PLOTNO- VAISHALI Ghaziabad 1,SECTOR-5,VASHALI RWA SHIPRA SUN CITY INDIRAPURAM Ghaziabad 9 IGLGH009 APPARTMENT (GZB) GOURI and RAJ HIGHT,C- 10 IGLGH010 24B and C-24C,SHALIMAR SHALIMAR GARDEN Ghaziabad GARDEN (GUARD ROOM) B-BLOCK CHANDER 11 IGLGH011 SHEKHAR PARK EXT-2 SHALIMAR GARDEN Ghaziabad SHALIMAR GARDEN GAUTAM SEHKARI SAMITI ,RICHMOND 12 IGLGH012 VASUNDHRA Ghaziabad PARK,SECTOR-6 VASUNDHRA SHIV MANDIR FRIENDS 13 IGLGH013 SICIETY,VASUNDHRA VASUNDHRA Ghaziabad SECTOR-12.(GHAZIABAD) GAUR GREEN AVENUE ABHAY KHAND-II, 14 IGLGH014 INDIRAPURAM Ghaziabad INDIRAPURAM (GHAZIABAD) (GUARD MAIN GATE NTPC APT ABHAY KHAND -IV NEAR 15 IGLGH015 INDIRAPURAM Ghaziabad SAI BABA MANDIR (INDIRAPURAM) PNG CONTROL ROOM RAJINDER NAGAR,aman 16 IGLGH016 RAJINDER NAGAR Ghaziabad garden sector-5 (sahibabad) AHINSA KHAND -II ARIHANT PARADISO, 17 IGLGH017 INDIRAPURAM Ghaziabad INDIRAPURAM (GATENO- 1) VIJAYA APPARTMENT,AHINSA 18 IGLGH018 INDIRAPURAM Ghaziabad KHAND-II,INDIRAPURAM (MAIN -

State Profiles of Uttar Pradesh
State Profile Ground Water Scenario of Uttar Pradesh Area (Sq.km) 2,40,928 Rainfall (mm) 1279 Total Districts / Blocks 70 Districts Hydrogeology Hydrogeologically, the States can be divided into Five units namely (1) Bhabar (2) Tarai (3) Central Ganga plains (4) Marginal alluvial plains and (5) Southern Peninsular zone. The first one is in the extreme north followed successively by the rest southwardly. The yield of tubewells tapping Bhabar and Tarai zones ranges between 100-300 m3/hr and 100-200 m3/hr, respectively. The water level is deep in Bhabar where as in Tarai auto flow conditions are noticed with piezometric head of 6-9 magl. The Central Ganga plain is characterized by low relief and numerous alluvial features. There are four major aquifers in the depth range of 700 mbgl. The yield of these tubewells ranges from 90 to 200 m3/hr. The thickness of sediments in Marginal alluvium is 50-300 m and yield of tubewells is between 35 to 70 m3/hr. The yield prospects of Vindhyan & crystalline rocks in the southern peninsular region are limited. Dynamic Ground Water Resources (2011) Annual Replenishable Ground water Resource 77.19 BCM Net Annual Ground Water Availability 71.66 BCM Annual Ground Water Draft 52.78 BCM Stage of Ground Water Development 74 % Ground Water Development & Management Over Exploited 111 Blocks Critical 68 Blocks Semi- critical 82 Blocks Artificial Recharge to Ground Water (AR) . Area identified for AR: 110783 sq km . Volume of water to be harnessed: 5185 MCM . Volume of water to be harnessed through RTRWH:221.18 MCM . -

District Disaster Management Authority Ghaziabad District Administration, Collectorate Ghaziabad, Tel
Ghaziabad CITY DISASTER MANAGEMENT PLAN District Disaster Management Authority Ghaziabad District Administration, Collectorate Ghaziabad, Tel. No. 0120- 2824416, 2820106, 2822901, 2822902, Fax: 0120-2828798, Web: www.ghaziabad.nic.in GOI-UNDP Urban Risk Reduction Project Ghaziabad District City Disaster Management Plan 2011-2012 FORWORD The City Disaster Management Plan (CDMP) outlining the measures to be taken in the event of any natural or man-made disaster during the year 2011-2012 has been prepared on the basis of past experiences. The CDMP includes the facts and figures those have been collected from various sources with a view to meet the challenges during any Natural Disaster, while formulating the City Disaster Management Plan, instruction of Relief Commissioner, and also valuable suggestions of District Disaster Management Committee, have been taken into account. The plan is prepared to help the District Administration focus quickly on the essentials and crucial aspects of both preparedness and response. The plan deals with Risk Assessment and Vulnerability Analysis, Identification of Disaster Prone Areas, Response Structures, Inventory of Resources, Standard Operating Procedures, Directory of Institutions and key individuals etc. It is suggested that the District Level Officials who are in-charge of different departments will carefully go through the CDMP and remain alert to effectively countenance any emergent situations that may arise at any point of time. The CDMP is desired to serve as a useful handbook of operational guidelines for all concerned officials of the district, It is expected that District level Officials working in Ghaziabad District in different Departments will thoroughly acquaint themselves with these guidelines and also with the relevant provisions of Relief Code and CRF Guide Line.