Epidemiology of Osteoporotic Fracture in Moldova and Development of a Country-Specific FRAX Model
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
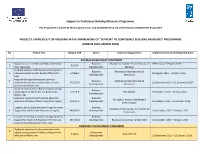
Projects Carried out Or Ongoing in the Framework of "Support to Confidence Building Measures" Programme (March 2015- March 2018)
Support to Confidence Building Measures Programme This Programme is funded by the European Union, and implemented by the United Nations Development Programme PROJECTS CARRIED OUT OR ONGOING IN THE FRAMEWORK OF "SUPPORT TO CONFIDENCE BUILDING MEASURES" PROGRAMME (MARCH 2015- MARCH 2018) No Project title Budget, EUR Sector Implementing partners Implementation period/Expected dates BUSINESS DEVELOPMENT COMPONENT Support to a set of CSOs and BAs and develop Business Chamber of Commerce and Industry of 29 February – 29 April, 2016 1 9,314 € their capacities Development Moldova In-depth analysis of the Business Development Business Alternative Internationale de 2 Services market on both banks of the Nistru 67,568 € 18 August, 2015 – 29 April, 2016 Development Dezvoltare river Improve the opportunities and services 3 Business Alternative Internationale de available for business communities on both 172,725 € 21 December 2015 – 21 December 2017 Development Dezvoltare banks of the Nistru river Study on entrepreneurship perception among Business 4 youth (aged 18-35) on the left bank of the 22,519 € CBS-AXA SRL 20 October, 2015 – 20 May, 2016 Development Nistru river Economic research and forecasts about the Business AO Centrul Analitic Independent 5 economic situation of the Transnistrian region 60,011 € Development 15 October, 2015 – 15 October, 2016 EXPERT-GRUP Creation of Job Opportunities through Business Business Chamber of Commerce and Industry of 6 Support for Youth in the Transnistria region 344,561 € Development 1 September, 2015 – 30 April, -

Report on Research Into the Process of Transition from Kindergarten to School
Ensuring Educational Inclusion for Children with Special Educational Needs Report on Research into the Process of Transition from Kindergarten to School Chisinau, 2015 1 Contents Abbreviations and acronymns ................................ ................................ .................... 2 1. Introduction ................................ ................................ ................................ .......... 3 1.1. Background to the research ................................ ................................ ............. 3 1.2. Background to the context ................................ ................................ ............... 5 2. Findings ................................ ................................ ................................ ................ 6 2.1. Attitudes towards inclusive education ................................ .............................. 6 2.2. Teaching and learning practices ................................ ................................ ...... 7 2.3. Parents’ roles and expectations ................................ ................................ ....... 8 2.4. Communication issues ................................ ................................ ................... 11 2.5. Specialist support ................................ ................................ .......................... 11 2.6. Suggestions from respondents to make transition more inclusive ................. 12 3. Conclusions ................................ ................................ ................................ ....... -

Rapid Assessment of Trafficking in Children for Labour and Sexual Exploitation in Moldova
PROject of Technical assistance against the Labour and Sexual Exploitation of Children, including Trafficking, in countries of Central and Eastern Europe PROTECT CEE www.ilo.org/childlabour International Programme on the Elimination of Child Labour (IPEC) International Labour Office 4, Route des Morillons CH 1211 Geneva 22 Switzerland Rapid Assessment of Trafficking E-mail: [email protected] Tel: (+41 22) 799 81 81 in Children for Labour and Sexual Fax: (+41 22) 799 87 71 Exploitation in Moldova ILO-IPEC PROTECT CEE ROMANIA intr. Cristian popisteanu nr. 1-3, Intrarea D, et. 5, cam. 574, Sector 1, 010024-Bucharest, ROMANIA [email protected] Tel: +40 21 313 29 65 Fax: +40 21 312 52 72 2003 ISBN 92-2-116201-X IPEC International Programme on the Elimination of Child Labour Rapid Assessment of Trafficking in Children for Labour and Sexual Exploitation in Moldova Prepared by the Institute for Public Policy, Moldova Under technical supervision of FAFO Institute for Applied International Studies, Norway for the International Programme on the Elimination of Child Labour (IPEC) of the International Labour Organization (ILO) Chisinau, 2003 Copyright © International Labour Organization 2004 Publications of the International Labour Office enjoy copyright under Protocol 2 of the Universal Copyright Convention. Nevertheless, short excerpts from them may be reproduced without authorization, on condition that the source is indicated. For rights of reproduction or translation, application should be made to the ILO Publications Bureau (Rights and Permissions), -

STUDY Finance Benchmarks: Areas and Options for Assessing Local Financial Resources and Financial Management in Moldova
STRENGTHENING INSTITUTIONAL FRAMEWORKS FOR LOCAL GOVERNANCE PROGRAMME 2015-2017 STUDY Finance Benchmarks: areas and options for assessing local financial resources and financial management in Moldova Author: Viorel Roscovan September 25, 2015 Table of contents 1. POLITICAL AND ADMINISTRATIVE STRUCTURE OF THE REPUBLIC OF MOLDOVA ....... 5 1.1. GENERAL DATA ...................................................................................................................................... 5 1.2. ADMINISTRATIVE-TERRITORIAL DIVISION AND LOCAL GOVERNMENTS .................................................. 5 1.3. POLITICAL STRUCTURE ........................................................................................................................... 6 2. LOCAL GOVERNMENT COMPETENCES ........................................................................................... 7 2.1. LOCAL GOVERNMENT FUNCTIONS, RESPONSIBILITIES, AND RIGHTS ........................................................ 7 2.2. INSTITUTIONAL STRUCTURE OF LOCAL GOVERNMENTS .......................................................................... 9 2.3. LOCAL GOVERNMENTS SUPERVISION .................................................................................................... 11 3. LOCAL GOVERNMENT OWN AND SHARED REVENUES ............................................................ 12 3.1. OWN REVENUES ................................................................................................................................... 13 3.2. SHARED TAXES AND FEES -
Progress Report for 2009
Contract number: 2009/219-955 Project Title: Building confidence between Chisinau and Tiraspol Report starting date: 01 January 2010 Report end date: 31 December 2011 Implementing agency: UNDP Moldova Country: Republic of Moldova Support to Confidence Building Measures II – Final Report 2010-2011 – submitted by UNDP Moldova 1 Table of Contents I. SUMMARY ................................................................................................................................................................. 3 II. CONTEXT ................................................................................................................................................................. 4 III. PROJECT BACKGROUND .................................................................................................................................. 5 1. BUSINESS DEVELOPMENT ............................................................................................................................................ 5 2. COMMUNITY DEVELOPMENT ........................................................................................................................................ 6 3. CIVIL SOCIETY DEVELOPMENT ...................................................................................................................................... 7 4. SUPPORT TO CREATION OF DNIESTER EUROREGION AND RESTORATION OF RAILWAY TRAFFIC. ........................................... 7 IV. SUMMARY OF IMPLEMENTATION PROGRESS ......................................................................................... -

Advancing Democracy and Human Rights PROMO-LEX ASSOCIATION
advancing democracy and human rights THE CIVIC COALITION FOR FREE AND FAIR ELECTIONS PROMO-LEX ASSOCIATION REPORT #3 Monitoring the preterm parliamentary elections of 28 November 2010 Monitoring period: 26 October 2010 – 8 November 2010 Published on 11 November 2010 Promo-LEX is grateful for the financial and technical assistance offered by the United States of America Embassy in Chisinau, the National Endowment for Democracy (NED), and the National Democratic Institute for International Affairs (NDI). The opinions expressed in this report do not necessarily reflect those of the donors. Page 1 of 28 Third monitoring report on the preterm parliamentary elections of 28 November 2010 CONTENTS: I. SUMMARY II. PROMO-LEX MONITORING EFFORT III. INTRODUCTION A. Legal framework B. Electoral competitors C. Election authorities D. Local authorities E. Electoral campaigning F. Financial analysis G. Mass media H. National and international observers I. Transnistrian region IV. CONCERNS V. RECOMMENDATIONS Page 2 of 28 I. SUMMARY This report, covering the period from October 25 through November 8, 2010, describes the electoral environment and reviews from a legal perspective the recent developments in the election campaign, and the performance of the electoral competitors and of the local and election authorities. The election campaign is becoming increasingly intense, with cases of intimidation and abuse being registered both against electoral competitors and voters. While engaged in various campaigning activities, some candidates resort to the misuse of administrative resources and offering of “electoral gifts”. Promo-LEX salutes the impartiality of the election authorities in performing their duties. The Central Election Commission registered until the end of the authorization period 40 electoral competitors and issued warnings to the contenders that violated the rules. -

Proposal for Moldova
AFB/PPRC.24/29 26 February, 2019 Adaptation Fund Board Project and Programme Review Committee Twenty-Third Meeting Bonn, Germany, 12-13 March , 2019 Agenda Item 9 v) PROPOSAL FOR MOLDOVA AFB/PPRC.24/29 Background 1. The Operational Policies and Guidelines (OPG) for Parties to Access Resources from the Adaptation Fund (the Fund), adopted by the Adaptation Fund Board (the Board), state in paragraph 45 that regular adaptation project and programme proposals, i.e. those that request funding exceeding US$ 1 million, would undergo either a one-step, or a two-step approval process. In case of the one-step process, the proponent would directly submit a fully-developed project proposal. In the two-step process, the proponent would first submit a brief project concept, which would be reviewed by the Project and Programme Review Committee (PPRC) and would have to receive the endorsement of the Board. In the second step, the fully- developed project/programme document would be reviewed by the PPRC, and would ultimately require the Board’s approval. 2. The Templates approved by the Board (Annex 5 of the OPG, as amended in March 2016) do not include a separate template for project and programme concepts but provide that these are to be submitted using the project and programme proposal template. The section on Adaptation Fund Project Review Criteria states: For regular projects using the two-step approval process, only the first four criteria will be applied when reviewing the 1st step for regular project concept. In addition, the information provided in the 1st step approval process with respect to the review criteria for the regular project concept could be less detailed than the information in the request for approval template submitted at the 2nd step approval process. -
Report of the Observance of Human Rights and Freedoms in The
REPORT ON THE OBSERVANCE OF HUMAN RIGHTS AND FREEDOMS IN THE REPUBLIC OF MOLDOVA IN 2016 CHISINAU, 2017 1 CONTENTS Foreword..................................................................................................................3 Universal Periodic Review..............................................................................................7 CHAPTER I OBSERVANCE OF HUMAN RIGHTS AND FREEDOMS IN THE REPUBLIC OF MOLDOVA Equality before law and public authorities .............................................................................9 Legal status of foreign citizens and stateless persons …………………………………...…14 Right to a fair trial .................................................................................................................17 Right to life, physical and mental integrity…........................................................................22 Individual freedom and personal security.................................................................. 29 Private and family life…………...............................................................................31 Freedom of expression……………………………………………………………………..34 Right to information………………………………………………………………………..41 Right to health protection….……..........................................................................................44 Right to a clean environment…………..……………………………………………….......51 Right to vote and right to be elected .....................................................................................60 Freedom of assembly……………………………………………………………………….63 -

Children in the Republic of Moldova
CHILDREN IN THE REPUBLIC OF MOLDOVA SITUATION ANALYSIS 2016 This report was produced with the support of UNICEF Moldova. Authors: Dennis Arends, Mariana Ianachevici, Ala Nemerenco, Arina Turcan Quality assurance: Camelia Gheorghe Acknowledgements The Situation Analysis was developed by a team of consultants: Mariana Ianachevici, Ala Nemerenco and Arina Turcan under the leadership of Dennis Arends. Quality assurance review was completed by Camelia Gheorghe. The research was supported by UNICEF Moldova. We are thankful to UNICEF programme team colleagues who provided expertise and contributed extensively to the review of the document. UNICEF is immensely grateful for the support and extensive reviews provided by government counterparts: the State Chancellery of the Republic of Moldova, the National Bureau of Statistics, the Ministry of Education, the Ministry of Health, the Ministry of Labour, Social Protection and Family , the Ministry of Justice and other relevant ministries, state institutions and government agencies, including the Ombudsperson for Child Rights. Stakeholders consulted during the field research included national-level policymakers, local public authorities, professionals, representatives from non-governmental organizations, as well as adolescents and youth. UNICEF is very grateful for their invaluable contributions to the research as well. Extracts from this publication may be freely reproduced with due acknowledgment using the following reference: UNICEF, ‘Children in the Republic of Moldova: A Situation Analysis’, 2016. -

Request for Project/Programme Funding from the Adaptation Fund
REQUEST FOR PROJECT/PROGRAMME FUNDING FROM THE ADAPTATION FUND The annexed form should be completed and transmitted to the Adaptation Fund Board Secretariat by email or fax. Please type in the responses using the template provided. The instructions attached to the form provide guidance to filling out the template. Please note that a project/programme must be fully prepared (i.e., fully appraised for feasibility) when the request is submitted. The final project/programme document resulting from the appraisal process should be attached to this request for funding. Complete documentation should be sent to: The Adaptation Fund Board Secretariat 1818 H Street NW MSN P4-400 Washington, D.C., 20433 U.S.A Fax: +1 (202) 522-3240/5 Email: [email protected] Table of Contents Abbreviations and Acronyms ................................................................................................. vi PART I PROJECT INFORMATION ................................................................................. 1 Background and Context. ...................................................................................................... 1 A Geography ................................................................................................................................... 1 B Climate ......................................................................................................................................... 2 C Economy ..................................................................................................................................... -

Geological and Hydrological Survey for the Tintareni Landfill. Summary Moldova: Chisinau Solid Waste Project Feasibility Study C
Geological and Hydrological Survey for the Tintareni Landfill. Summary Moldova: Chisinau Solid Waste Project Feasibility Study Contract No. C32112/SWM2-2015-08-09 European Bank for Reconstruction and Development (EBRD) Summary Report November 2016 This project is supported by the Government of Sweden. FICHTNER MANAGEMENT CONSULTING AG Stuttgart Berlin Sarweystrasse 5 D-70191 Stuttgart Tel.: +49 711 8995-750 Fax: +49 711 8995-1491 www.fmc.fichtner.de Contact person Dr. Maria Belova Chisinau landfill geological study results (Tintareni) Moldova: Chisinau Solid Waste Project Feasibility Study For public use Disclaimer The content of this report is intended for the exclusive use of FICHTNER's client and other agreed recipients. It may only be made available in whole or in part to third parties on non- reliance basis. FICHTNER is not liable to third parties for the completeness and accuracy of the information provided therein. 3 Chisinau landfill geological study results (Tintareni) Moldova: Chisinau Solid Waste Project Feasibility Study For public use Table of Contents Disclaimer 3 Table of Contents 4 List of Figures 5 List of Tables 5 List of Abbreviations 5 1. General Overview 6 2. Physical-geographical conditions 7 3. Geomorphology and geology of the investigated area 8 4. Results evaluation of the drilling works 8 5. Hydrologic characteristics 9 6. Geological-engineering characteristics of the investigation site 11 7. Slope and dam stability 12 4 Chisinau landfill geological study results (Tintareni) Moldova: Chisinau Solid Waste Project Feasibility Study For public use List of Figures Figure 1: Location of boreholes (BH) ......................................................................................... 6 Figure 2: 3D representation of intersecting lithologies.............................................................. -

Questions About Orhei National Park
Questions about Orhei National Park 1 The booklet was developed under the Awareness Raising and Information Program on biodiversity conservation for Orhei region as part of the UNDP project “Strengthening the institutional capacity and representativeness of the Protected Area System in Moldova”, funded by the Global Environment Facility. The purpose of the booklet is to answer the most common 15 questions about Orhei National Park. The views expressed in this publication do not necessarily reflect the official views of the United Nations Develop- ment Programme in Moldova and other international organizations involved in the project. Author: AO “ProRuralInvest” Photo: Alecu Renita, www.sxc.hu Design and layout: Mancas Mihail 15 Questions about Orhei National Park Copyright © 2010-2011 UNDP Moldova 2 CONTENTS 1. What are the protected areas? 2. What are National Parks? 3. What are the zones of National Parks? 4. Where is Orhei National Park located? 5. What are the main values of Orhei National Park? 6. What are the benefits of Orhei National Park to the community? 7. May other products found in the areas located within Orhei National Park (mushrooms, medicinal herbs) be cultivated and harvested? 8. May the wood from the forest located in Orhei National Park be used? 9. May livestock growing activities be carried out within Orhei National Park? 10. What regime is applied to tourism units operating within Orhei National Park? 11. What hunting regime is applied in Orhei National Park? 12. What are my rights as an owner or user of land located within Orhei National Park? 13. May the activities carried out before the inclusion of land in Orhei National Park be continued, even if these are profit- oriented? 14.