An Improved Method to Visualize Eosinophils in Eosinophilic Esophagitis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Eosinophilic Gastroenteritis Presenting with Severe Anemia and Near Syncope
J Am Board Fam Med: first published as 10.3122/jabfm.2012.06.110269 on 7 November 2012. Downloaded from BRIEF REPORT Eosinophilic Gastroenteritis Presenting with Severe Anemia and Near Syncope Nneka Ekunno, DO, MPH, Kirk Munsayac, DO, Allen Pelletier, MD, and Thad Wilkins, MD Eosinophilic gastrointestinal disorders or eosinophilic digestive disorders encompass a spectrum of rare gastrointestinal disorders that includes eosinophilic esophagitis, eosinophilic gastroenteritis, and eosinophilic colitis. Eosinophilic gastroenteritis is a rare inflammatory disease characterized by eosino- philic infiltration of the gastrointestinal tract. The clinical manifestations include anemia, dyspepsia, and diarrhea. Endoscopy with biopsy showing histologic evidence of eosinophilic infiltration is consid- ered definitive for diagnosis. Corticosteroid therapy, food allergen testing, elimination diets, and ele- mental diets are considered effective treatments for eosinophilic gastroenteritis. The treatment and prognosis of eosinophilic gastroenteritis is determined by the severity of the clinical manifestations. We describe a 24-year-old woman with eosinophilic gastroenteritis presenting as epigastric pain with a history of severe iron deficiency anemia, asthma, eczema, and allergic rhinitis, and we review the litera- ture regarding presentation, diagnostic testing, pathophysiology, predisposing factors, and treatment recommendations. (J Am Board Fam Med 2012;25:913–918.) Keywords: Case Reports, Eosinophilic Gastroenteritis, Gastrointestinal Disorders copyright. A 24-year-old nulliparous African-American woman During examination, her height was 62 inches, was admitted after an episode of near syncope asso- weight 117 lb, and body mass index 21.44 kg/m2. Her ciated with 2 days of fatigue and dizziness. She re- heart rate was 111 beats per minute, blood pressure ported gradual onset of dyspepsia over 2 to 3 121/57 mm Hg, respiratory rate 20 breaths per minute, months. -
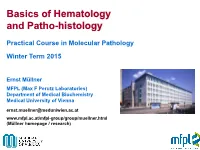
Basics of Hematology and Patho-Histology
Basics of Hematology and Patho-histology Practical Course in Molecular Pathology Winter Term 2015 Ernst Müllner MFPL (Max F Perutz Laboratories) Department of Medical Biochemistry Medical University of Vienna [email protected] www.mfpl.ac.at/mfpl-group/group/muellner.html (Müllner homepage / research) E. coli + macrophages medicalschool.tumblr.com/post/43914024728/sem-image-of-e-coli-bacteria-and-macrophages medicalschool.tumblr.com/post/18256087351/r ed-blood-cells-erythrocytes-trapped-by-fibrin Overview on main white blood cell (WBC) types – (Wikipedia) Mature white blood cell types I White Blood cells (WBCs) are frequently also referred to as peripheral blood mononuclear cells (PBMCs). Granulocytes in general are part of the innate immune system. Names derive from staining with hematoxylin and eosin. Whereas basophils stain dark blue and eosinophils are bright red, neutrophils stain neutral to pink. Basophil granulocytes Eosinophil granulocytes Neutrophil granulocytes Least common granulocyte type About 1-6% of WBCs; component Most abundant WBC type (40- (0.01- 0.3% of WBCs. Large of innate immune system to com- 75%) and essential part of the cytoplasmic granules obscure the bat parasites and certain infec- innate immune system. A patho- nucleus under the microscope. tions; also associated with allergy gen is likely to first encounter a When unstained, the nucleus is and asthma. Following activation, neutrophil. Normally contain a nu- visible and usually has 2 lobes. eosinophils effector functions in- cleus of 2-5 lobes. Neutrophils Basophils appear in inflammatory clude production and release (de- quickly congregate at a infection reactions, particularly those granulation) of cytotoxic substan- site, attracted by cytokines from causing allergies, mainly via the ces (granule proteins, reactive activated endothelium, mast cells, vasodilator histamine (antihistami- oxygen species …) and production or macrophages. -

Eosinophilic Gastrointestinal Disorders
Clinical Reviews in Allergy & Immunology (2019) 57:272–285 https://doi.org/10.1007/s12016-019-08732-1 Eosinophilic Gastrointestinal Disorders Nirmala Gonsalves1 Published online:22 March 2019 # Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract Eosinophilic gastrointestinal disorders (EGID) are a group of disorders characterized by pathologic eosinophilic infiltration of the esophagus, stomach, small intestine, or colon leading to organ dysfunction and clinical symptoms (J Pediatr Gastroenterol Nutr; Spergel et al., 52: 300–306, 2011). These disorders include eosinophilic esophagitis (EoE), eosinophilic gastritis (EG), eosino- philic gastroenteritis (EGE), eosinophilic enteritis (EE), and eosinophilic colitis (EC). Symptoms are dependent not only on the location (organ) as well as extent (layer invasion of the bowel wall). Common symptoms of EoE include dysphagia and food impaction in adults and heartburn, abdominal pain, and vomiting in children. Common symptoms of the other EGIDs include abdominal pain, nausea, vomiting, early satiety, diarrhea, and weight loss. These disorders are considered immune-mediated chronic inflammatory disorders with strong links to food allergen triggers. Treatment strategies focus on either medical or dietary therapy. These options include not only controlling symptoms and bowel inflammation but also on identifying potential food triggers. This chapter will focus on the clinical presentation, pathophysiology, and treatment of these increasingly recognized disorders. Keywords Eosinophilic gastroenteritis . Eosinophilic gastritis . Eosinophilic esophagitis . Dysphagia . Food impaction . Food allergy Introduction purpose of this chapter, we will discuss these disorders sepa- rately and focus on the available data on the clinical presenta- Eosinophilic gastrointestinal disorders (EGID) are a group of tion, pathophysiology, and treatment. disorders characterized by pathologic eosinophilic infiltration of the esophagus, stomach, small intestine, or colon leading to organ dysfunction and clinical symptoms [1]. -

Utility of Direct Fast Scarlet Staining in the Histopathological Diagnosis of Eosinophilic Esophagitis: a Short Report
Brief Report Utility of Direct Fast Scarlet Staining in the Histopathological Diagnosis of Eosinophilic Esophagitis: A Short Report Takuji Tanaka 1,* , Naoki Watanabe 1, Tomohiro Kato 2, Ryogo Aoki 1, Tomio Ogiso 2, Akihiko Sugiyama 2 and Eiichi Tomita 2 1 Department of Diagnostic Pathology & Research Center of Diagnostic Pathology, Gifu Municipal Hospital, 7-1 Kashima-cho, Gifu City 500-8513, Japan; [email protected] (N.W.); [email protected] (R.A.) 2 Department of Internal Medicine, Gifu Municipal Hospital, Gifu City 500-8513, Japan; [email protected] (T.K.); [email protected] (T.O.); [email protected] (A.S.); [email protected] (E.T.) * Correspondence: [email protected] Received: 7 October 2020; Accepted: 29 October 2020; Published: 9 November 2020 Abstract: Eosinophilic esophagitis (EoE), an atopic disease of the esophagus, has become increasingly recognized over the last 15 years. The epidemiology of EoE has now been reported from many countries around the world. While the clinical diagnosis of this disease depends on the patient’s clinical manifestations, the final diagnosis should be made based on the histopathological examination of esophageal mucosal biopsies. In the diagnosis of EoE, to facilitate the appropriate treatment of patients, it is extremely important to precisely recognize the presence of eosinophils in biopsy specimens of the esophageal mucosa. If eosinophils are present, EoE patients should be referred to an allergist for appropriate management with dietary modification, pharmacological agents (including corticosteroids), and/or mechanical dilation of the esophagus. We herein present and recommend the use of direct fast scarlet staining for the easy and precise recognition of eosinophils in biopsy specimens of the esophageal mucosa, a technique that has been routinely used in our laboratory. -

Is Hybrid Oncocytic/Chromophobe Renal Tumor a Subtype of Oncocytoma, Chromophobe Renal Cell Carcinoma, Or a Distinct Tumor Entity?
350 Editorial Commentary Page 1 of 5 Classification of solid renal tumor with oncocytic/eosinophilic cytoplasm: is hybrid oncocytic/chromophobe renal tumor a subtype of oncocytoma, chromophobe renal cell carcinoma, or a distinct tumor entity? Shuji Mikami1, Naoto Kuroda2, Yoji Nagashima3, Chisato Ohe4, Hiroyuki Hayashi5, Ryuichi Mizuno6, Mototsugu Oya6, Kaori Kameyama1 1Department of Diagnostic Pathology, Keio University Hospital, Tokyo Japan; 2Department of Diagnostic Pathology, Kochi Red Cross Hospital, Kochi, Japan; 3Department of Surgical Pathology, Tokyo Women’s Medical University, Tokyo, Japan; 4Department of Pathology, Kansai Medical University Hospital, Osaka, Japan; 5Department of Pathology, Fukuoka University Hospital, Fukuoka, Japan; 6Department of Urology, Keio University Hospital, Tokyo, Japan Correspondence to: Shuji Mikami, MD, PhD. Department of Diagnostic Pathology, Keio University Hospital, 35 Shinanomachi, Shinjuku-ku, Tokyo 160-8582, Japan. Email: [email protected]. Provenance: This is an invited article commissioned by the Section Editor Dr. Xiao Li (Department of Urology, Jiangsu Cancer Hospital, Jiangsu Institute of Cancer Research, Nanjing Medical University Affiliated Cancer Hospital, Nanjing, Chnia). Comment on: Ruiz-Cordero R, Rao P, Li L, et al. Hybrid oncocytic/chromophobe renal tumors are molecularly distinct from oncocytoma and chromophobe renal cell carcinoma. Mod Pathol 2019. [Epub ahead of print]. Submitted Sep 01, 2019. Accepted for publication Sep 12, 2019. doi: 10.21037/atm.2019.09.77 View this article at: http://dx.doi.org/10.21037/atm.2019.09.77 Pathological diagnosis of oncocytic renal tumor is usually or a distinct renal tumor entity. Therefore, we comment on difficult task, and their differential diagnosis involves important studies of HOCT including recently published chromophobe renal cell carcinoma (ChRCC), renal paper by Ruiz-Cordero et al. -
Near Fatal Eosinophilic Gastroenteritis Responding to Oral Sodium Chromoglycate
Gut: first published as 10.1136/gut.29.9.1282 on 1 September 1988. Downloaded from Gut, 1988, 29, 1282-1285 Case report Near fatal eosinophilic gastroenteritis responding to oral sodium chromoglycate R J MOOTS, P PROUSE, AND J M GUMPEL From Northwick Park Hospital, Harrow, Middlesex SUMMARY Eosinophilic gastroenteritis (EG) is an uncommon disorder, characterised by cramping abdominal pain, diarrhoea and vomiting and histologically by eosinophilic infiltration of bowel wall.' We present a patient who developed EG during the course ofa systemic, necrotising vasculitis, who became critically ill after failure of treatment with corticosteroids and cytotoxic drugs and responded only to oral sodium chromoglycate. Case report bleeding. By then her condition required admission to hospital. A 57 years old cachectic woman was admitted as an On admission she was taking prednisolone (ec) 10 http://gut.bmj.com/ emergency, with a five months history of increasing and 15 mg on alternate days, cyclophosphamide 100 epigastric pains, anorexia, bloody diarrhoea, and mg once a day, spironolactone 50 mg twice a day and weight loss. cimetidine 400 mg twice a day. Her weight was only Ten years earlier, she had been diagnosed as 50 kg after a total weight loss of 20 kg. Clinically, her having a sero negative, non-erosive, symmetrical abdomen was generally distended and there was polyarthritis. A year before this admission she was evidence of gross fluid retention: the peripheral investigated for a painful peripheral neuropathy, neuropathy was unchanged. Initial investigations on September 25, 2021 by guest. Protected copyright. livedo reticularis skin rash and leg ulcers. Non- revealed Hb 107 g/dl, with a lymphocytopaenia and specific vasculitis was present on a skin biopsy. -
Eosinophilic Gastrointestinal Diseases (Egids)
Journal of Pediatric Gastroenterology and Nutrition 47:234–238 # 2008 by European Society for Pediatric Gastroenterology, Hepatology, and Nutrition and North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition Eosinophilic Gastrointestinal Diseases (EGIDs) EGIDs Working Group: ôGlenn T. Furuta, yyDavid Forbes, zzChris Boey, yC. Dupont, §§Phil Putnam, ôS.K. Roy, ÃAderbal Sabra´, jjAnadina Salvatierra, §Yuichiro Yamashiro, and ÃÃS. Husby ÃyDepartment of Paediatrics and Nutrition, Hospital Saint Vincent de Paul, Paris, France, {International Centre for Diarrhoeal Disease Research, Bangaldesh, Dhaka, §Probiotics Research Laboratory, Juntendo University School of Medicine, Tokyo, Japan, ôUniversity of Colorado School of Medicine, Denver, ÃÃDepartment of Paediatrics, Odense University Hospital, Odense, Denmark, {{School of Paediatrics and Child Health, University of Western Australia, Perth, {{Pediatric Gastroenterology and Hepatology, Department of Pediatrics, University of Malaya Medical Centre, Kuala Lumpur, Malaysia, and §§Department of Pediatrics, Cincinnati Children’s Hospital Medical Center, University of Cincinnati College of Medicine, Cincinnati, OH Eosinophilic gastrointestinal diseases (EGIDs) are a rarity of the diseases limits well-designed studies and heterogeneous group of diseases (eosinophilic esophagi- precludes consensus on histological features; in fact, only tis [EoE], eosinophilic gastroenteritis, and eosinophilic recently have studies explored the normal numbers of colitis) characterized by gastrointestinal symptoms and eosinophils in the different part of the gastrointestinal increased eosinophils in the intestinal mucosa; more tract (1,2). A gradient exists with respect to the normal important, other causes of gastrointestinal eosinophilia number of eosinophils per high power field (eos/HPF) in must have been ruled out for the diagnosis of EGIDs to be the gastrointestinal (GI) tract starting with the esophagus, confirmed. -

Quantification of Histopathology in Haemotoxylin and Eosin Stained Muscle Sections
DMD_M.1.2.007 Please quote the use of this SOP in your Methods. Quantification of histopathology in Haemotoxylin and Eosin stained muscle sections SOP (ID) Number DMD_M.1.2.007 Version 1.0 Issued May 18th, 2010 Last reviewed January 25th, 2014 Author Miranda Grounds School of Anatomy and Human Biology, the University of Western Australia, Perth, Australia Working group Hannah Radley-Crabb (School of Anatomy and Human Biology, members the University of Western Australia, Perth, Australia) Kanneboyina Nagaraju (Research Center for Genetic Medicine, Children's National Medical Center 111 Michigan Avenue, N.W. Washington, DC 20010) Annemieke Aartsma-Rus (Leiden University Medical Center, Department of Human Genetics, Leiden, The Netherlands) Maaike van Putten (Leiden University Medical Center, Department of Human Genetics, Leiden, The Netherlands) Markus A. Rüegg (Biozentrum, University of Basel, Basel, Switzerland) Sabine de La Porte (Laboratoire de Neurobiologie Cellulaire et Moléculaire, CNRS UPR 9040, Gif sur Yvette, France) SOP responsible Miranda Grounds Official reviewer Nagaraju Kanneboyina Page 1 of 13 DMD_M.1.2.007 TABLE OF CONTENTS OBJECTIVE .................................................................................................................................. 3 SCOPE AND APPLICABILITY ........................................................................................................ 3 CAUTIONS ................................................................................................................................. -
Classification of Renal Cell Tumors – Current Concepts and Use Of
Athanazio et al. Surgical and Experimental Pathology (2021) 4:4 Surgical and Experimental https://doi.org/10.1186/s42047-020-00084-x Pathology REVIEW Open Access Classification of renal cell tumors – current concepts and use of ancillary tests: recommendations of the Brazilian Society of Pathology Daniel Abensur Athanazio1,2* , Luciana Schultz Amorim3, Isabela Werneck da Cunha4, Katia Ramos Moreira Leite5, Alexandre Rolim da Paz6,7, Regina de Paula Xavier Gomes8,9,10, Fabio Rocha Fernandes Tavora11,12, Sheila Friedrich Faraj13,14, Marcela Santos Cavalcanti15,16 and Stephania Martins Bezerra17 Abstract Classification of renal cell carcinomas has become more challenging. The 2016 WHO classification included 14 different subtypes and 4 emerging/provisional entities, and recent literature indicates new entities to be incorporated. Nomenclature is based on cytoplasmic appearance, architecture, combination of morphologies, anatomic location, underlying disease, familial syndromes, and specific genetic alterations. Immunohistochemistry is useful in selected cases while it can be insufficient in entities that require molecular confirmation of a specific gene alteration. The aim of these recommendations is to provide a reasonable and optimized approach for the use of ancillary tests in subtyping renal tumors, particularly in resource-limited settings. Keywords: Carcinoma, renal cell, Pathology, molecular, Immunohistochemistry, Classification Background and treatment of diseases. In cancer, it can also be viewed Renal cell carcinomas (RCCs) encompass 1–3% of hu- as a way of cataloging evolutionary trajectories of complex man malignancies and 75–80% of adult kidney cancers. genomes. In times of globalization and big data acquisition, Pathologic classification of renal carcinomas is complex, large cohorts have revealed not only biological diversity and nomenclature is based on cytoplasmic appearance, within known entities, but also previously unrecognized architecture, combination of morphologies, anatomic lo- ones. -
Eosinophil-Associated Inflammation and Elaboration of Eosinophil-Derived Proteins in 2 Children with Raccoon Roundworm (Baylisascaris Procyonis) Encephalitis
Eosinophil-Associated Inflammation and Elaboration of Eosinophil-Derived Proteins in 2 Children With Raccoon Roundworm (Baylisascaris procyonis) Encephalitis Christopher L. Moertel, MD*; Kevin R. Kazacos, DVM, PhD‡; Joseph H. Butterfield, MD§; Hirohito Kita, MDʈ; Jan Watterson, BA*; and Gerald J. Gleich, MDʈ ABSTRACT. Objective. Eosinophil-associated pro- aylisascaris procyonis, the common raccoon as- teins, especially eosinophil-derived neurotoxin, may be carid, is a well-known cause of severe neuro- important contributors to the neurologic pathology and logic disease (neural larva migrans) in animals, B Ͼ symptoms caused by Baylisascaris procyonis infection. with cases identified in 90 species of mammals and Methods. Two cases of severe B procyonis encephali- birds in North America.1,2 Neural larva migrans and tis with evidence of marked eosinophil degranulation in eosinophilic meningoencephalitis attributable to B the central nervous system are presented. Serial cerebro- procyonis have now been identified in 7 young chil- spinal fluid (CSF) specimens were collected from each dren, including the 2 reported here.3–7 We specifi- patient during the course of their illness. Antibodies cally note a novel correlation with elevated cerebro- against B procyonis were measured in the patients’ serum spinal fluid (CSF) levels of major basic protein and and CSF. Levels of the eosinophilopoietin interleukin-5 the neurotoxic protein eosinophil-derived neuro- (IL-5) and 2 important eosinophil proteins, eosinophil- toxin associated with eosinophilic inflammation in derived neurotoxin and major basic protein, were as- sayed in the CSF. these 2 cases. We hypothesize that the severe neuro- Results. Both patients had rapidly progressive central logic consequences of Baylisascaris encephalitis are nervous system disease with evidence of eosinophilic attributable, in part, to marked eosinophil degranu- meningoencephalitis. -
Newly Developed and Validated Eosinophilic Esophagitis Histology
Xavier University Exhibit Faculty Scholarship Health Services Administration 2016 Newly Developed and Validated Eosinophilic Esophagitis Histology Scoring System and Evidence that it Outperforms Peak Eosinophil Count for Disease Diagnosis and Monitoring Margaret H. Collins University of Cincinnati College of Medicine, Cincinnati Children's Hospital Medical Center Lisa J. Martin University of Cincinnati College of Medicine, Cincinnati Children's Hospital Medical Center Eileen Steinle Alexander Xavier University, Cincinnati Children's Hospital Medical Center J Todd Boyd University of Cincinnati College of Medicine, Cincinnati Children's Hospital Medical Center Rachel Sheridan University of Cincinnati College of Medicine, Cincinnati Children's Hospital Medical Center Follow this and additional works at: http://www.exhibit.xavier.edu/ heSee alth_snext pagee forrv addiceis_ationadminil authorsstration_faculty Part of the Digestive System Diseases Commons, Disease Modeling Commons, Disorders of Environmental Origin Commons, Life Sciences Commons, and the Public Health Commons Recommended Citation Collins, Margaret H.; Martin, Lisa J.; Alexander, Eileen Steinle; Boyd, J Todd; Sheridan, Rachel; He, Hua; Pentiuk, Scott; Putnam, Philip E.; Abonia, J Pablo; Mukkada, Vincent A.; Franciosi, James P.; and Rothenberg, Marc E., "Newly Developed and Validated Eosinophilic Esophagitis Histology Scoring System and Evidence that it Outperforms Peak Eosinophil Count for Disease Diagnosis and Monitoring" (2016). Faculty Scholarship. Paper 20. http://www.exhibit.xavier.edu/health_services_administration_faculty/20 This Article is brought to you for free and open access by the Health Services Administration at Exhibit. It has been accepted for inclusion in Faculty Scholarship by an authorized administrator of Exhibit. For more information, please contact [email protected]. Authors Margaret H. Collins, Lisa J. Martin, Eileen Steinle Alexander, J Todd Boyd, Rachel Sheridan, Hua He, Scott Pentiuk, Philip E. -

Molecular Genetics of Renal Cell Tumors: a Practical Diagnostic Approach
cancers Review Molecular Genetics of Renal Cell Tumors: A Practical Diagnostic Approach Reza Alaghehbandan 1 , Delia Perez Montiel 2, Ana Silvia Luis 3,4 and Ondrej Hes 5,* 1 Department of Pathology, Faculty of Medicine, University of British Columbia, Royal Columbian Hospital, Vancouver, BC V3E 0G9, Canada; [email protected] 2 Department of Pathology, Institute Nacional de Cancerologia, INCAN, Mexico DF 14080, Mexico; [email protected] 3 Department of Pathology, Centro Hospitalar de Vila Nova de Gaia-Espinho, Vila Nova de Gaia, Cancer Biology and Epigenetics Group (CBEG), IPO Porto Research Center (CI-IPOP), Portuguese Oncology Institute of Porto (IPO Porto) & Porto Comprehensive Cancer Center (P.CCC), 4200-072 Porto, Portugal; [email protected] 4 Department of Microscopy, Institute of Biomedical Sciences Abel Salazar, University of Porto (ICBAS-UP), 4200-072 Porto, Portugal 5 Department of Pathology, Charles University in Prague, Faculty of Medicine in Plzen, 304 60 Pilsen, Czech Republic * Correspondence: [email protected] Received: 1 December 2019; Accepted: 23 December 2019; Published: 30 December 2019 Abstract: Renal epithelial cell tumors are composed of a heterogeneous group of tumors with variable morphologic, immunohistochemical, and molecular features. A “histo-molecular” approach is now an integral part of defining renal tumors, aiming to be clinically and therapeutically pertinent. Most renal epithelial tumors including the new and emerging entities have distinct molecular and genetic features which can be detected using various methods. Most renal epithelial tumors can be diagnosed easily based on pure histologic findings with or without immunohistochemical examination. Furthermore, molecular-genetic testing can be utilized to assist in arriving at an accurate diagnosis.