World Bank Document
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Botswana Environment Statistics Water Digest 2018
Botswana Environment Statistics Water Digest 2018 Private Bag 0024 Gaborone TOLL FREE NUMBER: 0800600200 Tel: ( +267) 367 1300 Fax: ( +267) 395 2201 E-mail: [email protected] Website: http://www.statsbots.org.bw Published by STATISTICS BOTSWANA Private Bag 0024, Gaborone Phone: 3671300 Fax: 3952201 Email: [email protected] Website: www.statsbots.org.bw Contact Unit: Environment Statistics Unit Phone: 367 1300 ISBN: 978-99968-482-3-0 (e-book) Copyright © Statistics Botswana 2020 No part of this information shall be reproduced, stored in a Retrieval system, or even transmitted in any form or by any means, whether electronically, mechanically, photocopying or otherwise, without the prior permission of Statistics Botswana. BOTSWANA ENVIRONMENT STATISTICS WATER DIGEST 2018 Statistics Botswana PREFACE This is Statistics Botswana’s annual Botswana Environment Statistics: Water Digest. It is the first solely water statistics annual digest. This Digest will provide data for use by decision-makers in water management and development and provide tools for the monitoring of trends in water statistics. The indicators in this report cover data on dam levels, water production, billed water consumption, non-revenue water, and water supplied to mines. It is envisaged that coverage of indicators will be expanded as more data becomes available. International standards and guidelines were followed in the compilation of this report. The United Nations Framework for the Development of Environment Statistics (UNFDES) and the United Nations International Recommendations for Water Statistics were particularly useful guidelines. The data collected herein will feed into the UN System of Environmental Economic Accounting (SEEA) for water and hence facilitate an informed management of water resources. -

Ethnozoological Survey of the Indigenous Knowledge on the Use of Pangolins (Manis Sps) in Traditional Medicine in Lentsweletau Extended Area in Botswana
Journal of Animal Science Advances Ethnozoological Survey of the Indigenous Knowledge on the Use of Pangolins (Manis Sps) in Traditional Medicine in Lentsweletau Extended Area in Botswana Setlalekgomo M. R. J Anim Sci Adv 2014, 4(6): 883-890 DOI: 10.5455/jasa.20140526093512 Online version is available on: www.grjournals.com ISSN: 2251-7219 SETLALEKGOMO M. R. Original Article Ethnozoological Survey of the Indigenous Knowledge on the Use of Pangolins (Manis Sps) in Traditional Medicine in Lentsweletau Extended Area in Botswana Setlalekgomo M. R. *Botswana College of Agriculture, Private Bag 0027, Gaborone, Botswana. Abstract Animals have played an important role in human life from prehistory. Many animals are used in zootherapy worldwide. However, the zootherapeutic practices by some communities are not well documented and may be forgotten. An ethnozoological study to document indigenous knowledge on the utilisation of pangolins in traditional medicine in Lentsweletau area in Botswana was carried out. A formal questionnaire was administered to 37 informants. The informants were 70.27% males and 29.73% females. The 10.81% of the informants were traditional doctors. Only 67.57% of the informants knew pangolins. The study revealed that most of the informants currently under the age of forty years did not know pangolins. However, the community had several pangolin myths. Pangolins were used mainly in traditional medicine (79.41%) and rarely as bush meat (20.59%) in the past. The study showed that different body parts of pangolins were used as charms and in the treatment of various human ailments like cracked heels, epistaxis, hypertension and psoriasis. The commonly used parts in the treatment of human ailments were blood and scales. -

Land Tenure Reforms and Social Transformation in Botswana: Implications for Urbanization
Land Tenure Reforms and Social Transformation in Botswana: Implications for Urbanization. Item Type text; Electronic Dissertation Authors Ijagbemi, Bayo, 1963- Publisher The University of Arizona. Rights Copyright © is held by the author. Digital access to this material is made possible by the University Libraries, University of Arizona. Further transmission, reproduction or presentation (such as public display or performance) of protected items is prohibited except with permission of the author. Download date 06/10/2021 17:13:55 Link to Item http://hdl.handle.net/10150/196133 LAND TENURE REFORMS AND SOCIAL TRANSFORMATION IN BOTSWANA: IMPLICATIONS FOR URBANIZATION by Bayo Ijagbemi ____________________ Copyright © Bayo Ijagbemi 2006 A Dissertation Submitted to the Faculty of the DEPARTMENT OF ANTHROPOLOGY In Partial Fulfillment of the Requirements For the Degree of DOCTOR OF PHILOSOPHY In the Graduate College THE UNIVERSITY OF ARIZONA 2006 2 THE UNIVERSITY OF ARIZONA GRADUATE COLLEGE As members of the Dissertation Committee, we certify that we have read the dissertation prepared by Bayo Ijagbemi entitled “Land Reforms and Social Transformation in Botswana: Implications for Urbanization” and recommend that it be accepted as fulfilling the dissertation requirement for the Degree of Doctor of Philosophy _______________________________________________________________________ Date: 10 November 2006 Dr Thomas Park _______________________________________________________________________ Date: 10 November 2006 Dr Stephen Lansing _______________________________________________________________________ Date: 10 November 2006 Dr David Killick _______________________________________________________________________ Date: 10 November 2006 Dr Mamadou Baro Final approval and acceptance of this dissertation is contingent upon the candidate’s submission of the final copies of the dissertation to the Graduate College. I hereby certify that I have read this dissertation prepared under my direction and recommend that it be accepted as fulfilling the dissertation requirement. -

2011 Population & Housing Census Preliminary Results Brief
2011 Population & Housing Census Preliminary Results Brief For further details contact Census Office, Private Bag 0024 Gaborone: Tel 3188500; Fax 3188610 1. Botswana Population at 2 Million Botswana’s population has reached the 2 million mark. Preliminary results show that there were 2 038 228 persons enumerated in Botswana during the 2011 Population and Housing Census, compared with 1 680 863 enumerated in 2001. Suffice to note that this is the de-facto population – persons enumerated where they were found during enumeration. 2. General Comments on the Results 2.1 Population Growth The annual population growth rate 1 between 2001 and 2011 is 1.9 percent. This gives further evidence to the effect that Botswana’s population continues to increase at diminishing growth rates. Suffice to note that inter-census annual population growth rates for decennial censuses held from 1971 to 2001 were 4.6, 3.5 and 2.4 percent respectively. A close analysis of the results shows that it has taken 28 years for Botswana’s population to increase by one million. At the current rate and furthermore, with the current conditions 2 prevailing, it would take 23 years for the population to increase by another million - to reach 3 million. Marked differences are visible in district population annual growths, with estimated zero 3 growth for Selebi-Phikwe and Lobatse and a rate of over 4 percent per annum for South East District. Most district growth rates hover around 2 percent per annum. High growth rates in Kweneng and South East Districts have been observed, due largely to very high growth rates of villages within the proximity of Gaborone. -
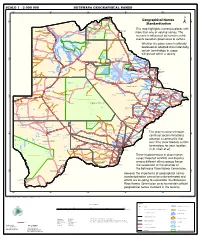
Geographical Names Standardization BOTSWANA GEOGRAPHICAL
SCALE 1 : 2 000 000 BOTSWANA GEOGRAPHICAL NAMES 20°0'0"E 22°0'0"E 24°0'0"E 26°0'0"E 28°0'0"E Kasane e ! ob Ch S Ngoma Bridge S " ! " 0 0 ' ' 0 0 ° Geographical Names ° ! 8 !( 8 1 ! 1 Parakarungu/ Kavimba ti Mbalakalungu ! ± n !( a Kakulwane Pan y K n Ga-Sekao/Kachikaubwe/Kachikabwe Standardization w e a L i/ n d d n o a y ba ! in m Shakawe Ngarange L ! zu ! !(Ghoha/Gcoha Gate we !(! Ng Samochema/Samochima Mpandamatenga/ This map highlights numerous places with Savute/Savuti Chobe National Park !(! Pandamatenga O Gudigwa te ! ! k Savu !( !( a ! v Nxamasere/Ncamasere a n a CHOBE DISTRICT more than one or varying names. The g Zweizwe Pan o an uiq !(! ag ! Sepupa/Sepopa Seronga M ! Savute Marsh Tsodilo !(! Gonutsuga/Gonitsuga scenario is influenced by human-centric Xau dum Nxauxau/Nxaunxau !(! ! Etsha 13 Jao! events based on governance or culture. achira Moan i e a h hw a k K g o n B Cakanaca/Xakanaka Mababe Ta ! u o N r o Moremi Wildlife Reserve Whether the place name is officially X a u ! G Gumare o d o l u OKAVANGO DELTA m m o e ! ti g Sankuyo o bestowed or adopted circumstantially, Qangwa g ! o !(! M Xaxaba/Cacaba B certain terminology in usage Nokaneng ! o r o Nxai National ! e Park n Shorobe a e k n will prevail within a society a Xaxa/Caecae/Xaixai m l e ! C u a n !( a d m a e a a b S c b K h i S " a " e a u T z 0 d ih n D 0 ' u ' m w NGAMILAND DISTRICT y ! Nxai Pan 0 m Tsokotshaa/Tsokatshaa 0 Gcwihabadu C T e Maun ° r ° h e ! 0 0 Ghwihaba/ ! a !( o 2 !( i ata Mmanxotae/Manxotae 2 g Botet N ! Gcwihaba e !( ! Nxharaga/Nxaraga !(! Maitengwe -

Constituency Athletics Competitions
MINISTRY OF YOUTH EMPOWERMENT SPORT AND CULTURE DEVELOPMENT RULES AND REGULATIONS FOR THE CONSTITUENCY ATHLETICS COMPETITIONS 2017/18 1 CONSTITUENCY ATHLETICS COMPETITIONS COMPETITION RULES AND REGULATIONS: 2017-18 PREAMBLE The Constituency Athletics Competitions is a mass participation programme funded by the Government of Botswana. Rules and Regulations are established to provide guidance and foster compliance to the competition to ensure fair and honesty. The competition shall occur under the auspices of the Ministry of Youth Empowerment, Sport & Culture Development in collaboration with Botswana Athletic Association (BAA). Any rights which are not ceded by these Regulations to any Constituency Athletics Club or individuals taking part in the Tournament shall be regulated alongside the BAA with the ownership belonging to the Ministry of Youth Empowerment, Sport and Culture Development. It should be noted that the word Club means Athletics Constituency Team. ARTICLE 1 – TITLE 1.1. The Constituency Athletics Competitions shall take place every financial year on a two (2) cycle with some break between the cycles 1.2. Constituency Athletics Competition shall be governed on a heat-final basis starting at District level in sprints, medium races and middle to long distances. 1.3. Competitions are to be held in accordance with the Rules and Regulations of the competition here contained, coordinated by various Committees established by Ministry of Youth Empowerment, Sport and Culture Development at Districts and Sub Districts. 1.4. Competitions shall be officiated by qualified/competent technical officials appointed by the Coordinating Committees with the guidance of a competent person. 2 ARTICLE 2: ELIGIBILITY 2.1. An athlete or team is eligible to compete in the competitions when he/she is registered with Ministry of Youth Empowerment, Sport and Culture Development at respective districts. -

Botswana. Supervisor of Elections. . Report to the Minister of State on the General Elections, 1974
Botswana. Supervisor of Elections. Report to the Minister of State on the general elections, 1974. Gaborone, Government Printer [1974?] / 30p. 29cm. 1. Botswana-Pol. & govt. 2. Elections- Botswana. I • INDEX Page. Report to the Minister of State on the General Elections, 1974 Evaluation and Recommendations *"* Conclusion ...... 2 - • • • • 4 Title Appendix lA' A list of Constituencies, Polling Districts and Polling Stations showing the number of registered voters by constituency and polling station Appendix '/?' Authenticating Officers appointed in accordance with the Presidential Elections (Supplementary Provisions) Act >;• 12 Appendix 'C A list of Returning Officers for the Parliamentary Elections • ! l 13 Appendix Z)' A list of Returning Officers for the Local Government Elections .. ^ . 14 Appendix 'ZT Summary of the Parliamentary election results Appendix lF 17 A list of candidates in the Parliamentary Election showing the number of votes cast for each, number of votes in each constituency, and the majority gained by the winning can- didate and the percentage poll 18 Appendix '6" Summary of Local Government Election results by District or Town Council 20 Appendix 'IT A list of candidates in the Local Government election showing the number of votes cast tor each, the number of voters in each Polling District, the majority gained by the win- ning candidate, and the percentage poll / 22 Appendix T A list of political Parries registered under Section 149 of the Electoral Act 1969 30 Appendix ' J" A Report on-expenditure on the 1974 General Election 30 Sir, REPORT TO ™E MINISTER. OF STATE ON THE GENERAL ELECTIONS, 1974 SSSITOSSS: S.»=^^HS£s~rr?' Lo^l Government Election* become generally available to the public - - - > »S5S^S^as: • l^^sstsss^aSSSS^5^^-^-"5 5. -

Rural Poverty in Botswana. University of Botswana
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Brage INN Gerd Wikan Cash, crops and cattle A study of rural livelihoods in Botswana Høgskolen i Hedmark Rapport nr. 7 - 2001 Online-versjon Utgivelsessted: Elverum Det må ikke kopieres fra rapporten i strid med åndsverkloven og fotografiloven eller i strid med avtaler om kopiering inngått med KOPINOR, interesseorgan for rettighetshavere til åndsverk. Forfatteren er selv ansvarlig for sine konklusjoner. Innholdet gir derfor ikke nødvendigvis uttrykk for Høgskolens syn. I rapportserien fra Høgskolen i Hedmark publiseres FoU-arbeid og utredninger. Dette omfatter kvalifiseringsarbeid, stoff av lokal og nasjonal interesse, oppdragsvirksomhet, foreløpig publisering før publisering i et vitenskapelig tidsskrift etc. Rapporten kan bestilles ved henvendelse til Høgskolen i Hedmark. (http://www.hihm.no/Publikasjon/default.htm) Rapport nr. 7 - 2001 © Forfatteren/Høgskolen i Hedmark ISBN: 82-7671-167-7 ISSN: 1501-8563 2 Title: Cash, crops and cattle. A study of rural livelihoods in Botswana Author: Gerd Wikan Number: 7 Year: 2001 Pages: 182 ISBN: 82-7671-167-7 ISSN: 1501-8563 Financed by: Hedmark College and The research council of Norway Keywords: Botswana, livelihoods, rural poverty, income strategy Summary: Lack of economic development has lead to a growing scepticism to grand economic development theories and strategies. The focus has shifted towards a more open-ended perspective where the local context and poverty alleviation are in focus. As a result, the new key concepts in the discourse are livelihoods and urban-rural linkages. The academic interest is focused on the question: how are African households surviving given their increasing difficult economic circumstances? In the African context, Botswana is a special case. -
Republic of Botswana the Project for Enhancing National Forest Monitoring System for the Promotion of Sustainable Natural Resource Management
DEPARTMENT OF FORESTRY AND RANGE RESOURCES (DFRR) MINISTRY OF ENVIRONMENT, NATURAL RESOURCES CONSERVATION AND TOURISM (MENT) REPUBLIC OF BOTSWANA REPUBLIC OF BOTSWANA THE PROJECT FOR ENHANCING NATIONAL FOREST MONITORING SYSTEM FOR THE PROMOTION OF SUSTAINABLE NATURAL RESOURCE MANAGEMENT PROJECT COMPLETION REPORT DECEMBER 2017 JAPAN INTERNATIONAL COOPERATION AGENCY(JICA) ORIENTAL CONSULTANTS GLOBAL CO., LTD. JAPAN FOREST TECHNOLOGY ASSOCIATION GE JR 17-131 DEPARTMENT OF FORESTRY AND RANGE RESOURCES (DFRR) MINISTRY OF ENVIRONMENT, NATURAL RESOURCES CONSERVATION AND TOURISM (MENT) REPUBLIC OF BOTSWANA REPUBLIC OF BOTSWANA THE PROJECT FOR ENHANCING NATIONAL FOREST MONITORING SYSTEM FOR THE PROMOTION OF SUSTAINABLE NATURAL RESOURCE MANAGEMENT PROJECT COMPLETION REPORT DECEMBER 2017 JAPAN INTERNATIONAL COOPERATION AGENCY(JICA) ORIENTAL CONSULTANTS GLOBAL CO., LTD. JAPAN FOREST TECHNOLOGY ASSOCIATION DFRR/JICA: Botswana Forest Distribution Map Zambia Angola Zambia Legend KASANE Angola ! ! Settlement CountryBoundary Riparian Forest Typical Forest Woodland Zimbabwe Zimbabwe Bushland/Shrubland Savanna/Grassland/Forbs MAUN ! NATA Baregorund ! TUTUME ! Desert/Sand Dunes Marsh/Wetland FRANCISTOWN Waterbody/Pan ! ORAPA Namibia ! TONOTA ! GHANZI Angola Zambia Namibia ! SELEBI-PHIKWE BOBONONG ! ! Zimbabwe SEROWE ! PALAPYE ! Namibia MAHALAPYE ! South Africa KANG ! MOLEPOLOLE MOCHUDI ! ! JWANENG ! GABORONE ! ´ 0 50 100 200 RAMOTSWA ! KANYE Kilometres ! Coordinate System: GCS WGS 1984 Datum: WGS 1984 LOBATSE ! Botswana Forest Distribution Map Produced from -

SABONET Report No 18
ii Quick Guide This book is divided into two sections: the first part provides descriptions of some common trees and shrubs of Botswana, and the second is the complete checklist. The scientific names of the families, genera, and species are arranged alphabetically. Vernacular names are also arranged alphabetically, starting with Setswana and followed by English. Setswana names are separated by a semi-colon from English names. A glossary at the end of the book defines botanical terms used in the text. Species that are listed in the Red Data List for Botswana are indicated by an ® preceding the name. The letters N, SW, and SE indicate the distribution of the species within Botswana according to the Flora zambesiaca geographical regions. Flora zambesiaca regions used in the checklist. Administrative District FZ geographical region Central District SE & N Chobe District N Ghanzi District SW Kgalagadi District SW Kgatleng District SE Kweneng District SW & SE Ngamiland District N North East District N South East District SE Southern District SW & SE N CHOBE DISTRICT NGAMILAND DISTRICT ZIMBABWE NAMIBIA NORTH EAST DISTRICT CENTRAL DISTRICT GHANZI DISTRICT KWENENG DISTRICT KGATLENG KGALAGADI DISTRICT DISTRICT SOUTHERN SOUTH EAST DISTRICT DISTRICT SOUTH AFRICA 0 Kilometres 400 i ii Trees of Botswana: names and distribution Moffat P. Setshogo & Fanie Venter iii Recommended citation format SETSHOGO, M.P. & VENTER, F. 2003. Trees of Botswana: names and distribution. Southern African Botanical Diversity Network Report No. 18. Pretoria. Produced by University of Botswana Herbarium Private Bag UB00704 Gaborone Tel: (267) 355 2602 Fax: (267) 318 5097 E-mail: [email protected] Published by Southern African Botanical Diversity Network (SABONET), c/o National Botanical Institute, Private Bag X101, 0001 Pretoria and University of Botswana Herbarium, Private Bag UB00704, Gaborone. -
A History of the Botswana Defence Force, C. 1977-2007
University of Calgary PRISM: University of Calgary's Digital Repository Graduate Studies The Vault: Electronic Theses and Dissertations 2021-01-11 Thebe ya Sechaba: A History of the Botswana Defence Force, c. 1977-2007 Mocheregwa, Bafumiki Mocheregwa, B. (2021). Thebe ya Sechaba: A History of the Botswana Defence Force, c. 1977-2007 (Unpublished doctoral thesis). University of Calgary, Calgary, AB. http://hdl.handle.net/1880/112986 doctoral thesis University of Calgary graduate students retain copyright ownership and moral rights for their thesis. You may use this material in any way that is permitted by the Copyright Act or through licensing that has been assigned to the document. For uses that are not allowable under copyright legislation or licensing, you are required to seek permission. Downloaded from PRISM: https://prism.ucalgary.ca UNIVERSITY OF CALGARY Thebe ya Sechaba: A History of the Botswana Defence Force, c. 1977 – 2007 by Bafumiki Mocheregwa A THESIS SUBMITTED TO THE FACULTY OF GRADUATE STUDIES IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILSOPHY GRADUATE PROGRAM IN HISTORY CALGARY, ALBERTA JANUARY, 2021 © Bafumiki Mocheregwa 2021 Abstract The protracted liberation struggles of Southern Africa that began in the 1960s, particularly in Rhodesia (Zimbabwe today) eventually prompted the Botswana government to establish its own defence force in 1977. Due to budgetary constraints and relative internal political stability, Botswana had relied on a small paramilitary force called the Police Mobile Unit (PMU) since the early 1960s for all defence – related issues. By the late 1970s, the sharp escalation of the struggle for Zimbabwe resulted in cross – border incursions by Rhodesian security forces who were pursuing armed freedom fighters. -

Notrufnummern Botswana
Notruf und Servicenummern Botswana Regional Carsten Möhle Internationale Vorwahl 00267, dann die "0" weglassen www.bwana.de [email protected] Genereller Notruf / Emergencies Internationale Vorwahl, dann die "0" weglassen und dann Ortsvorwahl und dann 999 Asternweg 4 Bei Ländervorwahl 00267 durch Mobiltelefone die "00" durch ein "+" -Zeichen ersetzen. D-25551 Hohenlockstedt Botswana Mobiltelefonnummern fangen mit "7"an Fon: 0049 4826 - 5208 SOS- International Emergency 24 Hour Control Center Flying Doctors +267 3901 601 +267 911 MedRescue Fax: 0049 4826 - 3371 Ort Polizei Polizei Ort Krankenhaus Krankenhaus Ort Telefon Werkstatt Werkstatt Ort Telefon Charleshill Engen Charleshill 659 2154 Francistown 241 2221 Haskins Street (Nord) Jubilee Hospital Haskins Street/New Maun Rd 241 2333 Toyota Francistown Straße Maun/Sam Nujoma 241 3855 Francistown 241 4204 Immigration Blue Jacket Nyanagabgwe Hospital Matsiloje Road 241 1000 4x4 Service Centre Industriegebiet West 241 3008 Francistown Pana Medical Clinic 241 5351 Landrover 241 6601 Francistown Dr. J.E. Cobbina Zahnärztin Baines Street 241 2295 B & S Motors And Steelworks 241 3944 Francistown Hana Pharmacy Blue Jacket Plaza 241 6026 Diesel Repair Centre Somerset East Ext 241 4374 Francistown Pharma North Pharmacy Blue Jacket Plaza 241 0877 J J Automotive Services Along Monarch Siding Bulawayo 241 6829 Francistown Kasane Motor And Tyres 241 2607 Francistown Midway Car & Truck Clinic Plot 5037 Somerset East Ext 241 0193 Francistown Mototech Botswana (pty) Ltd 240 4677 Gaborone 395 1161 Botswana Road