Climate Change Vulnerability Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
National Weather Service Reference Guide
National Weather Service Reference Guide Purpose of this Document he National Weather Service (NWS) provides many products and services which can be T used by other governmental agencies, Tribal Nations, the private sector, the public and the global community. The data and services provided by the NWS are designed to fulfill us- ers’ needs and provide valuable information in the areas of weather, hydrology and climate. In addition, the NWS has numerous partnerships with private and other government entities. These partnerships help facilitate the mission of the NWS, which is to protect life and prop- erty and enhance the national economy. This document is intended to serve as a reference guide and information manual of the products and services provided by the NWS on a na- tional basis. Editor’s note: Throughout this document, the term ―county‖ will be used to represent counties, parishes, and boroughs. Similarly, ―county warning area‖ will be used to represent the area of responsibility of all of- fices. The local forecast office at Buffalo, New York, January, 1899. The local National Weather Service Office in Tallahassee, FL, present day. 2 Table of Contents Click on description to go directly to the page. 1. What is the National Weather Service?…………………….………………………. 5 Mission Statement 6 Organizational Structure 7 County Warning Areas 8 Weather Forecast Office Staff 10 River Forecast Center Staff 13 NWS Directive System 14 2. Non-Routine Products and Services (watch/warning/advisory descriptions)..…….. 15 Convective Weather 16 Tropical Weather 17 Winter Weather 18 Hydrology 19 Coastal Flood 20 Marine Weather 21 Non-Precipitation 23 Fire Weather 24 Other 25 Statements 25 Other Non-Routine Products 26 Extreme Weather Wording 27 Verification and Performance Goals 28 Impact-Based Decision Support Services 30 Requesting a Spot Fire Weather Forecast 33 Hazardous Materials Emergency Support 34 Interactive Warning Team 37 HazCollect 38 Damage Surveys 40 Storm Data 44 Information Requests 46 3. -
SKYWARN Detailed Documentation
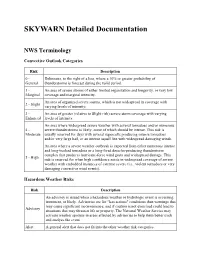
SKYWARN Detailed Documentation NWS Terminology Convective Outlook Categories Risk Description 0 - Delineates, to the right of a line, where a 10% or greater probability of General thunderstorms is forecast during the valid period. 1 - An area of severe storms of either limited organization and longevity, or very low Marginal coverage and marginal intensity. An area of organized severe storms, which is not widespread in coverage with 2 - Slight varying levels of intensity. 3 - An area of greater (relative to Slight risk) severe storm coverage with varying Enhanced levels of intensity. An area where widespread severe weather with several tornadoes and/or numerous 4 - severe thunderstorms is likely, some of which should be intense. This risk is Moderate usually reserved for days with several supercells producing intense tornadoes and/or very large hail, or an intense squall line with widespread damaging winds. An area where a severe weather outbreak is expected from either numerous intense and long-tracked tornadoes or a long-lived derecho-producing thunderstorm complex that produces hurricane-force wind gusts and widespread damage. This 5 - High risk is reserved for when high confidence exists in widespread coverage of severe weather with embedded instances of extreme severe (i.e., violent tornadoes or very damaging convective wind events). Hazardous Weather Risks Risk Description An advisory is issued when a hazardous weather or hydrologic event is occurring, imminent, or likely. Advisories are for "less serious" conditions than warnings that may cause significant inconvenience, and if caution is not exercised could lead to Advisory situations that may threaten life or property. The National Weather Service may activate weather spotters in areas affected by advisories to help them better track and analyze the event. -

Section 11 Mountrail County Hazard Identification and Risk Assessment, Capability Assessment, and Mitigation Strategy
Mountrail County, ND Hazard Mitigation Plan Update Section 11: Mountrail County: Hazard Identification and Risk Assessment, Capability Assessment, and Mitigation Strategy Section 11 Mountrail County Hazard Identification and Risk Assessment, Capability Assessment, and Mitigation Strategy 11.1 IFR for Hazard Identification and Risk Assessment 11.2 Hazard Identification (Updated) 11.2.1 Overview of Mountrail County’s History of Hazards and Potential Hazards 11.2.2 Hazard Profiles 11.3 Risk Assessment (Updated) 11.3.1 Risk Assessment Methodology 11.3.2 Risk and Vulnerability Assessment 11.4 Capability Assessment (Updated) 11.5 Mitigation Strategy (Updated) 11.5.1 Mitigation Goals 11.5.2 Mitigation Actions 11.1 Interim Final Rule for Hazard Identification and Risk Assessment Requirement §201.6(c)(2): The plan shall include a risk assessment that provides the factual basis for activities proposed in the strategy to reduce losses from identified hazards. Local risk assessments must provide sufficient information to enable the jurisdiction to identify and prioritize appropriate mitigation actions to reduce losses from identified hazards. Requirement §201.6(c)(2)(i): [The risk assessment shall include a] description of the type…location and extent of all natural hazards that can affect the jurisdiction. The plan shall include information on previous occurrences of hazard events and on the probability of future hazard events. Requirement §201.6(c)(2)(ii): [The risk assessment shall include a] description of the jurisdiction’s vulnerability to the hazards described in paragraph (c)(2)(i) of this section. This description shall include an overall summary of each hazard and its impact on the community. -

Nwa Newsletter
August 2016 No 16 - 8 NWA NEWSLETTER NWA Webinars Bring Better Science, Better Communication, Better Benefi ts for Members Trisha Palmer, NWA Councilor; NWA Professional Development Committee Chair Inside Jonathan Belles, Weather.com Digital Meteorologist 41st Annual Meeting: Did you know that the NWA hosts webinars each month? These webinars are offered free to NWA Special Events . 4 members, and they have been a great success! On the fi rst Wednesday of every month, a different Keynote Speaker . 6 NWA committee presents a webinar, up to an hour long, on a vast variety of meteorological topics and NWA programs. Meeting Sponsors . 6 General Info and Schedule . 7 In preparing for each monthly webinar, an ad-hoc team of planners and In Memory of Dave Schwartz . 2 technical support personnel including NWA Social Media . 2 Trisha Palmer (NWA Professional Development Committee Chair), Tim August President’s Message . 3 Brice (NWA Social Media Committee), New JOM Articles . 5 and Jonathan Belles collaborate with committees and their guests to create Chapter News: High Plains . 5 the best possible presentation of useful New NWA Members . 7 information. Assistance has been strong across the Association with dedicated Screenshot of NWA member Mike Mogil during the January New Seal Holders . 8 members including Greg Carbin, Frank webinar, “Planting MORE Micro-scale Forecasts” Alsheimer, Trevor Boucher, and Hulda Strategic Planning Committee . 9 Johannsdottir providing a great deal of service to this series. The webinars have been hosted on Professional Development and both GoToWebinar and Google Hangouts in order to extend benefi ts to as many people as possible Other Events . -
National Weather Service Reference Guide
National Weather Service Reference Guide Purpose of this Document he National Weather Service (NWS) provides many products and services which can be T used by other governmental agencies, Tribal Nations, the private sector, the public and the global community. The data and services provided by the NWS are designed to fulfill us- ers’ needs and provide valuable information in the areas of weather, hydrology and climate. In addition, the NWS has numerous partnerships with private and other government entities. These partnerships help facilitate the mission of the NWS, which is to protect life and prop- erty and enhance the national economy. This document is intended to serve as a reference guide and information manual of the products and services provided by the NWS on a na- tional basis. Editor’s note: Throughout this document, the term ―county‖ will be used to represent counties, parishes, and boroughs. Similarly, ―county warning area‖ will be used to represent the area of responsibility of all of- fices. The local forecast office at Buffalo, New York, January, 1899. The local National Weather Service Office in Tallahassee, FL, present day. 2 Table of Contents Click on description to go directly to the page. 1. What is the National Weather Service?…………………….………………………. 5 Mission Statement 6 Organizational Structure 7 County Warning Areas 8 Weather Forecast Office Staff 10 River Forecast Center Staff 13 NWS Directive System 14 2. Non-Routine Products and Services (watch/warning/advisory descriptions)..…….. 15 Convective Weather 16 Tropical Weather 17 Winter Weather 18 Hydrology 19 Coastal Flood 20 Marine Weather 21 Non-Precipitation 23 Fire Weather 24 Other 25 Statements 25 Other Non-Routine Products 26 Extreme Weather Wording 27 Verification and Performance Goals 28 Impact-Based Decision Support Services 30 Requesting a Spot Fire Weather Forecast 33 Hazardous Materials Emergency Support 34 Interactive Warning Team 37 HazCollect 38 Damage Surveys 40 Storm Data 44 Information Requests 46 3. -
CLIMATE CHANGE and PUBLIC HEALTH in GREY BRUCE HEALTH UNIT Current Conditions and Future Projections
CLIMATE CHANGE AND PUBLIC HEALTH IN GREY BRUCE HEALTH UNIT Current Conditions and Future Projections 2017 0 ABOUT THIS REPORT This report was completed as part of a Master of Public Health practicum placement by Gillian Jordan of Lakehead University during the summer of 2017 under the supervision of Robert Hart and Alanna Leffley of Grey Bruce Health Unit. Acknowledgements Much of this report was inspired by past work conducted by Stephen Lam, Krista Youngblood, and Dr. Ian Arra. This report is meant to build upon and accompany these previous reports to assist in furthering climate change-related understanding and planning of adaptation activities in Grey Bruce. Special thanks to Bob Hart and Alanna Leffley for their guidance and assistance throughout the report process; additional thanks to Virginia McFarland for her help with data analysis. Suggested Citation: Grey Bruce Health Unit. (2017). Climate Change and Public Health in Grey Bruce Health Unit: Current conditions and future projections. Owen Sound, Ontario. Grey Bruce Health Unit. 0 CONTENTS Table of Figures ............................................................................................................................................. ii Executive Summary ...................................................................................................................................... iii Introduction .................................................................................................................................................. 1 Climate Change -

Ensuring a Safe and Secure Homeland for All North Dakotans
■ Ensuring a safe and secure homeland for all North Dakotans ■ Winter Season - Watch The National Weather Service issues Watches when the risk of a hazardous winter weather event has increased, but the occurrence, location, and/or timing is still uncertain. Watches are issued to highlight significant and life threatening situations that may occur or are possible in the next several days. The significant winter weather could be heavy snow, freezing rain, sleet, blowing snow, extreme cold, blizzard, or combinations of these. Watches are issued for Winter Storms, Blizzards, and Extreme Cold, depending on what the threat is. Watches may be dropped (cancelled), or upgraded to advisories or warnings. ■ Winter Season - Warning The National Weather Service issues Warnings when life threatening winter weather is imminent, or occurring. Anytime you hear the National Weather Service has issued a Warning (winter or summer), you should be thinking of life threatening dangerous weather. There are four types of warnings issued for winter weather: Winter Storm Warning; Blizzard Warning; Ice Storm Warning; and Extreme Cold Warning. ■ Winter Storm Warning - 6 inches (or more) of snow is expected in a 12 hour (or less) period of time, OR, when 8 inches (or more) of snow is expected in a 24 hour (or less) period of time. Winter Storm Warnings may also be issued for combinations of snow, wind, blowing snow and dangerously cold conditions. ■ Blizzard Warning – (the most deadly winter events in North Dakota) –considerable falling and/or blowing snow combined with winds of 35 mph or more and reducing visibility to less than ¼ mile (near zero), and lasting at least 3 hours. -

Minnesota Weathertalk Newsletter for Friday, January 7Th, 2011
Minnesota WeatherTalk Newsletter for Friday, January 7th, 2011 To: MPR Morning Edition Crew From: Mark Seeley, University of Minnesota Extension Dept of Soil, Water, and Climate Subject: Minnesota WeatherTalk Newsletter for Friday, January 7th, 2011 Headlines: -Cold continues -Overlooked feature of 2010 weather -Experimental Extreme Cold Warning -Weekly Weather Potpourri -MPR listener question -Almanac for January 7th -Past weather features -Feeding storms -Outlook Topic: Cold continues to start 2011 Following a colder than normal December, January is continuing the pattern as mean temperatures are averaging 5 to 9 degrees F colder than normal through the first week of the month. Minnesota has reported the coldest temperature in the 48 contiguous states four times so far this month, the coldest being -33 degrees F at Bigfork on the 3rd. In fact several places including Bemidji, International Falls, Bigfork, Babbit, and Cass Lake have recorded -30 degrees F or colder already this month. Temperatures are expected to continue colder than normal well into the third week of the month, with perhaps some moderation in temperature and a January thaw during the last ten days of the month. Topic: Overlooked feature of 2010 weather In my write-up and radio comments of last week about significant weather in 2010 several people mentioned that I overlooked the flash flood event in southern Minnesota over September 22-23, 2010 affecting at least 19 counties. One of the largest flash floods in history, this storm produced rainfall amounts greater than 10 inches in some places (11.06 inches near Winnebago) and near record flood crests on many Minnesota watersheds. -

Sign up for Fond Du Lac Employee Emergency Alerts
EMPLOYEE EMERGENCY ALERT SIGN-UP INSTRUCTIONS – OPT-IN SIGN UP FOR FOND DU LAC EMPLOYEE EMERGENCY ALERTS First Name: Last Name: Middle Initial: Suffix: Registration Email: Username: Password: Please Select Your Security Question Please Circle What is your maternal Grandmother’s maiden name/ What is the City or Town where your Mother and Father met? What is the name of your favorite childhood friend? What is the city or town where you met your spouse/significant other? Where was your first job? What school did you attend in sixth grade? What was your childhood nickname? What street did you live on in third grade? What was the name of your favorite pet or stuffed animal? What was the last name of your favorite teacher? What is the city or town of your birth? Security Question Answer: Please List Order to Contact You 1st/2nd/3rd and so on. (You must list at least 2) How do you want to be alerted: ________Business Email:_________________________________________ ________Personal Email:_________________________________________ ________Work Phone:___________________________________________ ________Home Phone:__________________________________________ ________Cell Phone:____________________________________________ ________Text Message:__________________________________________ ________TTY:__________________________________________________ www.everbridge.com Weather & Hazard Alert Settings ____ Don’t contact me Between: Time _______ AM/PM & Time______AM/PM Alerts Subscriptions Signed Up For: Please Check the Alerts You Would Like to Recieve ____Weather -
Blizzards, Freezing Rain, and Ice Storms
Blizzards, freezing rain, and ice storms Overview Blizzards and blowing snow Blizzards, ice storms, high winds and blowing snow A blizzard warning is issued when falling or blowing can develop quickly and threaten life and property. snow, combined with 40 km/h winds, is expected for Severe storms occur frequently across Alberta and 4 hours or longer. Visibility is usually reduced to 400 can be unpredictable when they happen outside of metres or less. their regular season. A blowing snow advisory is issued when blowing snow combined with 30 km/h winds are expected for Be prepared 3 hours or longer and visibility is reduced to 800 Individuals and families should be prepared to take metres or less. care of themselves for at least 72 hours. The following steps will assist you in building your Blizzard facts preparedness plan. Blizzards can occur when there are clear skies. Know the risks: Knowing the risks and hazards In wide open areas, blowing snow or a blizzard can help you and your loved ones prepare for can mean zero visibility! the unexpected. Make a plan: A plan will help you cope with the Blizzard survival tips stress of an emergency or disaster. If you live in a rural area and a blizzard or blowing Build a kit: By taking a few simple steps you can snow is forecast, you may want to string a become better prepared to face a range of guideline between your house and any other emergencies. Be sure your kit includes a buildings you might have to go to during the battery-powered/crank radio/flashlight or storm. -

Page SASKATOON COLD WEATHER STRATEGY – 2020/21 EDITION
1 | P a g e SASKATOON COLD WEATHER STRATEGY – 2020/21 EDITION Contents Background ..................................................................................................................................................3 Principles ......................................................................................................................................................3 Cold Weather Alert ......................................................................................................................................4 Target Groups ..............................................................................................................................................4 Transportation .............................................................................................................................................4 Warm-Up Locations .....................................................................................................................................4 Communication ............................................................................................................................................4 Strategy Evaluation and Feedback ...............................................................................................................4 Members of the Cold Weather Strategy Committee ...................................................................................5 Become a Member of the Cold Weather Strategy Advisory Team ..............................................................5 -

Sky Watchers Teachers' Guide
Sky Watchers Teachers’ Guide Weather Resource Acknowledgements Project Management: Victoria Hudec (Outreach Officer: Ontario; SkyW atchers National Coordinator) Author and Custom Artwork: Nicole Lantz (Sprout Educational Consulting) Photography: George Lantz (Vision Photography), Victoria Hudec and iStock Diagrams: Nicole Lantz (Sprout Educational Consulting) Special thanks are extended to Julie Turner and Environment and Climate Change Canada staff across the country for the original Sky Watchers Guide to Weather. We would also like to thank the teachers, students, and educational psychologists in the Halifax Regional School Board and Colchester East-Hants Regional School Board for their input on publication design. Also, thanks to Hannah Thomas and Lisa Vitols for their assistance in the editing process. DISCLAIMER Her Majesty is not responsible for the accuracy or completeness of the information contained in the reproduced material. Her Majesty shall at all times be indemnified and held harmless against any and all claims whatsoever arising out of negli- gence or other fault in the use of the information contained in this publication or product. THIRD-PARTY MATERIALS Some of the information contained in this publication or product may be subject to copyrights held by other individuals or organizations. To obtain information concerning copyright ownership and restrictions, please contact: Environment and Climate Change Canada Public Inquiries Centre 7th Floor, Fontaine Building 200 Sacré-Coeur Boulevard Gatineau QC K1A 0H3 Telephone: 819-997-2800 Toll Free: 1-800-668-6767 (in Canada only) Email: [email protected] ISBN: En56-257/2015E-PDF Cat. No.: 978-0-660-02002-0 Sky Watchers Teachers’ Guide - Weather Resource Unless otherwise specified, you may not reproduce materials in this publication, in whole or in part, for the purposes of commercial redistribution without prior written permission from Environment and Climate Change Canada’s copyright administrator.