Seasonal Allergies in Children
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Caring for Children with Special Needs ALLERGIES and ASTHMA
caring for children with special needs ALLERGIES AND ASTHMA We don’t usually think of children with allergies or asthma as children with “special needs,” but they certainly are. In fact, children with these conditions are probably the most frequently encountered “special needs” children. Child care providers can do a great deal to help individual children manage their specific allergy or asthma needs and feel more comfortable in a child care setting. Allergies wastes. Every house has them, no matter how clean. Other inhaled Children with allergies face the allergens include mold, pollen (hay same social difficulties as do adults, fever), animal dander (especially but they have less maturity and from cats), chemicals, and per emotional resources to deal with fumes. them. Children find that they cannot eat what their friends eat or The most common allergy symp cannot play outside during some toms are seasons. Until a child is mature � a clear, runny nose and enough to understand why she sneezing, cannot do something, you must be � itchy or stuffed-up nose or careful to help the child through the itchy, runny eyes, and difficulties. Start teaching a child early on about what he is allergic to; � asthma (remember that not all you will not always be able to people with asthma have monitor everything. allergies and not all allergies Some foods can cause a life cause or develop into asthma). threatening reaction. The mouth, throat, and bronchial tubes swell enough to interfere with breathing. Strategies for inclusion The person may wheeze or faint. Some parents have found that by Often there are generalized hives volunteering to bring food to and/or a swollen face. -

Symptoms Related to Asthma and Chronic Bronchitis in Three Areas of Sweden
Eur Respir J, 1994, 7, 2146–2153 Copyright ERS Journals Ltd 1994 DOI: 10.1183/09031936.94.07122146 European Respiratory Journal Printed in UK - all rights reserved ISSN 0903 - 1936 Symptoms related to asthma and chronic bronchitis in three areas of Sweden E. Björnsson*, P. Plaschke**, E. Norrman+, C. Janson*, B. Lundbäck+, A. Rosenhall+, N. Lindholm**, L. Rosenhall+, E. Berglund++, G. Boman* Symptoms related to asthma and chronic bronchitis in three areas of Sweden. E. Björnsson, *Dept of Lung Medicine and Asthma P. Plaschke, E. Norrman, C. Janson, B. Lundbäck, A. Rosenhall, N. Lindholm, L. Research Center, Akademiska sjukhu- Rosenhall, E. Berglund, G. Boman. ERS Journals Ltd 1994. set, Uppsala University, Uppsala, Sweden. ABSTRACT: Does the prevalence of respiratory symptoms differ between regions? **Asthma and Allergy Research Center, Sahlgren's Hospital, University of Göteborg, As a part of the European Community Respiratory Health Survey, we present data Göteborg, Sweden. +Dept of Pulmonary from an international questionnaire on asthma symptoms occurring during a 12 Medicine and Allergology, Univer- month period, smoking and symptoms of chronic bronchitis. The questionnaire was sity Hospital of Northern Sweden, Umeå, mailed to 10,800 persons aged 20–44 yrs living in three regions of Sweden (Västerbotten, Sweden. ++Dept of Pulmonary Medicine, Uppsala and Göteborg) with different environmental characteristics. The total Sahlgrenska University Hospital, Göteborg, response rate was 86%. Sweden. Wheezing was reported by 20.5%, and the combination of wheezing without a Correspondence: E. Björnsson, Dept of cold and wheezing with breathlessness by 7.4%. The use of asthma medication was Lung Medicine, Akademiska sjukhuset, S- reported by 5.3%. -

Pediatric Institute & Cleveland Clinic Children's
Pediatric Institute & Cleveland Clinic Children’s This project would not have been possible without the commitment and expertise of a team led by Dr. Vera Hupertz, Anne Shi, and Allan Cohn. Graphic design and photography were provided by Cleveland Clinic’s Center for Medical Art and Photography. © The Cleveland Clinic Foundation 2017 9500 Euclid Avenue, Cleveland, OH 44195 clevelandclinic.org 2016 Outcomes 17-OUT-420 108373_CCFBCH_17OUT420_ACG.indd 1-3 9/7/17 1:42 PM Measuring Outcomes Promotes Quality Improvement Clinical Trials Cleveland Clinic is running more than 2200 clinical trials at any given time for conditions including breast and liver cancer, coronary artery disease, heart failure, epilepsy, Parkinson disease, chronic obstructive pulmonary disease, asthma, high blood pressure, diabetes, depression, and eating disorders. Cancer Clinical Trials is a mobile app that provides information on the more than 200 active clinical trials available to cancer patients at Cleveland Clinic. clevelandclinic.org/cancertrialapp Healthcare Executive Education Cleveland Clinic has programs to share its expertise in operating a successful major medical center. The Executive Visitors’ Program is an intensive, 3-day behind-the-scenes view of the Cleveland Clinic organization for the busy executive. The Samson Global Leadership Academy is a 2-week immersion in challenges of leadership, management, and innovation taught by Cleveland Clinic leaders, administrators, and clinicians. Curriculum includes coaching and a personalized 3-year leadership development plan. clevelandclinic.org/executiveeducation Consult QD Physician Blog A website from Cleveland Clinic for physicians and healthcare professionals. Discover the latest research insights, innovations, treatment trends, and more for all specialties. consultqd.clevelandclinic.org Social Media Cleveland Clinic uses social media to help caregivers everywhere provide better patient care. -
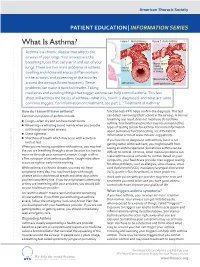
What Is Asthma? Figure 1
American Thoracic Society PATIENT EDUCATION | INFORMATION SERIES What Is Asthma? Figure 1. Normal Airway Figure 2. Acute Asthma Asthma is a chronic disease that affects the airways of your lungs. Your airways are the breathing tubes that carry air in and out of your Muscle spasm causing lungs. There are two main problems in asthma: relaxed narrowing muscles swelling and increased mucus (inflammation) of airways in the airways, and squeezing of the muscles Mucus build up around the airways (bronchospasm). These open airways Swelling/inammation problems can make it hard to breathe. Taking medicines and avoiding things that trigger asthma can help control asthma. This fact sheet will address the basics of asthma—what it is, how it is diagnosed, and what are some common triggers. For information on treatment, see part 2, “Treatment of Asthma”. How do I know if I have asthma? function test–PFT) helps confirm the diagnosis. This test Common symptoms of asthma include: can detect narrowing (obstruction) in the airways. A normal breathing test result does not mean you do not have ■ Cough—often dry and can have harsh bursts asthma. Your healthcare provider may recommend other ■ Wheezing—a whistling sound mainly when you breathe types of testing to look for asthma. For more information out through narrowed airways about pulmonary function testing, see ATS Patient ■ Chest tightness Information series at www.thoracic.org/patients. ■ Shortness of breath which may occur with activity or If you have been diagnosed with asthma, but it is not even at rest getting better with treatment, you might benefit from When you are having a problem with asthma, you may feel CLIP AND COPY AND CLIP seeing an asthma specialist. -

Allergic Bronchopulmonary Aspergillosis and Severe Asthma with Fungal Sensitisation
Allergic Bronchopulmonary Aspergillosis and Severe Asthma with Fungal Sensitisation Dr Rohit Bazaz National Aspergillosis Centre, UK Manchester University NHS Foundation Trust/University of Manchester ~ ABPA -a41'1 Severe asthma wl'th funga I Siens itisat i on Subacute IA Chronic pulmonary aspergillosjs Simp 1Ie a:spe rgmoma As r§i · bronchitis I ram une dysfu net Ion Lun· damage Immu11e hypce ractivitv Figure 1 In t@rarctfo n of Aspergillus Vliith host. ABP A, aHerg tc broncho pu~ mo na my as µe rgi ~fos lis; IA, i nvas we as ?@rgiH os 5. MANCHl·.'>I ER J:-\2 I Kosmidis, Denning . Thorax 2015;70:270–277. doi:10.1136/thoraxjnl-2014-206291 Allergic Fungal Airway Disease Phenotypes I[ Asthma AAFS SAFS ABPA-S AAFS-asthma associated with fu ngaIsensitization SAFS-severe asthma with funga l sensitization ABPA-S-seropositive a llergic bronchopulmonary aspergi ll osis AB PA-CB-all ergic bronchopulmonary aspergi ll osis with central bronchiectasis Agarwal R, CurrAlfergy Asthma Rep 2011;11:403 Woolnough K et a l, Curr Opin Pulm Med 2015;21:39 9 Stanford Lucile Packard ~ Children's. Health Children's. Hospital CJ Scanford l MEDICINE Stanford MANCHl·.'>I ER J:-\2 I Aspergi 11 us Sensitisation • Skin testing/specific lgE • Surface hydroph,obins - RodA • 30% of patients with asthma • 13% p.atients with COPD • 65% patients with CF MANCHl·.'>I ER J:-\2 I Alternar1a• ABPA •· .ABPA is an exagg·erated response ofthe imm1une system1 to AspergUlus • Com1pUcatio n of asthm1a and cystic f ibrosis (rarell·y TH2 driven COPD o r no identif ied p1 rior resp1 iratory d isease) • ABPA as a comp1 Ucation of asth ma affects around 2.5% of adullts. -

Diseases of the Respiratory System (J00-J99) ICD-10-CM
Diseases of the Respiratory System (J00-J99) ICD-10-CM Coverage provided by Amerigroup Inc. This publication contains proprietary information. This material is for informational purposes only. Reference the Centers for Medicare and Medicaid Services (CMS) for more information on Risk Adjustment and the CMS-HCC Model. Redistribution or other use is strictly forbidden This publication is for informational purposes only and is not guaranteed to be without defect. Please reference the current version(s) of the ICD-10-CM codebook, CMS-HCC Risk Adjustment Model, and AHA Coding Clinic for complete code sets and official coding guidance. AGPCARE-0080-19 63321MUPENABS 10/05/16 Diseases of the respiratory system are located in chapter Intermittent asthma which is defined as less 10 of the ICD-10-CM code book; this chapter includes than or equal to two occurrences per week. conditions such as asthma, pneumonia, and chronic Persistent asthma which includes three levels obstructive pulmonary disease (COPD). of severity: Mild: more than two times per week Reporting respiratory conditions Moderate: daily and may restrict Codes for reporting diseases of the respiratory physical activity system in ICD-10-CM feature relatively minor Severe: throughout the day with changes from ICD-9-CM. Most of the changes recurrent severe attacks limiting the involve understanding the medical terminology that ability to breathe the more specific codes include, as well as, the new The fourth character indicates severity, and the general coding structure and rules. fifth identifies whether status asthmaticus or At the beginning of chapter 10 for “Diseases of exacerbation is present. the Respiratory System (J00-J99),” an instructional note states, “When a respiratory condition is Asthma ICD-10-CM description described as occurring in more than one site and Category J45 Asthma is not specifically indexed, it should be classified Includes: to the lower anatomic site.” For example, Allergic: tracheobronchitis is classified to bronchitis with Asthma code J40. -

Increasing Prevalence of Bronchial Hyperresponsiveness in Three Selected Areas in East Germany
Copyright #ERS Journals Ltd 2001 Eur Respir J 2001; 18: 451–458 European Respiratory Journal Printed in UK – all rights reserved ISSN 0903-1936 Increasing prevalence of bronchial hyperresponsiveness in three selected areas in East Germany C. Frye*, J. Heinrich*, M. Wjst*, H-E. Wichmann*,#, for the Bitterfeld study group Increasing prevalence of bronchial hyperresponsiveness in three selected areas in East *GSF - Forschungszentrum fu¨r Um- Germany. C. Frye, J. Heinrich, M. Wjst, H-E. Wichmann, for the Bitterfeld study welt und Gesundheit, Institut fur # Epidemiologie, Ingolstaedter Land- group. ERS Journals Ltd 2001. # ABSTRACT: The prevalence of asthma, bronchial hyperresponsiveness (BHR) and strabe 1, Neuherberg, Germany. Lehr- stuhl fu¨r Epidemiologie, Institut fu¨r allergic rhinitis in children was lower in East Germany compared to West Germany. medizinische Informationsverarbei- The reasons for this difference are still not understood. This study tested the hypothesis tung, Biometrie und Epidemiologie that prevalence of BHR increased in East German children after reunification. der Ludwig-Maximilians-Universita¨t Two consecutive cross-sectional surveys of schoolchildren aged 8–14 yrs from three Mu¨nchen, Neuherberg, Germany. communities in East Germany were carried out in 1992–1993 and 1995–1996. A subsample of 530 and 790 children with complete lung function and cold air challenge Correspondence: J. Heinrich, GSF - data was analysed. Forschungszentrum fu¨r Umwelt und The prevalence of BHR increased from 6.4% in 1992–1993 to 11.6% in 1995–1996 Gesundheit, Institut fur Epidemiologie, Ingolstaedter Landstrabe 1, D-85764 (odds ratio (OR): 2.0, 95% confidence interval (CI): 1.3–3.0, adjusted for age, sex, Neuherberg, Germany. -

Environmental Determinants of Allergy and Asthma in Early Life
Clinical reviews in allergy and immunology Environmental determinants of allergy and asthma in early life Allison J. Burbank, MD,* Amika K. Sood, MD,* Matthew J. Kesic, PhD, David B. Peden, MD, MS, and Michelle L. Hernandez, MD Chapel Hill, NC INFORMATION FOR CATEGORY 1 CME CREDIT Credit can now be obtained, free for a limited time, by reading the review List of Design Committee Members: Allison J. Burbank, MD, Amika articles in this issue. Please note the following instructions. K. Sood, MD, Matthew J. Kesic, PhD, David B. Peden, MD, MS, and Mi- Method of Physician Participation in Learning Process: The core ma- chelle L. Hernandez, MD terial for these activities can be read in this issue of the Journal or online at Disclosure of Significant Relationships with Relevant Commercial the JACI Web site: www.jacionline.org. The accompanying tests may only Companies/Organizations: M. L. Hernandez has received grants from be submitted online at www.jacionline.org. Fax or other copies will not be the American Academy of Allergy, Asthma & Immunology Foundation. accepted. The rest of the authors declare that they have no relevant conflicts of interest. Date of Original Release: July 2017. Credit may be obtained for these Activity Objectives: courses until June 30, 2018. 1. To describe the effect of microbial exposure and childhood infec- Ó Copyright Statement: Copyright 2017-2018. All rights reserved. tions on the risk of allergic disease. Overall Purpose/Goal: To provide excellent reviews on key aspects 2. To understand the link between indoor allergen exposure and the risk of allergic disease to those who research, treat, or manage allergic of atopy. -

Food Allergy in Children and Young People Diagnosis and Assessment of Food Allergy in Children and Young People in Primary Care and Community Settings
Issue date: February 2011 Food allergy in children and young people Diagnosis and assessment of food allergy in children and young people in primary care and community settings NICE clinical guideline 116 Developed by the Centre for Clinical Practice at NICE Update information Minor changes since publication October 2018: After a surveillance review, links to other NICE guidance have been updated as needed and new links added in some recommendations. Some terminology has also been updated. These changes can be seen in the short version of the guideline at http://www.nice.org.uk/guidance/cg116 NICE clinical guidelines are recommendations about the treatment and care of people with specific diseases and conditions in the NHS in England and Wales. This guidance represents the view of NICE, which was arrived at after careful consideration of the evidence available. Healthcare professionals are expected to take it fully into account when exercising their clinical judgement. However, the guidance does not override the individual responsibility of healthcare professionals to make decisions appropriate to the circumstances of the individual patient, in consultation with the patient and/or guardian or carer, and informed by the summary of product characteristics of any drugs they are considering. Implementation of this guidance is the responsibility of local commissioners and/or providers. Commissioners and providers are reminded that it is their responsibility to implement the guidance, in their local context, in light of their duties to avoid unlawful discrimination and to have regard to promoting equality of opportunity. Nothing in this guidance should be interpreted in a way that would be inconsistent with compliance with those duties. -

Allergic Bronchopulmonary Aspergillosis: a Perplexing Clinical Entity Ashok Shah,1* Chandramani Panjabi2
Review Allergy Asthma Immunol Res. 2016 July;8(4):282-297. http://dx.doi.org/10.4168/aair.2016.8.4.282 pISSN 2092-7355 • eISSN 2092-7363 Allergic Bronchopulmonary Aspergillosis: A Perplexing Clinical Entity Ashok Shah,1* Chandramani Panjabi2 1Department of Pulmonary Medicine, Vallabhbhai Patel Chest Institute, University of Delhi, Delhi, India 2Department of Respiratory Medicine, Mata Chanan Devi Hospital, New Delhi, India This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. In susceptible individuals, inhalation of Aspergillus spores can affect the respiratory tract in many ways. These spores get trapped in the viscid spu- tum of asthmatic subjects which triggers a cascade of inflammatory reactions that can result in Aspergillus-induced asthma, allergic bronchopulmo- nary aspergillosis (ABPA), and allergic Aspergillus sinusitis (AAS). An immunologically mediated disease, ABPA, occurs predominantly in patients with asthma and cystic fibrosis (CF). A set of criteria, which is still evolving, is required for diagnosis. Imaging plays a compelling role in the diagno- sis and monitoring of the disease. Demonstration of central bronchiectasis with normal tapering bronchi is still considered pathognomonic in pa- tients without CF. Elevated serum IgE levels and Aspergillus-specific IgE and/or IgG are also vital for the diagnosis. Mucoid impaction occurring in the paranasal sinuses results in AAS, which also requires a set of diagnostic criteria. Demonstration of fungal elements in sinus material is the hall- mark of AAS. -

Right Heart Pressures in Bronchial Asthma
Thorax: first published as 10.1136/thx.26.1.39 on 1 January 1971. Downloaded from Thorax (1971), 26, 39. Right heart pressures in bronchial asthma R. F. GUNSTONE St. George's Hospital, London S.W.1 Right heart pressures, electrocardiograms, blood gases, and peak expiratory flow rates were measured in nine patients admitted to hospital with severe bronchial asthma. Low or normal right heart pressures were found despite electrocardiographic changes in five patients consisting of right atrial P waves, abnormal right axis deviation, and in one patient T-wave changes in pre- cordial leads. These electrocardiographic changes reverted towards normal on recovery of the patient from the asthmatic attack. Electrocardiographic changes suggestive of right The procedure was carried out in the general ward heart embarrassment have been noted in acute with the patient in the sitting position supported at 60 bronchial asthma, particularly right atrial P waves to 90 degrees to the horizontal because orthopnoea (P and abnormal right axis deviation was always present. Immediately after catheterization pulmonale) the peak expiratory flow rate was measured with a (Harkavy and Romanoff, 1942; Miyamato, Wright peak flow meter (Wright and McKerrow, Bastaroli, and Hoffman, 1961; Ambiavagar, 1959) and blood (capillary or arterial) was taken for Jones and Roberts, 1967). These observations measurement of pH, Pco2, and standard bicarbonate raise the possibility that death in bronchial asthma by the Astrup method (Astrup, J0rgensen, Andersen, may be due to acute cor pulmonale although and Engel, 1960). The peak flow rate and electro- copyright. necropsy evidence is against this suggestion (Earle, cardiogram were repeated after recovery. -

What You Need to Know About the New Guidelines for the Diagnosis and Management of Food Allergy in the U.S
Allergy guidelines insert_Layout 1 9/26/11 1:36 PM Page 1 What you need to know about the new guidelines for the diagnosis and management of food allergy in the U.S. V OLUME 126, N O . 6 D ECEMBER 2010 • Tests for food-specific IgE are recom- Overview www.jacionline.org • The Guidelines, sponsored by the NIH Supplement to mended to assist in diagnosis, but should (NIAID), are based upon expert opinion THE JOURNAL OF not be relied upon as a sole means to di- Allergy ANDClinical and a comprehensive literature review. Immunology agnose food allergy. The medical history/ AAP had input on the document.1,2 exam are recommended to aid in diag- nosis. A medically monitored feeding Guidelines for the Diagnosis and Management Definitions of Food Allergy in the United States: Report of the (food challenge) is considered the most NIAID-Sponsored Expert Panel • Food allergy was defined as an adverse definitive test for food allergy. health effect arising from a specific im- • Food-specific IgE testing has numerous mune response. limitations; positive tests are not intrin- • Food allergies result in IgE-mediated sically diagnostic and reactions some- immediate reactions (e.g., anaphylaxis) OFFICIAL JOURNAL OF times occur with negative tests. These and several chronic diseases (e.g., ente- Supported by the Food Allergy Initiative issues are also reviewed in an AAP Clini - rocolitis syndromes, eosinophilic esopha - cal Report.3 Testing “food panels” with- gitis, etc), in which IgE may not play an important role. out considering history is often mis - leading. Tests selected to evaluate food allergy should be Epidemiology and Natural History based on the patient’s medical history and not comprise • Food allergy is more common in children than adults, large general panels of food allergens.