Mechanics of Breathing (Pulmonary Ventilation)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
17 the Respiratory System
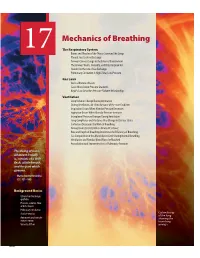
Mechanics of Breathing The Respiratory System 17 Bones and Muscles of the Thorax Surround the Lungs Pleural Sacs Enclose the Lungs Airways Connect Lungs to the External Environment The Airways Warm, Humidify, and Filter Inspired Air Alveoli Are the Site of Gas Exchange Pulmonary Circulation Is High-Flow, Low-Pressure G a s L a w s Air Is a Mixture of Gases Gases Move Down Pressure Gradients Boyle’s Law Describes Pressure-Volume Relationships Ventilation Lung Volumes Change During Ventilation During Ventilation, Air Flows Because of Pressure Gradients Inspiration Occurs When Alveolar Pressure Decreases Expiration Occurs When Alveolar Pressure Increases Intrapleural Pressure Changes During Ventilation Lung Compliance and Elastance May Change in Disease States Surfactant Decreases the Work of Breathing Airway Diameter Determines Airway Resistance Rate and Depth of Breathing Determine the Effi ciency of Breathing Gas Composition in the Alveoli Varies Little During Normal Breathing Ventilation and Alveolar Blood Flow Are Matched Auscultation and Spirometry Assess Pulmonary Function This being of mine, whatever it really is, consists of a little fl esh, a little breath, and the part which governs. — Marcus Aurelius Antoninus ( C . E . 121–180) Background Basics Ciliated and exchange epithelia Pressure, volume, fl ow, and resistance Pulmonary circulation Surface tension Colored x-ray of the lung Autonomic and somatic showing the motor neurons branching Velocity of fl ow airways. 600 Mechanics of Breathing magine covering the playing surface of a racquetball court cavity to control their contact with the outside air. Internalization (about 75 m2 ) with thin plastic wrap, then crumpling up the creates a humid environment for the exchange of gases with the wrap and stuffi ng it into a 3-liter soft drink bottle. -
Unit 11 Sound Speed of Sound Speed of Sound Sound Can Travel Through Any Kind of Matter, but Not Through a Vacuum
Unit 11 Sound Speed of Sound Speed of Sound Sound can travel through any kind of matter, but not through a vacuum. The speed of sound is different in different materials; in general, it is slowest in gases, faster in liquids, and fastest in solids. The speed depends somewhat on temperature, especially for gases. vair = 331.0 + 0.60T T is the temperature in degrees Celsius Example 1: Find the speed of a sound wave in air at a temperature of 20 degrees Celsius. v = 331 + (0.60) (20) v = 331 m/s + 12.0 m/s v = 343 m/s Using Wave Speed to Determine Distances At normal atmospheric pressure and a temperature of 20 degrees Celsius, speed of sound: v = 343m / s = 3.43102 m / s Speed of sound 750 mi/h Speed of light 670 616 629 mi/h c = 300,000,000m / s = 3.00 108 m / s Delay between the thunder and lightning Example 2: The thunder is heard 3 seconds after the lightning seen. Find the distance to storm location. The speed of sound is 345 m/s. distance = v t = (345m/s)(3s) = 1035m Example 3: Another phenomenon related to the perception of time delays between two events is an echo. In a canyon, an echo is heard 1.40 seconds after making the holler. Find the distance to the canyon wall (v=345m/s) distanceround trip = vt = (345 m/s )( 1.40 s) = 483 m d= 484/2=242m Applications: Sonar, Ultrasound, and Medical Imaging • Ultrasound or ultrasonography is a medical imaging technique that uses high frequency sound waves and their echoes. -

Atmospheric Cold Front-Generated Waves in the Coastal Louisiana
Journal of Marine Science and Engineering Article Atmospheric Cold Front-Generated Waves in the Coastal Louisiana Yuhan Cao 1 , Chunyan Li 2,* and Changming Dong 1,3,* 1 School of Marine Sciences, Nanjing University of Information Science and Technology, Nanjing 210044, China; [email protected] 2 Department of Oceanography and Coastal Sciences, College of the Coast and Environment, Louisiana State University, Baton Rouge, LA 70803, USA 3 Southern Laboratory of Ocean Science and Engineering (Zhuhai), Zhuhai 519000, China * Correspondence: [email protected] (C.L.); [email protected] (C.D.); Tel.: +1-225-578-2520 (C.L.); +86-025-58695733 (C.D.) Received: 15 October 2020; Accepted: 9 November 2020; Published: 11 November 2020 Abstract: Atmospheric cold front-generated waves play an important role in the air–sea interaction and coastal water and sediment transports. In-situ observations from two offshore stations are used to investigate variations of directional waves in the coastal Louisiana. Hourly time series of significant wave height and peak wave period are examined for data from 2004, except for the summer time between May and August, when cold fronts are infrequent and weak. The intra-seasonal scale variations in the wavefield are significantly affected by the atmospheric cold frontal events. The wave fields and directional wave spectra induced by four selected cold front passages over the coastal Louisiana are discussed. It is found that significant wave height generated by cold fronts coming from the west change more quickly than that by other passing cold fronts. The peak wave direction rotates clockwise during the cold front events. -
Respiratory Block Physiology 439 Team Work
Mechanics of pulmonary ventilation Respiratory Block Physiology 439 team work •Black: in male / female slides •Red : important Editing file •Pink: in female slides only •Blue: in male slides only •Green: notes @physiology439 •Gray: extra information •Textbook: Guyton + Linda Objectives : List the muscles of respiration and describe their roles during inspiration 01 and expiration Identify the importance of the following pressure in respiration: atmospheric, 02 intra-alveolar, intrapleural and transpulmonary Explain why intrapleural pressure is always subatmospheric under normal 03 conditions, and the significance of the thin layer of the intrapleural fluid surrounding the lung Define lung compliance and list the determinants of compliance 04 Mechanics of breathing Air movement depends upon : Boyle’s Law: Pulmonary Ventilation : the Volume depends on physical movement of air into PxV=K 1 2 P1xV1=P2xV2 3 movement of diaphragm and out of the lungs and ribs P= pressure , V= volume, K= constant Respiratory muscles Inspiratory muscle Expiratory muscle It is a passive process that depends on During resting Diaphragm and external intercostal the recoil tendency of the lung and need no muscle contraction Accessory muscles e.g It is an active process and need muscles Sternomastoid, anterior serratus, scalene During forced contraction the abdominal muscles and muscles contract in addition to the the internal intercostal muscles muscles of resting inspiration During deep forceful inhalation accessory muscles of inspiration -Expiration during forceful -

A Review of Ocean/Sea Subsurface Water Temperature Studies from Remote Sensing and Non-Remote Sensing Methods
water Review A Review of Ocean/Sea Subsurface Water Temperature Studies from Remote Sensing and Non-Remote Sensing Methods Elahe Akbari 1,2, Seyed Kazem Alavipanah 1,*, Mehrdad Jeihouni 1, Mohammad Hajeb 1,3, Dagmar Haase 4,5 and Sadroddin Alavipanah 4 1 Department of Remote Sensing and GIS, Faculty of Geography, University of Tehran, Tehran 1417853933, Iran; [email protected] (E.A.); [email protected] (M.J.); [email protected] (M.H.) 2 Department of Climatology and Geomorphology, Faculty of Geography and Environmental Sciences, Hakim Sabzevari University, Sabzevar 9617976487, Iran 3 Department of Remote Sensing and GIS, Shahid Beheshti University, Tehran 1983963113, Iran 4 Department of Geography, Humboldt University of Berlin, Unter den Linden 6, 10099 Berlin, Germany; [email protected] (D.H.); [email protected] (S.A.) 5 Department of Computational Landscape Ecology, Helmholtz Centre for Environmental Research UFZ, 04318 Leipzig, Germany * Correspondence: [email protected]; Tel.: +98-21-6111-3536 Received: 3 October 2017; Accepted: 16 November 2017; Published: 14 December 2017 Abstract: Oceans/Seas are important components of Earth that are affected by global warming and climate change. Recent studies have indicated that the deeper oceans are responsible for climate variability by changing the Earth’s ecosystem; therefore, assessing them has become more important. Remote sensing can provide sea surface data at high spatial/temporal resolution and with large spatial coverage, which allows for remarkable discoveries in the ocean sciences. The deep layers of the ocean/sea, however, cannot be directly detected by satellite remote sensors. -

Physical Geography Chapter 5: Atmospheric Pressure, Winds, Circulation Patterns
Physical Geography Chapter 5: Atmospheric Pressure, Winds, Circulation Patterns Torricelli – 1643- first Mercury barometer (76 cm, 29.92 in) – measures response to pressure Pressure – millibars- 1013.2 mb, will cause Hg to rise in tube Unequal heating of Earth’s surface is responsible for differences in pressure to! Variations in Atmospheric Pressure 1. Vertical Variations – increase in elevation, less air pressure Mt. Everest – 8848 m (or 29, 028 ft) – 1/3 pressure 2. Horizontal Variations a. Thermal (determined by T) Warm air is less dense – it rises away from the surface at the equator b. Dynamic: Air from the tropics moves northward and then to the east due to the Coryolis Effect. It collects at this latitude, increasing pressure at the surface. Basic Pressure Systems 1. Low – cyclone – converging air pressure decreases 2. High – anticyclone – Divergins air pressure increases Wind Isobars- line of equal pressure Pressure Gradient - significant difference in pressure Wind- horizontal movement of air in response to differences in pressure ¾ Responsible for moving heat toward poles ¾ 38° Lat and lower: radiation surplus If Earth did not rotate, and if there wasno friction between moving air and the Earth’s surface, the air would flow in a straight line from areas of higher pressure to areas of low pressure. Of course, this is not true, the Earth rotates and friction exists: and wind is controlled by three major factors: 1) PGF- Pressure is measured by barometer 2) Coriolis Effect 3) Friction 1) Pressure Gradient Force (PGF) Pressure differences create wind, and the greater these differences, the greater the wind speed. -

Dynamic Mechanics of the Lung Answer to the Last Class’S Question
Dynamic mechanics of the lung Answer to the Last class’s question Resistive (Frictional Forces) Opposing Lung Inflation Frictional opposition occurs only when the system is in motion. Frictional opposition to ventilation has the two components: 1. tissue viscous resistance 2. airway resistance. Tissue Viscous Resistance: the impedance of motion (opposition to flow) caused by displacement of tissues during ventilation that includes the lungs, rib cage, diaphragm, and abdominal organs. The frictional resistance is generated by the movement of each organ surface sliding against the other (e.g., the lung lobes sliding against each other and against the chest wall). Tissue resistance accounts for only approximately 20% of the total resistance to lung inflation. In conditions : obesity, pleural fibrosis, and ascites, the tissue viscous resistance increases the total impedance to ventilation. Airway Resistance (flow resistance) - Resistance to ventilation by the movement of gas through the airways. • accounts for approximately 80% of the frictional resistance to ventilation. • -is usually expressed in units of cm H2O/L/sec: R= ∆P/ ∆V • Airway resistance in healthy adults ranges from approximately 0.5 to 2.5 cm H2O/L/sec. • To cause gas to flow into or out of the lungs at 1 L/sec, a healthy person needs to lower his alveolar pressure 0.5 to 2.5 cm H2O below atmospheric pressure. Measurement of Airway Resistance • Airway resistance is the pressure difference between the alveoli and the mouth divided by a flow rate. Mouth pressure is easily measured with a manometer. Alveolar pressure can be deduced from measurements made in a body plethysmograph. -

Respiratory Physiology.Pdf
Respiratory Physiology • Chapter Outline • Functions of Respiratory System • Organization of Respiratory system • Ventilation and Lung mechanics: Boyle’s Law, Surfactant • 5-steps of respiration: Ventilation, external respiration, transport in blood, internal respiration and utilization of O2 and production of CO2 in cells • Lung volumes and capacities • Anatomical Dead Space • Hemoglobin and transport of gases • Oxygen Hemoglobin dissociation curve • Regulation of breathing: chemoreceptors and breathing center • Lung diseases • Main Functions of Respiratory System • Supplies O2 and removes CO2 • Joins kidney to Regulate pH of blood • Produces sounds for speech • Defends against microbes • Traps and dissolves systemic blood clots • Organization of Respiratory system • Has 3 portions: • Upper Airways: external nares nasal cavity nasopharynx oropharynx laryngopharynx larynx • Conducting zone: trachea bronchi bronchioles terminal bronchioles • Respiratory Zone: respiratory bronchioles alveolar ducts alveoli (main portion of gas exchange) • Conducting zone • Provides a low resistance path to alveoli • Bronchioles are the main site of air flow regulation by ANS and hormones. Bronchodilation versus bronchoconstriction. • Macrophages, mucous and cilia lining it defend against microbes and harmful particles • Epithelium secretes a watery fluid for easy movement of mucous. Cystic Fibrosis is genetic disease in which patient fails to secrete watery fluid and mucous narrows down the airways. • In chronic smokers cilia get damaged leading to mucous accumulation and chronic coughing • Respiratory zone • Main site of exchange of gases is Alveoli = air sacs • Each alveolus is surrounded by large # of pulmonary capillaries. Gases need to pass through 1 layer of very flat alveolar cells and 1 layer of endothelium of capillary wall • Type 1 Alveolar cells: very flat form main wall • Type 2 Alveolar cells: are thick cells and secrete detergent like Surfactant that prevents lung alveoli from collapsing. -

Diving Air Compressor - Wikipedia, the Free Encyclopedia Diving Air Compressor from Wikipedia, the Free Encyclopedia
2/8/2014 Diving air compressor - Wikipedia, the free encyclopedia Diving air compressor From Wikipedia, the free encyclopedia A diving air compressor is a gas compressor that can provide breathing air directly to a surface-supplied diver, or fill diving cylinders with high-pressure air pure enough to be used as a breathing gas. A low pressure diving air compressor usually has a delivery pressure of up to 30 bar, which is regulated to suit the depth of the dive. A high pressure diving compressor has a delivery pressure which is usually over 150 bar, and is commonly between 200 and 300 bar. The pressure is limited by an overpressure valve which may be adjustable. A small stationary high pressure diving air compressor installation Contents 1 Machinery 2 Air purity 3 Pressure 4 Filling heat 5 The bank 6 Gas blending 7 References 8 External links A small scuba filling and blending station supplied by a compressor and Machinery storage bank Diving compressors are generally three- or four-stage-reciprocating air compressors that are lubricated with a high-grade mineral or synthetic compressor oil free of toxic additives (a few use ceramic-lined cylinders with O-rings, not piston rings, requiring no lubrication). Oil-lubricated compressors must only use lubricants specified by the compressor's manufacturer. Special filters are used to clean the air of any residual oil and water(see "Air purity"). Smaller compressors are often splash lubricated - the oil is splashed around in the crankcase by the impact of the crankshaft and connecting A low pressure breathing air rods - but larger compressors are likely to have a pressurized lubrication compressor used for surface supplied using an oil pump which supplies the oil to critical areas through pipes diving at the surface control point and passages in the castings. -

Air Pressure and Wind
Air Pressure We know that standard atmospheric pressure is 14.7 pounds per square inch. We also know that air pressure decreases as we rise in the atmosphere. 1013.25 mb = 101.325 kPa = 29.92 inches Hg = 14.7 pounds per in 2 = 760 mm of Hg = 34 feet of water Air pressure can simply be measured with a barometer by measuring how the level of a liquid changes due to different weather conditions. In order that we don't have columns of liquid many feet tall, it is best to use a column of mercury, a dense liquid. The aneroid barometer measures air pressure without the use of liquid by using a partially evacuated chamber. This bellows-like chamber responds to air pressure so it can be used to measure atmospheric pressure. Air pressure records: 1084 mb in Siberia (1968) 870 mb in a Pacific Typhoon An Ideal Ga s behaves in such a way that the relationship between pressure (P), temperature (T), and volume (V) are well characterized. The equation that relates the three variables, the Ideal Gas Law , is PV = nRT with n being the number of moles of gas, and R being a constant. If we keep the mass of the gas constant, then we can simplify the equation to (PV)/T = constant. That means that: For a constant P, T increases, V increases. For a constant V, T increases, P increases. For a constant T, P increases, V decreases. Since air is a gas, it responds to changes in temperature, elevation, and latitude (owing to a non-spherical Earth). -

Aircraft Performance: Atmospheric Pressure
Aircraft Performance: Atmospheric Pressure FAA Handbook of Aeronautical Knowledge Chap 10 Atmosphere • Envelope surrounds earth • Air has mass, weight, indefinite shape • Atmosphere – 78% Nitrogen – 21% Oxygen – 1% other gases (argon, helium, etc) • Most oxygen < 35,000 ft Atmospheric Pressure • Factors in: – Weather – Aerodynamic Lift – Flight Instrument • Altimeter • Vertical Speed Indicator • Airspeed Indicator • Manifold Pressure Guage Pressure • Air has mass – Affected by gravity • Air has weight Force • Under Standard Atmospheric conditions – at Sea Level weight of atmosphere = 14.7 psi • As air become less dense: – Reduces engine power (engine takes in less air) – Reduces thrust (propeller is less efficient in thin air) – Reduces Lift (thin air exerts less force on the airfoils) International Standard Atmosphere (ISA) • Standard atmosphere at Sea level: – Temperature 59 degrees F (15 degrees C) – Pressure 29.92 in Hg (1013.2 mb) • Standard Temp Lapse Rate – -3.5 degrees F (or 2 degrees C) per 1000 ft altitude gain • Upto 36,000 ft (then constant) • Standard Pressure Lapse Rate – -1 in Hg per 1000 ft altitude gain Non-standard Conditions • Correction factors must be applied • Note: aircraft performance is compared and evaluated with respect to standard conditions • Note: instruments calibrated for standard conditions Pressure Altitude • Height above Standard Datum Plane (SDP) • If the Barometric Reference Setting on the Altimeter is set to 29.92 in Hg, then the altitude is defined by the ISA standard pressure readings (see Figure 10-2, pg 10-3) Density Altitude • Used for correlating aerodynamic performance • Density altitude = pressure altitude corrected for non-standard temperature • Density Altitude is vertical distance above sea- level (in standard conditions) at which a given density is to be found • Aircraft performance increases as Density of air increases (lower density altitude) • Aircraft performance decreases as Density of air decreases (higher density altitude) Density Altitude 1. -

OCN 201 El Nino
OCN 201 El Nino El Nino theme page http://www.pmel.noaa.gov/tao/elnino/nino-home-low.html Reports to the Nation http://www.pmel.noaa.gov/tao/elnino/report/el-nino-report.html This page has all the text and figures and also how to get the booklet 1 El Nino is a major reorganisation of the equatorial climate system that affects regions far from its point of origin in the western Equatorial Pacific Occurs roughly every 6 years around Xmas-time Onset recognised by climatic effects --warm surface waters -- collapse of fisheries -- heavy rains in Peru/Ecuador/central Pacific -- droughts in Indonesia -- change in typhoon tracks Is a good example of how the ocean and atmosphere interact 2 What phase do you think we are in now? A El Nino B La Nina C Normal D I don’t know! A = El Nino 2014 2015 Southern Oscillation Atmospheric pressure differential between Tahiti and Darwin Normally low pressure in Darwin, high in Tahiti Low pressure High pressure Normal El Nino El Nino high pressure in Darwin, low in Tahiti Change in pressure differential results in weakening of easterly equatorial winds 3 Normal conditions in the Equatorial Pacific Strong easterly winds: Pile up warm water in the western Pacific -- thermocline deep in western Pacific, shallow in eastern Pacific Winds drive equatorial upwelling How much higher do you think that sea level is in the western Pacific? A 10cm B 50 cm C 1 metres D 5 metres E More! About 40 cm 4 Satellite image of chlorophyll abundance As thermocline is shallow in eastern Pacific upwelling brings nutrients to surface waters along