NDA Multidisciplinary Review and Evaluation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Azelaic Acid
Azelaic Acid (FINACEA) Topical Foam 15% National Drug Monograph August 2016 VA Pharmacy Benefits Management Services, Medical Advisory Panel, and VISN Pharmacist Executives The purpose of VA PBM Services drug monographs is to provide a focused drug review for making formulary decisions. Updates will be made when new clinical data warrant additional formulary discussion. Documents will be placed in the Archive section when the information is deemed to be no longer current. FDA Approval Information Description/Mechanism of Azelaic acid is a naturally occurring C9-dicarboxylic acid that is found in plants Action (such as whole grain cereals), animals and humans. Azelaic acid has antiinflammatory, antioxidative and antikeratinizing effects. In rosacea skin, azelaic acid decreases cathelicidin levels and kallikrein 5 (KLK5) activity and possibly inhibits toll-like receptor 2 (TLR2) expression.1 A 15% gel formulation has been marketed for rosacea, and 20% cream has been available for acne vulgaris. The newer foam formulation consists of an oil- in-water emulsion and was designed to have a higher lipid content than the gel for dry and sensitive skin. Indication(s) Under Review Topical treatment of inflammatory papules and pustules of mild to moderate in This Document rosacea. Dosage Form(s) Under Foam, 15% Review REMS REMS No REMS Postmarketing Requirements See Other Considerations for additional REMS information Pregnancy Rating Category B Executive Summary Efficacy There have been no head-to-head trials comparing the foam and gel formulations of azelaic acid in terms of safety, tolerability and efficacy in the treatment of papulopustular (PP) rosacea.. In two major randomized clinical trials, azelaic acid foam produced small benefits over vehicle foam in achieving Investigator’s Global Assessment (IGA) treatment success (NNTs of 9.2 and 11.5) and in reducing inflammatory lesion counts. -

Skin - Sulfa*Derm Sulfaderm Or Sulfa*Derm - Helps Promote Healthy Skin Function
Skin - Sulfa*Derm Sulfaderm or Sulfa*Derm - Helps promote Healthy skin Function. Has been shown to help clear up most Acne in 24 hours, Bacterial infections, Rashes, Bed Sores, Dermatitis, Eczema, Fungus/Yeast, Psoriasis type problems, Ring Worm and Wounds that won't heal. HISTORY OF SULFUR Harnessing the power of volcanos, our cutting edge formula is considered a breakthrough for the treatment of acne. Sulfa*Derm has been shown to clear up acne in one day. The active ingredient sulfur from volcanic ash destroys bacteria quickly. The Zinc Oxide combats rashes. Tea Tree Oil is a well known antiseptic and anti-fungal, while the Aloe Vera re-nourishes the skin. Vitamin E is used as the base instead of oils that clog up the skin. Sulfa*Derm is probably the best acne and everything else cream that has ever been made. When treating skin problems it is recommended to detoxify your liver. Sulfur is a yellow mineral that quite often occurs in nature in powder form. It can, under pressure bond to water, as in mineral springs or mix into the earth, as in mud baths. Normally sulfur is expunged from under the ground through the craters of venting volcanoes, where it is spread around in chunky blocks. Sulfur has been around for a long time. Native Polynesians claim to have cured a variety of infections in their hot sulfur mineral springs. Russian mud treatments, high in sulfur, have been used for centuries as a reputed therapy for arthritis. California's Napa Valley, specifically the city called Sulfur Springs, was the health spa for the wealthy until the early 1900's. -

Acne Class Update
© Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 | Fax 503-947-2596 Drug Class Update with New Drug Evaluation: Acne Drugs Date of Review: June 2020 Date of Last Review: November 2018 Dates of Literature Search: 08/03/2018 - 12/26/2019 Generic Name: Trifarotene Brand Name (Manufacturer): Aklief® (Galderma Laboratories, LP) Dossier Received: no Current Status of PDL Class: See Appendix 1. Purpose for Class Update: The acne class has had one new approval, trifarotene cream, and several new product formulations since it was last reviewed in 2018. The purpose of this update is to evaluate new comparative evidence for trifarotene cream for the treatment of acne vulgaris and any new data on comparative efficacy or harms in the acne class since the previous update. Acne conglobata, acne fulminans, and severe cystic acne are covered conditions under the Oregon Health Plan (OHP). Research Questions: 1. What is the comparative efficacy and effectiveness of treatments for severe acne (topical agents of adapalene, adapalene/benzoyl peroxide, tretinoin, tazarotene, benzoyl peroxide, salicylic acid, dapsone, azelaic acid, clindamycin, erythromycin, minocycline, sulfacetamide, trifarotene; oral systemic antibiotics of doxycycline, minocycline, tetracycline, azithromycin, erythromycin, clindamycin, trimethoprim, and sulfamethoxazole/trimethoprim; hormonal agents of oral contraceptives and spironolactone; and oral isotretinoin)? 2. What are the comparative harms of treatments for severe acne? 3. Are there subpopulations of patients in which a particular treatment for severe acne would be more effective or associated with less harm? Conclusions: There are no new high-quality clinical practice guidelines which have evaluated comparative efficacy and safety of treatments for acne vulgaris. -
Enhanced Catalytic Ozonation of Ibuprofen Using a 3D Structured
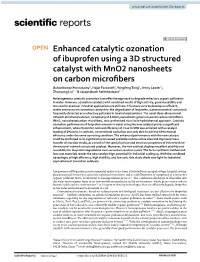
www.nature.com/scientificreports OPEN Enhanced catalytic ozonation of ibuprofen using a 3D structured catalyst with MnO2 nanosheets on carbon microfbers Guhankumar Ponnusamy1, Hajar Farzaneh2, Yongfeng Tong1, Jenny Lawler1, Zhaoyang Liu1* & Jayaprakash Saththasivam1* Heterogeneous catalytic ozonation is an efective approach to degrade refractory organic pollutants in water. However, ozonation catalysts with combined merits of high activity, good reusability and low cost for practical industrial applications are still rare. This study aims to develop an efcient, stable and economic ozonation catalyst for the degradation of Ibuprofen, a pharmaceutical compound frequently detected as a refractory pollutant in treated wastewaters. The novel three-dimensional network-structured catalyst, comprising of δ-MnO2 nanosheets grown on woven carbon microfbers (MnO2 nanosheets/carbon microfber), was synthesized via a facile hydrothermal approach. Catalytic ozonation performance of Ibuprofen removal in water using the new catalyst proves a signifcant enhancement, where Ibuprofen removal efciency of close to 90% was achieved with a catalyst loading of 1% (w/v). In contrast, conventional ozonation was only able to achieve 65% removal efciency under the same operating condition. The enhanced performance with the new catalyst could be attributed to its signifcantly increased available surface active sites and improved mass transfer of reaction media, as a result of the special surface and structure properties of this new three- dimensional network-structured catalyst. Moreover, the new catalyst displays excellent stability and reusability for ibuprofen degradation over successive reaction cycles. The facile synthesis method and low-cost materials render the new catalyst high potential for industrial scaling up. With the combined advantages of high efciency, high stability, and low cost, this study sheds new light for industrial applications of ozonation catalysts. -

Precipitated Sulfur: Summary Report
Precipitated Sulfur: Summary Report Item Type Report Authors Yuen, Melissa V.; Gianturco, Stephanie L.; Pavlech, Laura L.; Storm, Kathena D.; Yoon, SeJeong; Mattingly, Ashlee N. Publication Date 2020-02 Keywords Precipitated sulfur; Compounding; Food, Drug, and Cosmetic Act, Section 503B; Food and Drug Administration; Outsourcing facility; Drug compounding; Legislation, Drug; United States Food and Drug Administration Rights Attribution-NoDerivatives 4.0 International Download date 02/10/2021 22:32:18 Item License http://creativecommons.org/licenses/by-nd/4.0/ Link to Item http://hdl.handle.net/10713/12274 Summary Report Precipitated Sulfur Prepared for: Food and Drug Administration Clinical use of bulk drug substances nominated for inclusion on the 503B Bulks List Grant number: 2U01FD005946 Prepared by: University of Maryland Center of Excellence in Regulatory Science and Innovation (M-CERSI) University of Maryland School of Pharmacy February 2020 This report was supported by the Food and Drug Administration (FDA) of the U.S. Department of Health and Human Services (HHS) as part of a financial assistance award (U01FD005946) totaling $2,342,364, with 100 percent funded by the FDA/HHS. The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement by, the FDA/HHS or the U.S. Government. 1 Table of Contents REVIEW OF NOMINATIONS ................................................................................................... 4 METHODOLOGY ................................................................................................................... -
Hirsutism Joshua C
Review Hirsutism Joshua C. Berkowitz, BA; Adeel Kahtri, MD; Rao N. Saladi, MD; Dovid Herskowitz, BA; Joshua L. Fox, MD Hirsutism is defined as the development of a malelike pattern of excess hair especially in women. Hirsut- ism often results from raised androgen levels in the body and may indicate the existence of a serious underlying endocrine condition, such as polycystic ovary syndrome (PCOS). Treatment of hirsutism may require both medical and cosmetic actions. Medical therapy aims to counteract any suspected hormonal imbalance and can include administration of oral contraceptives and antiandrogens. Cosmetic treat- ment directly addresses excess hair and seeks to either remove the hair or diminish its appearance. Cos- metic options range from conventional methods, such as shaving and waxing, to modern techniques, such as laserCOS photoepilation. DERM irsutism refers to the growth of coarse that occurs despite normal androgen levels and normal terminal hair in females that follows a ovulatory function. malelike pattern, most commonly in the To comprehend the underlying mechanism of hirsut- upper lip area, beard area, abdomen, or ism, it is necessary to understand the physiology of hair chest. The amount of hair that is consid- growth. There are 2 types of hair: fine, nonpigmented Hered Donormal is subjective. In someNot cultures, women are vellus hairCopy and coarse, pigmented terminal hair. Both of disturbed by even a small amount of excess hair, while these hair types originate from the same pilosebaceous in other cultures, larger amounts may be tolerated and unit in the skin. Development of terminal hair mainly considered normal. The perception of excess hair has an is dependent on stimulation of the pilosebaceous unit associated psychosocial stigma that affects the lives of by androgens. -

Food and Drug Administration, HHS § 333.350
Food and Drug Administration, HHS § 333.350 (b) References in this subpart to reg- § 333.350 Labeling of acne drug prod- ulatory sections of the Code of Federal ucts. Regulations are to chapter I of title 21 (a) Statement of identity. The labeling unless otherwise noted. of the product contains the established name of the drug, if any, and identifies § 333.303 Definitions. the product as an ‘‘acne medication,’’ As used in this subpart: ‘‘acne treatment,’’ ‘‘acne medication’’ (a) Acne. A disease involving the oil (insert dosage form, e.g., ‘‘cream,’’ glands and hair follicles of the skin ‘‘gel,’’ ‘‘lotion,’’ or ‘‘ointment’’), or which is manifested by blackheads, ‘‘acne treatment’’ (insert dosage form, whiteheads, acne pimples, and acne e.g., ‘‘cream,’’ ‘‘gel,’’ ‘‘lotion,’’ or blemishes. ‘‘ointment’’). (b) Acne blemish. A flaw in the skin (b) Indications. The labeling of the resulting from acne. product states, under the heading ‘‘In- (c) Acne drug product. A drug product dications,’’ the phrase listed in para- used to reduce the number of acne graph (b)(1) of this section and may blemishes, acne pimples, blackheads, contain any of the additional phrases and whiteheads. listed in paragraph (b)(2) of this sec- (d) Acne pimple. A small, prominent, tion. Other truthful and nonmisleading inflamed elevation of the skin result- statements, describing only the indica- ing from acne. tions for use that have been established (e) Blackhead. A condition of the skin and listed in paragraph (b) of this sec- that occurs in acne and is character- tion, may also be used, as provided in ized by a black tip. -

DRUG and MEDICAL DEVICE HIGHLIGHTS Helping You Maintain and Improve Your Health 2019
DRUG AND MEDICAL DEVICE HIGHLIGHTS Helping you maintain and improve your health 2019 DRUG AND MEDICAL DEVICE HIGHLIGHTS 2019 Helping you maintain and improve your health Learn about the new drugs and medical devices that Health Canada approved for sale in Canada, the information we published about potential safety issues, and our other accomplishments in 2019. Health Canada is the federal department responsible for helping the people of Canada maintain and improve their health. Health Canada is committed to improving the lives of all of Canada’s people and to making this country’s population among the healthiest in the world as measured by longevity, lifestyle and effective use of the public health care system. Également disponible en français sous le titre : Préserver et améliorer votre santé : Faits saillants sur les médicaments et les instruments médicaux 2019 To obtain additional information, please contact: Health Canada Address Locator 0900C2 Ottawa, ON K1A 0K9 Tel.: 613-957-2991 Toll free: 1-866-225-0709 Fax: 613-941-5366 TTY: 1-800-465-7735 E-mail: [email protected] © Her Majesty the Queen in Right of Canada, as represented by the Minister of Health, 2020 Publication date: May 2020 This publication may be reproduced for personal or internal use only without permission provided the source is fully acknowledged. Cat.: H161-11E-PDF ISSN: 2562-9816 Pub.: 190484 CONTENTS WELCOME TO OUR 2019 HIGHLIGHTS REPORT ..........................................................................................1 MESSAGE FROM THE CHIEF MEDICAL -

Minocycline-Induced Pigmentation Mimicking Persistent Ecchymosis
CONTINUING MEDICAL EDUCATION Minocycline-Induced Pigmentation Mimicking Persistent Ecchymosis Sherry Youssef, MD, MPH, MS; Kathy Kim Langevin, MD, MPH; Lorraine C. Young, MD RELEASE DATE: July 2009 TERMINATION DATE: July 2010 The estimated time to complete this activity is 1 hour. GOAL To understand minocycline-induced pigmentation to better manage patients with the condition LEARNING OBJECTIVES Upon completion of this activity, you will be able to: 1. Distinguish the 3 common patterns of pigmentation based on clinical characteristics. 2. Recognize histologic findings of pigmentation. 3. Discuss the role of the duration and cumulative dose of minocycline on the incidence of pigmentation. INTENDED AUDIENCE This CME activity is designed for dermatologists and general practitioners. CME Test and Instructions on page 40. This article has been peer reviewed and ap- HealthCom, Inc. Albert Einstein College of Medicine proved by Ranon Ephraim Mann, MD, Assistant is accredited by the ACCME to provide continuing Professor, Department of Medicine (Dermatology), medical education for physicians. Albert Einstein College of Medicine. Review date: Albert Einstein College of Medicine designates June 2009. this educational activity for a maximum of 1 AMA This activity has been planned and implemented PRA Category 1 Credit TM. Physicians should only in accordance with the Essential Areas and Policies claim credit commensurate with the extent of their of the Accreditation Council for Continuing participation in the activity. Medical Education through the joint sponsorship of This activity has been planned and produced in Albert Einstein College of Medicine and Quadrant accordance with ACCME Essentials. Drs. Youssef and Young report no conflict of interest. Dr. -

19F Henry Ford Health System Publication List – May 2021 This
19f Henry Ford Health System Publication List – May 2021 This bibliography aims to recognize the scholarly activity and provide ease of access to journal articles, meeting abstracts, book chapters, books and other works published by Henry Ford Health System personnel. Searches were conducted in PubMed, Embase, and Web of Science during the month, and then imported into EndNote for formatting. There are 144 unique citations listed this month, with 8 articles and 5 conference abstracts on COVID-19. Articles are listed first, followed by conference abstracts, books and book chapters, and a bibliography of publications on COVID-19. Because of various limitations, this does not represent an exhaustive list of all published works by Henry Ford Health System authors. Click the “Full Text” link to view the articles to which Sladen Library provides access. If the full- text of the article is not available, you may request it through ILLiad by clicking on “Request Article,” or calling us at (313) 916-2550. If you would like to be added to the monthly email distribution list to automatically receive a PDF of this bibliography, or you have any questions or comments, please contact [email protected]. If your published work has been missed, please use this form to notify us for inclusion on next month’s list. All articles and abstracts listed here are deposited into Scholarly Commons, the HFHS institutional repository. Jump to: Articles Administration Neurology Allergy and Immunology Neurosurgery Anesthesiology Obstetrics, Gynecology and Women’s Behavioral -

2020 Research Annual Report Table of Contents
2020 RESEARCH ANNUAL REPORT TABLE OF CONTENTS PART I – INTERNAL MEDICINE DEPARTMENT ALLERGY AND IMMUNOLOGY ...................................................................................... 1 CARDIOLOGY/CARDIOVASCULAR RESEARCH…………………………………………..2 ENDOCRINOLOGY AND METABOLISM ........................................................................ 3 GASTROENTEROLOGY ................................................................................................ 5 HYPERTENSION AND VASCULAR RESEARCH……………………………………….…...6 PULMONARY……………………………………………………………………………………10 SLEEP MEDICINE………………………………………………………………………………10 GENERAL INTERNAL MEDICINE…………………………………………………….………12 HEMATOLOGY/ONCOLOGY………………………………………………………………….12 PART II – ALL OTHER CLINICAL DEPARTMENTS DERMATOLOGY ......................................................................................................... .14 EMERGENCY MEDICINE……………………………………………………………………..17 NEUROLOGY…………………………………………………………………………………...19 NEUROSURGERY……………………………………………………………………………… ORTHOPAEDICS/BONE & JOINT…………………………………………………………….31 OTOLARYNGOLOGY………………………………………………………………………… .36 PATHOLOGY ................................................................................................................ .36 PEDIATRICS…………………………………………………………………………………….37 PSYCHIATRY/BEHAVORIAL HEALTH………………………………………………………38 RADIATION ONCOLOGY ............................................................................................. 39 UROLOGY………………………………………………………………………………………40 WOMEN’S HEALTH……………………………………………………………………………42 i PART III POPULATION -
A20-73 Trifarotene (Acne Vulgaris) – Benefit Assessment According to §35A Social Code Book V1
IQWiG Reports – Commission No. A20-73 Trifarotene (acne vulgaris) – Benefit assessment according to §35a Social Code Book V1 Extract 1 Translation of Sections 2.1 to 2.5 of the dossier assessment Trifaroten (Acne vulgaris) – Nutzenbewertung gemäß § 35a SGB V (Version 1.0; Status: 12 November 2020). Please note: This translation is provided as a service by IQWiG to English-language readers. However, solely the German original text is absolutely authoritative and legally binding. Extract of dossier assessment A20-73 Version 1.0 Trifarotene (acne vulgaris) 12 November 2020 Publishing details Publisher Institute for Quality and Efficiency in Health Care Topic Trifarotene (acne vulgaris) – Benefit assessment according to §35a Social Code Book V Commissioning agency Federal Joint Committee Commission awarded on 13 August 2020 Internal Commission No. A20-73 Address of publisher Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen Im Mediapark 8 50670 Köln Germany Phone: +49 221 35685-0 Fax: +49 221 35685-1 E-mail: [email protected] Internet: www.iqwig.de Institute for Quality and Efficiency in Health Care (IQWiG) - i - Extract of dossier assessment A20-73 Version 1.0 Trifarotene (acne vulgaris) 12 November 2020 Medical and scientific advice . Prof. Dr. med. Dr. rer. nat. Enno Schmidt, University Hospital Schleswig-Holstein, Lübeck, Germany IQWiG thanks the medical and scientific advisor for his contribution to the dossier assessment. However, the advisor was not involved in the actual preparation of the dossier assessment. The responsibility for the contents of the dossier assessment lies solely with IQWiG. IQWiG employees involved in the dossier assessment . Anke Penno . Katharina Biester . Moritz Felsch .