Good Practice Guidelines for the Analysis of Child Speech
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

CONNECTED SPEECH IPA Symbols Represent the Correct Pronunciation
CONNECTED SPEECH IPA symbols represent the correct pronunciation of single words or segments of speech. However, we use single words or segments in isolation only occasionally. E.g., we can say “ah!” /ɑː/ to express surprise, or “sh!” /ʃ/ if we want to tell somebody to be quiet. Most commonly we use segments of speech or single words in a sequence, to form phrases or sentences. The sound “ah!” /ɑː/, for example, is likely to be found in whole sentences, to express: - surprise (“Ah, there you are!”) - pleasure (“Ah, this coffee is good.”) - admiration or sympathy (“Ah well, better luck next time.”) - when you disagree with somebody (“Ah, but that may not be true.”) In fact, we commonly use language in continuous, connected speech. Connected speech means speech produced without pauses. A consequence of connected speech is that single segments of speech are influenced by neighbouring segments (that is to say, speech sounds that come before and after them), and may slightly change their place or manner of articulation, or may sometimes totally disappear. Therefore the pronunciation of an isolated word may be different from the pronunciation of the same word in connected speech. These changes fall into two main types: assimilation and elision. ASSIMILATION In assimilation, one sound becomes phonetically similar to an adjacent sound. For example, the two words this and shop in isolation are pronounced - this /ðɪs/ - shop /ʃɒp/. In rapid speech, when the two words are pronounced together, the sound /s/ in this is influenced by the following initial sound and changes to /ʃ/. What we actually hear is: - this shop /ðɪʃʃɒp/. -

The Phonetics-Phonology Interface in Romance Languages José Ignacio Hualde, Ioana Chitoran
Surface sound and underlying structure : The phonetics-phonology interface in Romance languages José Ignacio Hualde, Ioana Chitoran To cite this version: José Ignacio Hualde, Ioana Chitoran. Surface sound and underlying structure : The phonetics- phonology interface in Romance languages. S. Fischer and C. Gabriel. Manual of grammatical interfaces in Romance, 10, Mouton de Gruyter, pp.23-40, 2016, Manuals of Romance Linguistics, 978-3-11-031186-0. hal-01226122 HAL Id: hal-01226122 https://hal-univ-paris.archives-ouvertes.fr/hal-01226122 Submitted on 24 Dec 2016 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Manual of Grammatical Interfaces in Romance MRL 10 Brought to you by | Université de Paris Mathematiques-Recherche Authenticated | [email protected] Download Date | 11/1/16 3:56 PM Manuals of Romance Linguistics Manuels de linguistique romane Manuali di linguistica romanza Manuales de lingüística románica Edited by Günter Holtus and Fernando Sánchez Miret Volume 10 Brought to you by | Université de Paris Mathematiques-Recherche Authenticated | [email protected] Download Date | 11/1/16 3:56 PM Manual of Grammatical Interfaces in Romance Edited by Susann Fischer and Christoph Gabriel Brought to you by | Université de Paris Mathematiques-Recherche Authenticated | [email protected] Download Date | 11/1/16 3:56 PM ISBN 978-3-11-031178-5 e-ISBN (PDF) 978-3-11-031186-0 e-ISBN (EPUB) 978-3-11-039483-2 Library of Congress Cataloging-in-Publication Data A CIP catalog record for this book has been applied for at the Library of Congress. -
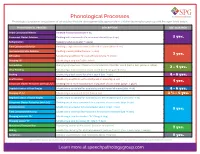
Phonological Processes
Phonological Processes Phonological processes are patterns of articulation that are developmentally appropriate in children learning to speak up until the ages listed below. PHONOLOGICAL PROCESS DESCRIPTION AGE ACQUIRED Initial Consonant Deletion Omitting first consonant (hat → at) Consonant Cluster Deletion Omitting both consonants of a consonant cluster (stop → op) 2 yrs. Reduplication Repeating syllables (water → wawa) Final Consonant Deletion Omitting a singleton consonant at the end of a word (nose → no) Unstressed Syllable Deletion Omitting a weak syllable (banana → nana) 3 yrs. Affrication Substituting an affricate for a nonaffricate (sheep → cheep) Stopping /f/ Substituting a stop for /f/ (fish → tish) Assimilation Changing a phoneme so it takes on a characteristic of another sound (bed → beb, yellow → lellow) 3 - 4 yrs. Velar Fronting Substituting a front sound for a back sound (cat → tat, gum → dum) Backing Substituting a back sound for a front sound (tap → cap) 4 - 5 yrs. Deaffrication Substituting an affricate with a continuant or stop (chip → sip) 4 yrs. Consonant Cluster Reduction (without /s/) Omitting one or more consonants in a sequence of consonants (grape → gape) Depalatalization of Final Singles Substituting a nonpalatal for a palatal sound at the end of a word (dish → dit) 4 - 6 yrs. Stopping of /s/ Substituting a stop sound for /s/ (sap → tap) 3 ½ - 5 yrs. Depalatalization of Initial Singles Substituting a nonpalatal for a palatal sound at the beginning of a word (shy → ty) Consonant Cluster Reduction (with /s/) Omitting one or more consonants in a sequence of consonants (step → tep) Alveolarization Substituting an alveolar for a nonalveolar sound (chew → too) 5 yrs. -

EVALUATING an INSTRUMENT for ASSESSING CONNECTED SPEECH PERFORMANCE USING FACETS ANALYSIS YOON AH SEONG University of Hawai‘I at M Ānoa
EVALUATING AN INSTRUMENT FOR ASSESSING CONNECTED SPEECH PERFORMANCE USING FACETS ANALYSIS YOON AH SEONG University of Hawai‘i at M ānoa ABSTRACT In the area of English pronunciation teaching, connected speech is increasingly being introduced and covered in pronunciation textbooks (e.g., Hagen, 2000; Weinstein, 2001). Connected speech is a phenomenon in spoken language that collectively includes phonological processes such as reduction, elision, intrusion, assimilation, and contraction. Several research studies have shown that connected speech instruction can help learners to more easily comprehend rapid speech used by native speakers (e.g., Brown & Hilferty, 2006; Celce-Murcia, Brinton, & Goodwin, 1996; Matsuzawa, 2006). Moreover, use of connected speech features can make learners sound more comprehensible and natural with less marked foreign accent (Brown & Kondo-Brown, 2006a; Dauer & Browne, 1992). However, compared to the growing connected speech literature regarding what forms to teach and how, there seems to be very little information on how to assess connected speech especially in terms of production. Therefore, the purpose of this study was to develop and evaluate a new test of connected speech performance within the context of an English study abroad program. The multi-faceted Rasch software FACETS was used to examine the effectiveness of the test instrument. The analyses used data from two administrations, a pretest and a posttest, and examined the relationships between examinee scores and various aspects of the testing situation (i.e., facets). The four facets investigated in this study were: (a) the examinees, (b) items, (c) raters, and (d) the rater L1 background. The results indicated that assessing the production of certain connected speech forms using this type of test instrument has potential. -

Connected Speech in Romanian: Exploring Sound Change Through an ASR System Ioana Chitorana, Ioana Vasilescub, Bianca Vieruc, Lori Lamelb
Connected speech in Romanian: Exploring sound change through an ASR system Ioana Chitorana, Ioana Vasilescub, Bianca Vieruc, Lori Lamelb a Université Paris Diderot and Laboratoire de Phonétique et Phonologie (UMR 7018) b LIMSI CNRS c Vocapia Research Abstract This study explores the hypothesis that traces of sound change can be found in connected speech processes as synchronic variation. To test this hypothesis we study the variation in connected speech through the output of an ASR system (Adda-Decker and Lamel, 1999). The case study is the vowel alternation [e]–[ʌ] after labials, encountered in Romanian historically, as part of a relatively sporadic sound change with unclear conditioning, as well as synchronically, as a phenomenon commonly observed in continuous speech. The specific question we address is whether the synchronic phenomenon in Romanian continuous speech is simply the result of general vowel reduction, or may reflect the sound change, with its apparent sensitivity to a labial consonantal context. We focus on the prepositions [pe] ‘on’ and [de] ‘of’, chosen specifically for their status as function words, more prone to vowel reduction than lexical words. We compare the ASR system’s choice of two transcription variants and their respective contexts. The results of this comparison suggest that the synchronic variation is grounded in the historical sound change, thus motivating a future systematic study of controlled speech, to determine the exact role of segmental contextual factors. The main result is that the selection of transcription variants is significantly different for the two prepositions. This allows us to better understand the conditioning environment of the relevant sound change, and reveals the language-specific articulatory and co-articulatory settings and dynamic patterns that may have led to it, as they emerge and can be observed in continuous speech. -

Assimilation, Reduction and Elision Reflected in the Selected Song Lyrics of Avenged Sevenfold
Dwi Nita Febriyanti Assimilation, Reduction and Elision Reflected in the Selected Song Lyrics of Avenged Sevenfold Dwi Nita Febriyanti [email protected] English Language Studies, Sanata Dharma University Abstract This paper discusses the phenomena of phonological rules, especially assimilation, reduction and elision processes. In this paper, the writer conducted phonological study which attempts to find the phenomena of those processes in song lyrics. In taking the data, the writer transcribed the lyrics of the songs, along with checking them to the internet source, then observed the lyrics to find the phenomena of assimilation, reduction, and elision. After that, she classified the observed phenomena in the lyrics based on the phonological processes. From the data analysis, the results showed that there were three processes found both in the first and second songs: assimilation, reduction and elision. The difference is that in the first song, it has four kinds of assimilation, while from the second song only has three kinds of assimilation. Keywords: assimilation, reduction, elision Introduction brothers and sisters’ discussion or even in songs, for which songs are considered as the As English spoken by the native media for the composer to share his feelings. speakers, it sometimes undergoes simplification to ease the native speakers in Assimilation usually happens in the expressing their feelings. That is why, it is double consonants. This is a phenomenon common for them to speak English in high which shows the influence of one sound to speed along with their emotions. As the another to become more similar. While for result, they make a ‘shortcut’ to get ease of the reduction process, it can happen to the their pronunciation. -

The Domain of Liaison: Theories and Data*
The domain of liaison: theories and data* GEERT BOOIJ and DAAN DE JONG Abstract In this paper it is argued that current theories of the domain of liaison are inadequate. It is shown thai 'domain' is a variable intralinguistic constraint on the (variable) rule of liaison. The variable nature of liaison is also apparent from the fact that its rate of application covaries with extralinguis- tic factors such as style and social class. These results also show that rules of sentence phonology should be based on reliable corpora of spoken language. 1. Introduction Liaison can be seen as the phenomenon of latent word-final consonants surfacing phonetically before a vowel-initial word. For instance, in petit ami [p(9)titami] 'little friend' the final / of petit is realized phonetically, whereas it does not surface in petit garςon [p(3)tigars5] 4small boy', because the following word begins with a consonant. These latent consonants also surface in inflectional and derivational morphology, as petite [p(s)tit] 'small', fern, sg., and petitesse [ptites] 'smallness' illustrate. A survey of alternative views of liaison is presented in Klausenburger (1984). The liaison consonant is usually (but not always, see Encreve 1983) tautosyllabic with the next word, the first fragment of the second word, as is illustrated by the syllabification of petit ami: (ρίί)σ(ΐ3)σ(ηιί)á where σ = syllable. That is, liaison usually implies enchamement.1 In this paper, we will focus on one particular problem in the analysis of liaison, its domain of application. It is well known that liaison only applies within certain environments. -

L Vocalisation As a Natural Phenomenon
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by University of Essex Research Repository L Vocalisation as a Natural Phenomenon Wyn Johnson and David Britain Essex University [email protected] [email protected] 1. Introduction The sound /l/ is generally characterised in the literature as a coronal lateral approximant. This standard description holds that the sounds involves contact between the tip of the tongue and the alveolar ridge, but instead of the air being blocked at the sides of the tongue, it is also allowed to pass down the sides. In many (but not all) dialects of English /l/ has two allophones – clear /l/ ([l]), roughly as described, and dark, or velarised, /l/ ([…]) involving a secondary articulation – the retraction of the back of the tongue towards the velum. In dialects which exhibit this allophony, the clear /l/ occurs in syllable onsets and the dark /l/ in syllable rhymes (leaf [li˘f] vs. feel [fi˘…] and table [te˘b…]). The focus of this paper is the phenomenon of l-vocalisation, that is to say the vocalisation of dark /l/ in syllable rhymes 1. feel [fi˘w] table [te˘bu] but leaf [li˘f] 1 This process is widespread in the varieties of English spoken in the South-Eastern part of Britain (Bower 1973; Hardcastle & Barry 1989; Hudson and Holloway 1977; Meuter 2002, Przedlacka 2001; Spero 1996; Tollfree 1999, Trudgill 1986; Wells 1982) (indeed, it appears to be categorical in some varieties there) and which extends to many other dialects including American English (Ash 1982; Hubbell 1950; Pederson 2001); Australian English (Borowsky 2001, Borowsky and Horvath 1997, Horvath and Horvath 1997, 2001, 2002), New Zealand English (Bauer 1986, 1994; Horvath and Horvath 2001, 2002) and Falkland Island English (Sudbury 2001). -

On the Production of Sandhi Phenomena in French: Psycholinguistic and Acoustic Data
On the production of sandhi phenomena in French: psycholinguistic and acoustic data Odile Bagou1, Violaine Michel1, Marina Laganaro1 1 Groupe NeuroPsychoLinguistique, FLSH, University of Neuchâtel, Switzerland [email protected], [email protected] Abstract detect than word-initial consonants (see also, [3]). Therefore, one might consider that liaison consonants have This preliminary study addresses two complementary a perceptual status that facilitates lexical access on W2. questions about the production of sandhi phenomena in French. First, we investigated whether the encoding of At least two hypotheses can be proposed to integrate enchaînement and liaison enchaînée involves a processing these two main results. First, liaison and enchaînement cost compared to non-resyllabified sequences. This consonants might be acoustically less salient than word- question was analyzed with a psycholinguistic production initial consonants. Indeed, liaison consonants [7, 8, 4, 5] time paradigm. The elicited sequences were then used to and enchaînement consonants [9, 10] have been reported to be shorter than word-initial consonants. Hence, the address our second question, namely how critical V1CV2 sequences are phonetically realized across different processing of the misalignement might be facilitated by boundary conditions. We compared the durational the presence of subtle acoustic cues that allow the listeners properties of critical sequences containing a word-final to discriminate resyllabified consonants from word-initial consonants. However, phoneme detection studies coda consonant (enchaînement: V1.C#V2), an additional consonant (liaison enchaînée: V +C#V ) and a similar established that only liaison consonants perceptually differ 1 2 from word-initial consonants [6]. Therefore, the effects onset consonant (V1#CV2). Results on production latencies suggested that the encoding of liaison enchaînée involves found in phoneme detection tasks cannot be explained by an additional processing cost compared to the two other acoustic differences only. -

Variable and Invariable Liaison in a Corpus of Spoken French
Erschienen in: Journal of French Language Studies ; 25 (2015), 3. - S. 367-396 https://dx.doi.org/10.1017/S0959269515000186 Journal of French Language Studies 25 (2015), 367–396, © Cambridge University Press doi:10.1017/S0959269515000186 Variable and invariable liaison in a corpus of spoken French JUDITH MEINSCHAEFERa,SVENBONIFERb AND CHRISTINE FRISCHc aFreie Universitat¨ Berlin bFormerly Universitat¨ Konstanz cFormerly Universitat¨ Wurzburg¨ (Received June 2013; revised October 2014) abstract Using texts selected from the C-Oral-Rom corpus, this study considers how linguistic and sociolinguistic variables affect liaison. In the majority of cases, liaison appears on monosyllabic function words. Individual lexemes differ greatly in rate of liaison. With regard to sociolinguistic variation, female speakers realize liaison consonants more often than male speakers, younger speakers realize it more often than older speakers, and liaison rates for speakers without university degree are higher than for speakers with university degree. Results are discussed in the light of models of prosodic structure and with respect to their implications for models of socio-linguistic variation. 1 introduction French liaison is a phrasal phonological phenomenon that consists in the pronunciation of a word-final consonant that is followed by a vowel-initial word, see (1a), where this consonant is otherwise not pronounced when the word is realised in isolation or before a pause,1 (1b). Here and in all following examples, realization of a liaison consonant is indicated in the orthographic representation by an underscore (‘_’), and word boundaries are indicated in the phonetic transcription by a hash (‘#’). (1) Liaison vs. absence of liaison for petit, Adj Masc ‘little’ a. -

Assimilation in English Connected Speech
Assimilation in English Connected Speech Assist. Lecturer Iman Farhan Mohammed Al-Mustansiriya University/ College of Arts/ Department of English Language البريد اﻹليكتروني: [email protected] 303 Abstract The current study focuses on one of the most significant problems of English phonemic analysis that is the phenomenon of assimilation. The notion assimilation is discussed, by many phoneticians and phonologists like Roach, Carr and many others, as a phonological process when there is a change of one sound into another because of adjacent segments. Assimilation has many types with different forms. It also has its own rules that constraint sounds and how a feature of a sound spreads to an adjacent sound. The aim of this paper is an attempt to provide an adequate background knowledge for those who are interested in this phonetic phenomenon. Keywords: (assimilation - speech – rules) 1.1 Assimilation: Overview Broadly speaking, Crystal (2011:39) states that assimilation means the effect that is expressed by one sound segment upon the production of another, so that the sounds become more similar. In this regard, Trask (2000:30) argues that the term assimilation is any syntagmatic change in which some sound seems more identical in nature to another sound in the same sequence, usually within one phonological word or phrase. Besides, Carr, (2008:16) assumes that assimilation is a process in which two, usually adjacent, segments appear more identical to each other. An instance of assimilation for place of articulation can be seen in sequences such as ten boys in 304 English, where the /n/ of ten seems to assimilate to the place of articulation of the following bilabial stop /tembɔɪz/. -

Morphophonology of Magahi
International Journal of Science and Research (IJSR) ISSN: 2319-7064 SJIF (2019): 7.583 Morphophonology of Magahi Saloni Priya Jawaharlal Nehru University, SLL & CS, New Delhi, India Salonipriya17[at]gmail.com Abstract: Every languages has different types of word formation processes and each and every segment of morphology has a sound. The following paper is concerned with the sound changes or phonemic changes that occur during the word formation process in Magahi. Magahi is an Indo- Aryan Language spoken in eastern parts of Bihar and also in some parts of Jharkhand and West Bengal. The term Morphophonology refers to the interaction of word formation with the sound systems of a language. The paper finds out the phonetic rules interacting with the morphology of lexicons of Magahi. The observations shows that he most frequent morphophonological process are Sandhi, assimilation, Metathesis and Epenthesis. Whereas, the process of Dissimilation, Lenition and Fortition are very Uncommon in nature. Keywords: Morphology, Phonology, Sound Changes, Word formation process, Magahi, Words, Vowels, Consonants 1. Introduction 3.1 The Sources of Magahi Glossary Morphophonology refers to the interaction between Magahi has three kind of vocabulary sources; morphological and phonological or its phonetic processes. i) In the first category, it has those lexemes which has The aim of this paper is to give a detailed account on the been processed or influenced by Sanskrit, Prakrit, sound changes that take place in morphemes, when they Apbhransh, ect. Like, combine to form new words in the language. धमम> ध륍म> धरम, स셍म> सꥍ셍> सााँ셍 ii) In the second category, it has those words which are 2.