University of Groningen Towards Dietary Assessment And
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Festiwal Chlebów Świata, 21-23. Marca 2014 Roku
FESTIWAL CHLEBÓW ŚWIATA, 21-23. MARCA 2014 ROKU Stowarzyszenie Polskich Mediów, Warszawska Izba Turystyki wraz z Zespołem Szkół nr 11 im. Władysława Grabskiego w Warszawie realizuje projekt FESTIWAL CHLEBÓW ŚWIATA 21 - 23 marca 2014 r. Celem tej inicjatywy jest promocja chleba, pokazania jego powszechności, ale i równocześnie różnorodności. Zaplanowaliśmy, że będzie się ona składała się z dwóch segmentów: pierwszy to prezentacja wypieków pieczywa według receptur kultywowanych w różnych częściach świata, drugi to ekspozycja producentów pieczywa oraz związanych z piekarnictwem produktów. Do udziału w żywej prezentacji chlebów świata zaprosiliśmy: Casa Artusi (Dom Ojca Kuchni Włoskiej) z prezentacją piady, producenci pity, macy oraz opłatka wigilijnego, Muzeum Żywego Piernika w Toruniu, Muzeum Rolnictwa w Ciechanowcu z wypiekiem chleba na zakwasie, przedstawiciele ambasad ze wszystkich kontynentów z pokazem własnej tradycji wypieku chleba. Dodatkowym atutem będzie prezentacja chleba astronautów wraz osobistym świadectwem Polskiego Kosmonauty Mirosława Hermaszewskiego. Nie zabraknie też pokazu rodzajów ziarna oraz mąki. Realizacją projektu będzie bezprecedensowa ekspozycja chlebów świata, pozwalająca poznać nie tylko dzieje chleba, ale też wszelkie jego odmiany występujące w różnych regionach świata. Taka prezentacja to podkreślenie uniwersalnego charakteru chleba jako pożywienia, który w znanej czy nieznanej nam dotychczas innej formie można znaleźć w każdym zakątku kuli ziemskiej zamieszkałym przez ludzi. Odkąd istnieje pismo, wzmiankowano na temat chleba, toteż, dodatkowo, jego kultowa i kulturowo – symboliczna wartość jest nie do przecenienia. Inauguracja FESTIWALU CHLEBÓW ŚWIATA planowana jest w piątek, w dniu 21 marca 2014 roku, pierwszym dniu wiosny a potrwa ona do niedzieli tj. do 23.03. 2014 r.. Uczniowie wówczas szukają pomysłów na nieodbywanie typowych zajęć lekcyjnych. My proponujemy bardzo celowe „vagari”- zapraszając uczniów wszystkich typów i poziomów szkoły z opiekunami do spotkania się na Festiwalu. -

Holland Shopping Centre 2012 Online Catalogue
8 83 Young oad. Chilliw ck, BC • V2P 6 192-0272· olla op.oom • 1 270-3595 Introduction........................... .. 3 Sandwich Spreads .................. 44 Sinterklaasl Christmas........... 4-1- Sandwich Sprinkles ................ 45 Gift Baskets......................... -10 Recipes •••••••••••••••••••••••••••••• 4E;,47 Christmas Gift Items ..•.•.•....... 11 irth .. Wedding Tiles............. 48 Céll1d"...............••••..•••.............. lL� F»lates St Tiles.......................... Ltd. 4� Cand" Rolis St Tins •••••••••••••••••• 13 Season Tiles St F»lates ••••••••••••• 50 BLilk Cëll1d" ..•.•.•.•..•.•.•............. lL4 BoerenlJont........................ 51-53 Sweet Bulk Candy ...••.............. 15 Dt!lft BIIIE!........................... 54,55 Salt" IItJIIt Cand" •••••••••••••••••••• iE; Birthda" Calendars ••••••••••••••••• 5E; Venco Licorice ........................ 17 Postca rds. .. .. .. .. .. .. .. .. .. .. .. .. ... 57 Drop I Licorice ...............••........ 18 Sou"enirs........................... 58,5� Chocolate •••••••••••••••••••••••••••••••• 1� tce"chains••••••••••••••••••••••••••••••• E;O Sugar Free •••••••••••••.••••••........•. �O Bike llells, Dolis .. Games•...... E;1 Pumpernickel Cakes..•.•.•.••.. �1 DVD's" ooks ...........•......•.••.. E;� VegetéllJles••••••••••••••••••••••••• ��,�3 André RieCentreu CD's ..•................... E;3 Sauces St Gourmet Sets ..... �4,�5 Cleaning F»roducts.................. E;4 Soup Mixes St Spices•.•.........•.. �E; F»ersonal Care ......................... E;5 Cup-a-Soups St Soup Extras -

View in 1986: "The Saccharine Sweet, Icky Drink? Yes, Well
Yashwantrao Chavan Maharashtra Open University V101:B. Sc. (Hospitality and Tourism Studies) V102: B.Sc. (Hospitality Studies & Catering Ser- vices) HTS 202: Food and Beverage Service Foundation - II YASHWANTRAO CHAVAN MAHARASHTRA OPEN UNIVERSITY (43 &Øا "••≤°• 3•≤©£• & §°© )) V101: B. Sc. Hospitality and Tourism Studies (2016 Pattern) V102: B. Sc. Hospitality Studies and Catering Services (2016 Pattern) Developed by Dr Rajendra Vadnere, Director, School of Continuing Education, YCMOU UNIT 1 Non Alcoholic Beverages & Mocktails…………...9 UNIT 2 Coffee Shop & Breakfast Service ………………69 UNIT 3 Food and Beverage Services in Restaurants…..140 UNIT 4 Room Service/ In Room Dinning........................210 HTS202: Food & Beverage Service Foundation -II (Theory: 4 Credits; Total Hours =60, Practical: 2 Credits, Total Hours =60) Unit – 1 Non Alcoholic Beverages & Mocktails: Introduction, Types (Tea, Coffee, Juices, Aerated Beverages, Shakes) Descriptions with detailed inputs, their origin, varieties, popular brands, presentation and service tools and techniques. Mocktails – Introduction, Types, Brief Descriptions, Preparation and Service Techniques Unit – 2 Coffee Shop & Breakfast Service: Introduction, Coffee Shop, Layout, Structure, Breakfast: Concept, Types & classification, Breakfast services in Hotels, Preparation for Breakfast Services, Mise- en-place and Mise-en-scene, arrangement and setting up of tables/ trays, Functions performed while on Breakfast service, Method and procedure of taking a guest order, emerging trends in Breakfast -

Kebersihan Pribadi Karyawan Bagian Patiseri Di Bawean Bakery Bandung
KEBERSIHAN PRIBADI KARYAWAN BAGIAN PATISERI DI BAWEAN BAKERY BANDUNG TUGAS AKHIR Diajukan untuk memenuhi salah satu syarat dalam menempuh Ujian Akhir Program Diploma III Oleh : Kharisma Nur Hawwa NIM : 201218668 JURUSAN HOSPITALITI PROGRAM STUDI MANAJEMEN PATISERI SEKOLAH TINGGI PARIWISATA BANDUNG 2016 LEMBAR PENGESAHAN Bandung, ……………………2016 Bandung, ……………………2016 Pembimbing II Pembimbing I Maksum Suparman, S.Pd., M.Pd. Drs. Rachmat Solahuddin, MSc NIP. 19680921 200605 1 001 Bandung, ……………..……2016 Menyetujui, Kepala Bagian Administrasi Akademik dan Kemahasiswaan Drs. Alexander Reyaan, MM NIP. 19630915 198603 1 001 Bandung, ……………..……2016 Mengesahkan, Ketua Sekolah Tinggi Pariwisata Bandung Dr. Anang Sutono, MM.Par., CHE NIP. 19650911 199203 1 001 PERNYATAAN MAHASISWA Yang bertanda tangan di bawah ini, saya : Nama : KHARISMA NUR HAWWA Tempat/Tanggal Lahir : BANDUNG, 15 FEBRUARI 1995 NIM : 201218668 Jurusan : HOSPITALITI Program Studi : MANAJEMEN PATISERI Dengan ini saya menyatakan bahwa: 1. Tugas Akhir/Proyek Akhir/Skripsi yang berjudul: KEBERSIHAN PRIBADI KARYAWAN BAGIAN PATISERI DI BAWEAN BAKERY BANDUNG ini adalah merupakan hasil karya dan hasil penelitian saya sendiri, bukan merupakan hasil penjiplakan, pengutipan, penyusunan oleh orang atau pihak lain atau cara-cara lain yang tidak sesuai dengan ketentuan akademik yang berlaku di STP Bandung dan etika yang berlaku dalam masyarakat keilmuan kecuali arahan dari Tim Pembimbing. 2. Dalam Tugas Akhir/Proyek Akhir/Skripsi ini tidak terdapat karya atau pendapat yang telah ditulis atau dipublikasikan -
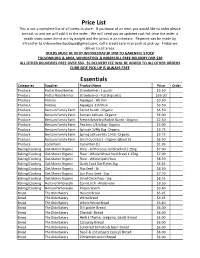
Price List This Is Not a Complete List of All Items in Store
Price List This is not a complete list of all items in store. If you know of an item you would like to order please contact us and we will add it to the order. We will send you an updated cost list once the order is made since some items are by weight and the prices is an estimate. Payment can be made by eTransfer to [email protected], call a credit card in or cash at pick-up. Friday we deliver to all areas. ODERS MUST BE IN BY WEDNESDAY @ 1PM TO GARENTEE STOCK TILLSONBURG & AREA, WOODSTOCK & INGERSOLL FREE DELIVERY OVR $30 ALL OTHER DELIVERIES FREE OVER $50. $5 DELIVERY FEE WILL BE ADDED TO ALL OTHER ORDERS CURB SIDE PICK-UP IS ALWAYS FREE Essentials Categories Supplier Product Name Price Order Produce Potter Road Berries Strawberries - 1 quartr $5.50 Produce Potter Road Berries Strawberries - Flat (6 quarts) $33.00 Produce Kotelas Aspaagus - 1lb thin $3.50 Produce Kotelas Aspaagus -1lb thick $3.50 Produce Bentum Family Farm Carrot Bunch - Organic $6.50 Produce Bentum Family Farm Romain Lettuce - Organic $6.00 Produce Bentum Family Farm French Breakfast Radish Bunch - Organic $2.50 Produce Bentum Family Farm Pea Sots 1/4lb Bag - Organic $5.00 Produce Bentum Family Farm Spinach 1/4lb Bag - Organic $3.75 Produce Bentum Family Farm Spring Lettuce Mix 1/4lb - Organic $3.75 Produce Bentum Family Farm Small Cucmbers - Organic (about 6) $6.50 Produce Local Farm Cucumber (1) $1.99 Baking/Cooking Oak Manor Organic Flour - All Purpose, Unbleached 1.25kg $7.00 Baking/Cooking Oak Manor Organic Flour - Whole Wheat Hard Bread 1.25kg $7.00 -

Stranas+2010-Lap+Hasil+Penelitian+
LAPORAN HIBAH PENELITIAN STRATEGIS NASIONAL TAHUN 2010 TEMA: PENGENTASAN KEMISKINAN STRATEGI PEMBERDAYAAN EKONOMI MELALUI LIFE SKILL EDUCATION SEBAGAI USAHA PENGENTASAN KEMISKINAN BAGI KOMUNITAS WARIA DI KOTAMADYA YOGYAKARTA Peneliti: Rr. Indah Mustikawati, M.Si., Ak. (Ketua) Mahendra Adhi Nugroho, M.Sc. (Anggota) Pratiwi Wahyu Widiarti, M.Si. (Anggota) FAKULTAS ILMU SOSIAL DAN EKONOMI UNIVERSITAS NEGERI YOGYAKARTA Tahun 2010 Dibiayai oleh Direktorat Jenderal Pendidikan Tinggi Kementerian Pendidikan Nasional, Sesuai dengan Surat Perjanjian Pelaksanaan Hibah Penelitian Nomor: 540/SP2H/PP/DP2M/VII/2010, Tanggal 24 Juli 2010 i HALAMAN PENGESAHAN LAPORAN PENELITIAN STRATEGIS NASIONAL 2010 1. Judul Penelitian : STRATEGI PEMBERDAYAAN EKONOMI MELALUI LIFE SKILL EDUCATION SEBAGAI USAHA PENGENTASAN KEMISKINAN BAGI KOMUNITAS WARIA DI KOTAMADYA YOGYAKARTA 2. Ketua Peneliti a. Nama Lengkap : Rr. Indah Mustikawati, SE.,MSi.,Ak. b. Jenis Kelamin : P c. N I P : 19681014.199802.2.001 d. Jabatan Fungsional : Lektor/ III/c. e. Jabatan Struktural : Ketua Program Studi Akuntansi S1 FISE UNY f. Bidang Keahlian : Akuntansi dan Pengauditan g. Fakultas/Jurusan : Fakultas Ilmu Sosial dan Ekonomi/ Pendidikan Akuntansi h. Perguruan Tinggi : Universitas Negeri Yogyakarta i. Tim Peneliti : No Nama Bidang Keahlian Fakultas/ Perguruan Jurusan Tinggi 1. Rr. Indah Mustikawati,SE.,MSi.Ak. Akuntansi dan FISE/ UNY Pengauditan. Pend.Akt 2. Mahendra Adhi Nugroho, S.E., Ekonomi dan Pend. FISE/ UNY M.Sc. Kewirausahaan Pend.Ek. 3. Dra. Pratiwi Wahyu Widiarti, M.Si. Psikologi FISE/ UNY Perkembangan PKN & Hukum 3. Jangka Waktu Penelitian : 1 tahun 4. Biaya yang disetujui : Rp. 27.500.000,- (dua puluh juta lima ratus ribu rupiah). Yogyakarta, November 2010 Mengetahui: Dekan, Ketua Peneliti (Sardiman AM.,MPd.) (Rr. -

Sweet Treats Around the World This Page Intentionally Left Blank
www.ebook777.com Sweet Treats around the World This page intentionally left blank www.ebook777.com Sweet Treats around the World An Encyclopedia of Food and Culture Timothy G. Roufs and Kathleen Smyth Roufs Copyright 2014 by ABC-CLIO, LLC All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, except for the inclusion of brief quotations in a review, without prior permission in writing from the publisher. The publisher has done its best to make sure the instructions and/or recipes in this book are correct. However, users should apply judgment and experience when preparing recipes, especially parents and teachers working with young people. The publisher accepts no responsibility for the outcome of any recipe included in this volume and assumes no liability for, and is released by readers from, any injury or damage resulting from the strict adherence to, or deviation from, the directions and/or recipes herein. The publisher is not responsible for any readerÊs specific health or allergy needs that may require medical supervision or for any adverse reactions to the recipes contained in this book. All yields are approximations. Library of Congress Cataloging-in-Publication Data Roufs, Timothy G. Sweet treats around the world : an encyclopedia of food and culture / Timothy G. Roufs and Kathleen Smyth Roufs. pages cm Includes bibliographical references and index. ISBN 978-1-61069-220-5 (hard copy : alk. paper) · ISBN 978-1-61069-221-2 (ebook) 1. Food·Encyclopedias. -
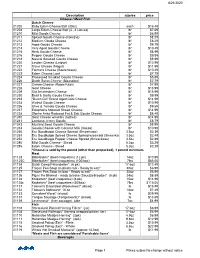
8/21/2020 Description Size/Ea Price Cheese / Meat
8/21/2020 Description size/ea price Cheese / Meat/ Fish Dutch Cheese 01202 Baby Edam Cheese Ball (30oz) each $16.49 01204 Large Edam Cheese Ball (3 - 4 Lbs ea) lb* $7.69 01210 Mild Gouda Cheese lb* $6.99 01211 Spiced Gouda Cheese (Komijne) lb* $8.29 01212 Medium Gouda Cheese lb* $8.29 01213 Aged Gouda Cheese lb* $9.79 01214 Very Aged Gouda Cheese lb* $10.49 01215 Herb Gouda Cheese lb* $8.99 01216 Pepper Gouda Cheese lb* $9.99 01218 Natural Smoked Gouda Cheese lb* $8.99 01220 Leyden Chesse (Leidse) lb* $10.99 01221 Clove Cheese (Nagel) lb* $11.99 01222 Farmers Cheese (Boerenkaas) lb* $10.49 01223 Edam Cheese Loaf lb* $7.79 01224 Processed Smoked Gouda Cheese lb* $5.89 01226 Dutch Swiss Cheese (Maasdam) lb* $7.79 01227 Cream Cheese (Room Kaas) lb* $7.99 01228 Goat Cheese lb* $13.99 01229 Old Amsterdam Cheese lb* $15.99 01230 Basil & Garlic Gouda Cheese lb* $9.99 01233 "Dutch Girl" Brand Aged Goat Cheese lb* $14.99 01234 Walnut Gouda Cheese lb* $10.99 01236 Olive & Tomato Gouda Cheese lb* $9.69 01237 Ewephoria Matured Sheep Cheese lb* $14.99 01238 Slanke Anke Reduced Fat & Salt Gouda Cheese lb* $8.49 01240 Goat Cheese w/Herbs (nettles) lb* $14.99 01241 Landana Jersey Gouda lb* $8.79 01243 Mustard Seed Gouda Cheese lb* $8.99 01244 Gouda Cheese with Coconut Milk (Kokos) lb* $10.99 01250 Eru Goudkuipje Cheese Spread (Smeerkaas) 3.5oz $2.39 01251 Eru Goudkuipje Spiced Cheese Spread w/sambal (Smeerkaas) 3.5oz $2.49 01252 Eru Goudkuipje Pepper Cheese Spread (Smeerkaas) 3.5oz $2.89 01280 Mild Gouda Cheese - Sliced 5.2oz $3.29 01285 Edam Cheese - Sliced 5.2oz $3.29 *Cheese is sold by the pound (other than prepacked), 1 pound minimum. -

Download Full Catalogue
BIBINA CATALOGUE INDEX Welcome to the Bibina Product Catalgoue. Due to it size the PDF document it is fully searchable. By pressing Ctrl+F (for find) on your keyboard to can search for product categories, or specific product. Due to the fact that products can only be in one category, please use the search function if you can't find the product you are searching for. Please note: Errors and omissions excepted (E&OE) ITEM CATEGORY BAKING/COOKING BISCUITS CEREAL CHEESE CHICKEN CHOCOLATES CLEANING/HOUSEHOLD CONDIMENTS/VINEGARS CONFECTIONERY DESSERT DRINKS/SYRUPS FLOURS AND MIXES FRUIT HERBS & SPICES NON STOCK NUTS OIL OLIVES PACKAGING PASTA/NOODLES PICKLED PRODUCTS RICE/COUS COUS SALT & PEPPER SEAFOOD SEASONAL SEEDS & GRAINS SMALLGOODS SNACKS SOUPS/STOCKS SPECIALTY SPREADS/SYRUPS SUGAR TEA & COFFEE TINNED/JARRED MEALS VEGETABLES VINEGAR Prices exclude gst CREATED 21/05/2021 BIBINA CATALOGUE PRODUCT LISTING BAKING/COOKING Item# Description Class Category 100602 100S AND 1000S - JAR BIBINA 300G SHELF BAKING/COOKING 104762 100S AND 1000S BIBINA 900G SHELF BAKING/COOKING 103833 100S AND 1000S GREEN - JAR BIBINA 300G SHELF BAKING/COOKING 105818 100S AND 1000S PINK - JAR BIBINA 300G SHELF BAKING/COOKING 107420 100S AND 1000S RED - JAR BIBINA 300G SHELF BAKING/COOKING 114002 BAKING POWDER BOB'S RED MILL 397G SHELF BAKING/COOKING 113619 BAKING POWDER FRUTEX 1KG SHELF BAKING/COOKING 101573 BAKING POWDER NATURE'S GROCER 1KG SHELF BAKING/COOKING 101585 BAKING POWDER PODRAVKA 5sX12G SHELF BAKING/COOKING 111528 BAKING POWDER VITAMINKA 5 PACK SHELF BAKING/COOKING -

Modul Guru Pembelajar Paket Keahlian Patiseri Sekolah Menengah Kejuruan (SMK) Dalam Rangka Pelatihan Guru Pasca Uji Kompetensi Guru (UKG)
MODUL GURU PEMBELAJAR Paket Keahlian Patiseri Sekolah Menengah Kejuruan(SMK) KELOMPOK KOMPETENSI J PUSAT PENGEMBANGAN DAN PEMBERDAYAAN PENDIDIK DAN TENAGA KEPENDIDIKAN (PPPPTK) BISNIS DAN PARIWISATA DIREKTORAT JENDERAL GURU DAN TENAGA KEPENDIDIKAN KEMENTERIAN PENDIDIKAN DAN KEBUDAYAAN TAHUN 2016 Penanggung Jawab : Dra. Hj. Djuariati Azhari, M.Pd KOMPETENSI PROFESIONAL Penulis: Dra. Endah Saraswati, M.M 08129002235 [email protected] Penelaah: Ir.Tuti Sumiati, M.M 08128051734 [email protected] KOMPETENSI PEDAGOGIK Penulis: Dra. Dwi Hastuti, M.M 081310579460 [email protected] Penelaah: Dra. Dwikora Hayuati, M.Pd 0817793766 [email protected] Layout & Desainer Grafis: Tim Copyright © 2016 Pusat Pengembangan dan Pemberdayaan Pendidik dan Tenaga Kependidikan Bisnis dan Pariwisata Direktorat Jenderal Pendidik dan Tenaga Kependidikan Hak Cipta dilindungi Undang-Undang Dilarang mengcopy sebagian atau keseluruhan isi buku ini untuk kepentingan komersial tanpa izin tertulis dari Kementerian Pendidikan dan Kebudayaan Kata Sambutan Peran guru profesional dalam proses pembelajaran sangat penting sebagai kunci keberhasilan belajar siswa. Guru Profesional adalah guru yang kompeten membangun proses pembelajaran yang baik sehingga dapat menghasilkan pendidikan yang berkualitas. Hal tersebut menjadikan guru sebagai komponen yang menjadi fokus perhatian pemerintah pusat maupun pemerintah daerah dalam peningkatan mutu pendidikan terutama menyangkut kompetensi guru. Pengembangan profesionalitas guru melalui program Guru Pembelajar (GP) merupakan upaya peningkatan kompetensi untuk semua guru. Sejalan dengan hal tersebut, pemetaan kompetensi guru telah dilakukan melalui uji kompetensi guru (UKG) untuk kompetensi pedagogik dan profesional pada akhir tahun 2015. Hasil UKG menunjukkan peta kekuatan dan kelemahan kompetensi guru dalam penguasaan pengetahuan. Peta kompetensi guru tersebut dikelompokkan menjadi 10 (sepuluh) kelompok kompetensi. Tindak lanjut pelaksanaan UKG diwujudkan dalam bentuk pelatihan paska UKG melalui program Guru Pembelajar. -
Food Consumption Survey Belgium Database 2014-2015 FOOD CONSUMPTION DATABASE
Food Consumption Survey Belgium Database 2014-2015 FOOD CONSUMPTION DATABASE Unit Nutrition & Health Unit of Epidemiology Juliette Wytsmanstraat 14 1050 Brussels | Belgium www.wiv-isp.be Table of contents 1. Introduction ........................................................................................................................ 3 2. Background characteristics............................................................................................. 4 2.1. Interview related information ................................................................................... 4 2.2. Demographic information....................................................................................... 12 2.3. Household characteristics ..................................................................................... 18 2.4. Education ................................................................................................................. 22 2.5. Pregnancy ................................................................................................................ 27 2.6. Anthropometric measurements............................................................................. 29 3. Food consumption interview (Epic-Soft) ..................................................................... 33 4. Food composition table characteristics....................................................................... 49 5. Consumed quantities .................................................................................................... -

Sunda Per Omzetgroep
Assortiment Sunda per Omzetgroep 10601 - 10750 | Rijst & Rijstproducten Artikelcode Artikel Omschrijving 10601 Surinaamse Rijst (SD FOODS) per baal a 20kg 10602 "Amigo" Long Grain Rijst per baal a 20kg 10603 "Golden Eagle" Long Grain Rijst per baal a 20kg 10604 Pandan Rijst (Dragon | Thai Hom Mali) per baal a 20kg 10605 Pandan Rijst (Dragon | Gebroken) per baal a 20kg 10606 Pandan Rijst (Aroy-D | Thai Hom Mali) per baal a 20kg 10607 Pandan Rijst (XO | Thai Hom Mali) per baal a 20kg 10608 Ketan Rijst (Aroy-D) per baal a 20kg 10609 Ketan Rijst (Dragon) per baal a 20kg 10610 Akash Basmatie Rijst per baal a 20kg 10611 Parboiled (Geel) Rijst per baal a 20kg 10612 Surinaamse Rijst (Palmier) per baal a 20kg 10615 "USA" (AEF) Long Grain Rijst per bl a 20kg 10616 Groene Driehoek Rijst per baal a 20kg 10617 Pandan Rijst "Rose" per baal a 20kg 10618 Pandan Rijst "Baitang" (KT | CMB) per baal a 20kg 10620 Pandan Rijst per zak a 10kg (doos a 2x10kg) 10621 Pandan Rijst (Dragon) per zak a 4,5kg (doos a 4x4,5kg) 10622 Pandan Rijst (Dragon) per doos a 12x1kg 10623 Pandan Rijst (XO) per doos a 4x4,5kg 10624 Pandan Rijst (XO) per doos a 20x1kg 10625 Ketan Rijst (Dragon) per doos a 12x1kg 10627 Pandan Rijst (Dragon | Gebroken) per 4x4,5kg 10630 Sushi Rijst (Shinzu | Calrose | Rood) per baal a 10kg 10642 Basmati Rijst (SAWI) per doos a 10x1kg 10650 Silvo Pandan Rijst per doos a 10x1kg 10651 Silvo Basmati Rijst per doos a 10x1kg 10652 Silvo Parboiled Rijst per doos a 10x1kg 10700 Lontong (Gebroken) per doos a 80x125 gram 10701 Lontong (Heel) per doos a 80x125