A New Heterozygous Mutation in GP1BA Gene Responsible For
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hemoglobin Interaction with Gp1ba Induces Platelet Activation And
ARTICLE Platelet Biology & its Disorders Hemoglobin interaction with GP1bα induces platelet activation and apoptosis: a novel mechanism associated with intravascular hemolysis Rashi Singhal,1,2,* Gowtham K. Annarapu,1,2,* Ankita Pandey,1 Sheetal Chawla,1 Amrita Ojha,1 Avinash Gupta,1 Miguel A. Cruz,3 Tulika Seth4 and Prasenjit Guchhait1 1Disease Biology Laboratory, Regional Centre for Biotechnology, National Capital Region, Biotech Science Cluster, Faridabad, India; 2Biotechnology Department, Manipal University, Manipal, Karnataka, India; 3Thrombosis Research Division, Baylor College of Medicine, Houston, TX, USA, and 4Hematology, All India Institute of Medical Sciences, New Delhi, India *RS and GKA contributed equally to this work. ABSTRACT Intravascular hemolysis increases the risk of hypercoagulation and thrombosis in hemolytic disorders. Our study shows a novel mechanism by which extracellular hemoglobin directly affects platelet activation. The binding of Hb to glycoprotein1bα activates platelets. Lower concentrations of Hb (0.37-3 mM) significantly increase the phos- phorylation of signaling adapter proteins, such as Lyn, PI3K, AKT, and ERK, and promote platelet aggregation in vitro. Higher concentrations of Hb (3-6 mM) activate the pro-apoptotic proteins Bak, Bax, cytochrome c, caspase-9 and caspase-3, and increase platelet clot formation. Increased plasma Hb activates platelets and promotes their apoptosis, and plays a crucial role in the pathogenesis of aggregation and development of the procoagulant state in hemolytic disorders. Furthermore, we show that in patients with paroxysmal nocturnal hemoglobinuria, a chronic hemolytic disease characterized by recurrent events of intravascular thrombosis and thromboembolism, it is the elevated plasma Hb or platelet surface bound Hb that positively correlates with platelet activation. -

A Computational Approach for Defining a Signature of Β-Cell Golgi Stress in Diabetes Mellitus
Page 1 of 781 Diabetes A Computational Approach for Defining a Signature of β-Cell Golgi Stress in Diabetes Mellitus Robert N. Bone1,6,7, Olufunmilola Oyebamiji2, Sayali Talware2, Sharmila Selvaraj2, Preethi Krishnan3,6, Farooq Syed1,6,7, Huanmei Wu2, Carmella Evans-Molina 1,3,4,5,6,7,8* Departments of 1Pediatrics, 3Medicine, 4Anatomy, Cell Biology & Physiology, 5Biochemistry & Molecular Biology, the 6Center for Diabetes & Metabolic Diseases, and the 7Herman B. Wells Center for Pediatric Research, Indiana University School of Medicine, Indianapolis, IN 46202; 2Department of BioHealth Informatics, Indiana University-Purdue University Indianapolis, Indianapolis, IN, 46202; 8Roudebush VA Medical Center, Indianapolis, IN 46202. *Corresponding Author(s): Carmella Evans-Molina, MD, PhD ([email protected]) Indiana University School of Medicine, 635 Barnhill Drive, MS 2031A, Indianapolis, IN 46202, Telephone: (317) 274-4145, Fax (317) 274-4107 Running Title: Golgi Stress Response in Diabetes Word Count: 4358 Number of Figures: 6 Keywords: Golgi apparatus stress, Islets, β cell, Type 1 diabetes, Type 2 diabetes 1 Diabetes Publish Ahead of Print, published online August 20, 2020 Diabetes Page 2 of 781 ABSTRACT The Golgi apparatus (GA) is an important site of insulin processing and granule maturation, but whether GA organelle dysfunction and GA stress are present in the diabetic β-cell has not been tested. We utilized an informatics-based approach to develop a transcriptional signature of β-cell GA stress using existing RNA sequencing and microarray datasets generated using human islets from donors with diabetes and islets where type 1(T1D) and type 2 diabetes (T2D) had been modeled ex vivo. To narrow our results to GA-specific genes, we applied a filter set of 1,030 genes accepted as GA associated. -
Supp Table 1.Pdf
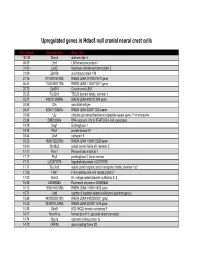
Upregulated genes in Hdac8 null cranial neural crest cells fold change Gene Symbol Gene Title 134.39 Stmn4 stathmin-like 4 46.05 Lhx1 LIM homeobox protein 1 31.45 Lect2 leukocyte cell-derived chemotaxin 2 31.09 Zfp108 zinc finger protein 108 27.74 0710007G10Rik RIKEN cDNA 0710007G10 gene 26.31 1700019O17Rik RIKEN cDNA 1700019O17 gene 25.72 Cyb561 Cytochrome b-561 25.35 Tsc22d1 TSC22 domain family, member 1 25.27 4921513I08Rik RIKEN cDNA 4921513I08 gene 24.58 Ofa oncofetal antigen 24.47 B230112I24Rik RIKEN cDNA B230112I24 gene 23.86 Uty ubiquitously transcribed tetratricopeptide repeat gene, Y chromosome 22.84 D8Ertd268e DNA segment, Chr 8, ERATO Doi 268, expressed 19.78 Dag1 Dystroglycan 1 19.74 Pkn1 protein kinase N1 18.64 Cts8 cathepsin 8 18.23 1500012D20Rik RIKEN cDNA 1500012D20 gene 18.09 Slc43a2 solute carrier family 43, member 2 17.17 Pcm1 Pericentriolar material 1 17.17 Prg2 proteoglycan 2, bone marrow 17.11 LOC671579 hypothetical protein LOC671579 17.11 Slco1a5 solute carrier organic anion transporter family, member 1a5 17.02 Fbxl7 F-box and leucine-rich repeat protein 7 17.02 Kcns2 K+ voltage-gated channel, subfamily S, 2 16.93 AW493845 Expressed sequence AW493845 16.12 1600014K23Rik RIKEN cDNA 1600014K23 gene 15.71 Cst8 cystatin 8 (cystatin-related epididymal spermatogenic) 15.68 4922502D21Rik RIKEN cDNA 4922502D21 gene 15.32 2810011L19Rik RIKEN cDNA 2810011L19 gene 15.08 Btbd9 BTB (POZ) domain containing 9 14.77 Hoxa11os homeo box A11, opposite strand transcript 14.74 Obp1a odorant binding protein Ia 14.72 ORF28 open reading -

Supplementary Table 1: Adhesion Genes Data Set
Supplementary Table 1: Adhesion genes data set PROBE Entrez Gene ID Celera Gene ID Gene_Symbol Gene_Name 160832 1 hCG201364.3 A1BG alpha-1-B glycoprotein 223658 1 hCG201364.3 A1BG alpha-1-B glycoprotein 212988 102 hCG40040.3 ADAM10 ADAM metallopeptidase domain 10 133411 4185 hCG28232.2 ADAM11 ADAM metallopeptidase domain 11 110695 8038 hCG40937.4 ADAM12 ADAM metallopeptidase domain 12 (meltrin alpha) 195222 8038 hCG40937.4 ADAM12 ADAM metallopeptidase domain 12 (meltrin alpha) 165344 8751 hCG20021.3 ADAM15 ADAM metallopeptidase domain 15 (metargidin) 189065 6868 null ADAM17 ADAM metallopeptidase domain 17 (tumor necrosis factor, alpha, converting enzyme) 108119 8728 hCG15398.4 ADAM19 ADAM metallopeptidase domain 19 (meltrin beta) 117763 8748 hCG20675.3 ADAM20 ADAM metallopeptidase domain 20 126448 8747 hCG1785634.2 ADAM21 ADAM metallopeptidase domain 21 208981 8747 hCG1785634.2|hCG2042897 ADAM21 ADAM metallopeptidase domain 21 180903 53616 hCG17212.4 ADAM22 ADAM metallopeptidase domain 22 177272 8745 hCG1811623.1 ADAM23 ADAM metallopeptidase domain 23 102384 10863 hCG1818505.1 ADAM28 ADAM metallopeptidase domain 28 119968 11086 hCG1786734.2 ADAM29 ADAM metallopeptidase domain 29 205542 11085 hCG1997196.1 ADAM30 ADAM metallopeptidase domain 30 148417 80332 hCG39255.4 ADAM33 ADAM metallopeptidase domain 33 140492 8756 hCG1789002.2 ADAM7 ADAM metallopeptidase domain 7 122603 101 hCG1816947.1 ADAM8 ADAM metallopeptidase domain 8 183965 8754 hCG1996391 ADAM9 ADAM metallopeptidase domain 9 (meltrin gamma) 129974 27299 hCG15447.3 ADAMDEC1 ADAM-like, -

Cellular and Molecular Signatures in the Disease Tissue of Early
Cellular and Molecular Signatures in the Disease Tissue of Early Rheumatoid Arthritis Stratify Clinical Response to csDMARD-Therapy and Predict Radiographic Progression Frances Humby1,* Myles Lewis1,* Nandhini Ramamoorthi2, Jason Hackney3, Michael Barnes1, Michele Bombardieri1, Francesca Setiadi2, Stephen Kelly1, Fabiola Bene1, Maria di Cicco1, Sudeh Riahi1, Vidalba Rocher-Ros1, Nora Ng1, Ilias Lazorou1, Rebecca E. Hands1, Desiree van der Heijde4, Robert Landewé5, Annette van der Helm-van Mil4, Alberto Cauli6, Iain B. McInnes7, Christopher D. Buckley8, Ernest Choy9, Peter Taylor10, Michael J. Townsend2 & Costantino Pitzalis1 1Centre for Experimental Medicine and Rheumatology, William Harvey Research Institute, Barts and The London School of Medicine and Dentistry, Queen Mary University of London, Charterhouse Square, London EC1M 6BQ, UK. Departments of 2Biomarker Discovery OMNI, 3Bioinformatics and Computational Biology, Genentech Research and Early Development, South San Francisco, California 94080 USA 4Department of Rheumatology, Leiden University Medical Center, The Netherlands 5Department of Clinical Immunology & Rheumatology, Amsterdam Rheumatology & Immunology Center, Amsterdam, The Netherlands 6Rheumatology Unit, Department of Medical Sciences, Policlinico of the University of Cagliari, Cagliari, Italy 7Institute of Infection, Immunity and Inflammation, University of Glasgow, Glasgow G12 8TA, UK 8Rheumatology Research Group, Institute of Inflammation and Ageing (IIA), University of Birmingham, Birmingham B15 2WB, UK 9Institute of -

Datasheet: MCA740PE Product Details
Datasheet: MCA740PE Description: MOUSE ANTI HUMAN CD42b:RPE Specificity: CD42b Other names: GPIB-ALPHA Format: RPE Product Type: Monoclonal Antibody Clone: AK2 Isotype: IgG1 Quantity: 100 TESTS Product Details Applications This product has been reported to work in the following applications. This information is derived from testing within our laboratories, peer-reviewed publications or personal communications from the originators. Please refer to references indicated for further information. For general protocol recommendations, please visit www.bio-rad-antibodies.com/protocols. Yes No Not Determined Suggested Dilution Flow Cytometry Neat Where this antibody has not been tested for use in a particular technique this does not necessarily exclude its use in such procedures. The suggested working dilution is given as a guide only. It is recommended that the user titrates the antibody for use in his/her own system using appropriate negative/positive controls. Target Species Human Product Form Purified IgG conjugated to R. Phycoerythrin (RPE) - lyophilized Reconstitution Reconstitute with 1 ml distilled water Max Ex/Em Fluorophore Excitation Max (nm) Emission Max (nm) RPE 488nm laser 496 578 Preparation Purified IgG prepared by affinity chromatography on Protein A from tissue culture supernatant Buffer Solution Phosphate buffered saline Preservative 0.09% Sodium Azide Stabilisers 1% Bovine Serum Albumin 5% Sucrose External Database Links UniProt: P07359 Related reagents Entrez Gene: 2811 GP1BA Related reagents Page 1 of 3 Specificity Mouse anti Human CD42b antibody, clone AK2 recognizes the human CD42b cell surface antigen, also known as platelet glycoprotein GP1B. CD42b is expressed by platelets and megakaryocytes. Clone AK2 has been reported to block the binding of von Willebrand Factor (VWF) to platelets Flow Cytometry Use 10ul of the suggested working dilution to label 100ul whole blood. -
Path Ggf 5 2020.Pdf
Hemostasis Hemostasis and Thrombosis Normal hemostasis is a consequence of tightly regulated processes that maintain blood in a fluid state in normal vessels, yet also permit the rapid formation of a hemostatic clot at the site of a vascular injury. Thrombosis involves blood clot formation within intact vessels. Both hemostasis and thrombosis involve three components: the vascular wall, platelets and the coagulation cascade. Elements of the Hemostatic process • Endothelium • Anti-thrombosis • Pro-thrombosis • Platelets • Platelet-endothelial cell interaction • Coagulation cascade http://www.as.miami.edu/chemistry/2086/chapter_21/NEW-Chap21_class_part1_files/image002.jpg After initial injury there is a brief period of arteriolar vasoconstriction mediated by reflex neurogenic mechanisms and augmented by the local secretion of factors such as endothelin (a potent endothelium-derived vasoconstrictor) The effect is transient, however, and bleeding would resume if not for activation of the platelet and coagulation systems. Endothelial injury exposes highly thrombogenic subendothelial extracellular matrix (ECM), facilitating platelet adherence and activation. Activation of platelets results in a dramatic shape change (from small rounded discs to flat plates with markedly increased surface area), as well as the release of secretory granules. Within minutes the secreted products recruit additional platelets (aggregation) to form a hemostatic plug; this process is referred to as primary hemostasis. http://www.ouhsc.edu/platelets/Platelet%20Pic s/Platelets3.jpg http://medcell.med.yale.edu/histology/blood_bone_marr ow_lab/images/platelets_em.jpg Tissue factor is also exposed at the site of injury. Also known as factor III and thromboplastin, tissue factor is a membrane-bound procoagulant glycoprotein synthesized by endothelial cells. It acts in conjunction with factor VII (see below) as the major in vivo initiator of the coagulation cascade, eventually culminating in thrombin generation. -

Biomechanical Thrombosis: the Dark Side of Force and Dawn of Mechano- Medicine
Open access Review Stroke Vasc Neurol: first published as 10.1136/svn-2019-000302 on 15 December 2019. Downloaded from Biomechanical thrombosis: the dark side of force and dawn of mechano- medicine Yunfeng Chen ,1 Lining Arnold Ju 2 To cite: Chen Y, Ju LA. ABSTRACT P2Y12 receptor antagonists (clopidogrel, pras- Biomechanical thrombosis: the Arterial thrombosis is in part contributed by excessive ugrel, ticagrelor), inhibitors of thromboxane dark side of force and dawn platelet aggregation, which can lead to blood clotting and A2 (TxA2) generation (aspirin, triflusal) or of mechano- medicine. Stroke subsequent heart attack and stroke. Platelets are sensitive & Vascular Neurology 2019;0. protease- activated receptor 1 (PAR1) antag- to the haemodynamic environment. Rapid haemodynamcis 1 doi:10.1136/svn-2019-000302 onists (vorapaxar). Increasing the dose of and disturbed blood flow, which occur in vessels with these agents, especially aspirin and clopi- growing thrombi and atherosclerotic plaques or is caused YC and LAJ contributed equally. dogrel, has been employed to dampen the by medical device implantation and intervention, promotes Received 12 November 2019 platelet thrombotic functions. However, this platelet aggregation and thrombus formation. In such 4 Accepted 14 November 2019 situations, conventional antiplatelet drugs often have also increases the risk of excessive bleeding. suboptimal efficacy and a serious side effect of excessive It has long been recognized that arterial bleeding. Investigating the mechanisms of platelet thrombosis -

Confirmation of Pathogenic Mechanisms by SARS-Cov-2–Host
Messina et al. Cell Death and Disease (2021) 12:788 https://doi.org/10.1038/s41419-021-03881-8 Cell Death & Disease ARTICLE Open Access Looking for pathways related to COVID-19: confirmation of pathogenic mechanisms by SARS-CoV-2–host interactome Francesco Messina 1, Emanuela Giombini1, Chiara Montaldo1, Ashish Arunkumar Sharma2, Antonio Zoccoli3, Rafick-Pierre Sekaly2, Franco Locatelli4, Alimuddin Zumla5, Markus Maeurer6,7, Maria R. Capobianchi1, Francesco Nicola Lauria1 and Giuseppe Ippolito 1 Abstract In the last months, many studies have clearly described several mechanisms of SARS-CoV-2 infection at cell and tissue level, but the mechanisms of interaction between host and SARS-CoV-2, determining the grade of COVID-19 severity, are still unknown. We provide a network analysis on protein–protein interactions (PPI) between viral and host proteins to better identify host biological responses, induced by both whole proteome of SARS-CoV-2 and specific viral proteins. A host-virus interactome was inferred, applying an explorative algorithm (Random Walk with Restart, RWR) triggered by 28 proteins of SARS-CoV-2. The analysis of PPI allowed to estimate the distribution of SARS-CoV-2 proteins in the host cell. Interactome built around one single viral protein allowed to define a different response, underlining as ORF8 and ORF3a modulated cardiovascular diseases and pro-inflammatory pathways, respectively. Finally, the network-based approach highlighted a possible direct action of ORF3a and NS7b to enhancing Bradykinin Storm. This network-based representation of SARS-CoV-2 infection could be a framework for pathogenic evaluation of specific 1234567890():,; 1234567890():,; 1234567890():,; 1234567890():,; clinical outcomes. -

MALE Protein Name Accession Number Molecular Weight CP1 CP2 H1 H2 PDAC1 PDAC2 CP Mean H Mean PDAC Mean T-Test PDAC Vs. H T-Test
MALE t-test t-test Accession Molecular H PDAC PDAC vs. PDAC vs. Protein Name Number Weight CP1 CP2 H1 H2 PDAC1 PDAC2 CP Mean Mean Mean H CP PDAC/H PDAC/CP - 22 kDa protein IPI00219910 22 kDa 7 5 4 8 1 0 6 6 1 0.1126 0.0456 0.1 0.1 - Cold agglutinin FS-1 L-chain (Fragment) IPI00827773 12 kDa 32 39 34 26 53 57 36 30 55 0.0309 0.0388 1.8 1.5 - HRV Fab 027-VL (Fragment) IPI00827643 12 kDa 4 6 0 0 0 0 5 0 0 - 0.0574 - 0.0 - REV25-2 (Fragment) IPI00816794 15 kDa 8 12 5 7 8 9 10 6 8 0.2225 0.3844 1.3 0.8 A1BG Alpha-1B-glycoprotein precursor IPI00022895 54 kDa 115 109 106 112 111 100 112 109 105 0.6497 0.4138 1.0 0.9 A2M Alpha-2-macroglobulin precursor IPI00478003 163 kDa 62 63 86 72 14 18 63 79 16 0.0120 0.0019 0.2 0.3 ABCB1 Multidrug resistance protein 1 IPI00027481 141 kDa 41 46 23 26 52 64 43 25 58 0.0355 0.1660 2.4 1.3 ABHD14B Isoform 1 of Abhydrolase domain-containing proteinIPI00063827 14B 22 kDa 19 15 19 17 15 9 17 18 12 0.2502 0.3306 0.7 0.7 ABP1 Isoform 1 of Amiloride-sensitive amine oxidase [copper-containing]IPI00020982 precursor85 kDa 1 5 8 8 0 0 3 8 0 0.0001 0.2445 0.0 0.0 ACAN aggrecan isoform 2 precursor IPI00027377 250 kDa 38 30 17 28 34 24 34 22 29 0.4877 0.5109 1.3 0.8 ACE Isoform Somatic-1 of Angiotensin-converting enzyme, somaticIPI00437751 isoform precursor150 kDa 48 34 67 56 28 38 41 61 33 0.0600 0.4301 0.5 0.8 ACE2 Isoform 1 of Angiotensin-converting enzyme 2 precursorIPI00465187 92 kDa 11 16 20 30 4 5 13 25 5 0.0557 0.0847 0.2 0.4 ACO1 Cytoplasmic aconitate hydratase IPI00008485 98 kDa 2 2 0 0 0 0 2 0 0 - 0.0081 - 0.0 -
Exploratory Aspirin Resistance Trial in Healthy Japanese Volunteers (J-ART) Using Platelet Aggregation As a Measure of Thrombogenicity
The Pharmacogenomics Journal (2007) 7, 395–403 & 2007 Nature Publishing Group All rights reserved 1470-269X/07 $30.00 www.nature.com/tpj ORIGINAL ARTICLE Exploratory aspirin resistance trial in healthy Japanese volunteers (J-ART) using platelet aggregation as a measure of thrombogenicity T Fujiwara1, M Ikeda2, K Esumi3, Aspirin prevents the production of thromboxane A2 (TXA2) by irreversibly 4 5 inhibiting platelet cyclooxygenase, exhibiting antiplatelet actions. This agent TD Fujita , M Kono , has been reported to prevent relapse in patients with ischemic heart disease 6 4 H Tokushige , T Hatoyama , or cerebral infarction via this action mechanism. However, there are T Maeda7, T Asai4, T Ogawa6, individual differences in this action, and aspirin is not effective in some T Katsumata4, S Sasaki8, patients, which is referred to as ‘aspirin resistance’. In this study, we analyzed E Suzuki7, M Suzuki5, F Hino9, laboratory aspirin resistance by platelet aggregation in 110 healthy adult 10 10 Japanese males using 24 single-nucleotide polymorphisms (SNPs) of nine TK Fujita , H Zaima , genes involved in platelet aggregation/hemorrhage. Among SNPs involved M Shimada9, T Sugawara8, in platelet aggregation, aspirin was less effective for 924T homozygote of a 10 3 Y Tsuzuki , Y Hashimoto , TXA2 receptor, 924T4C, and 1018C homozygote of a platelet membrane H Hishigaki1, S Horimoto5, glycoprotein GPIba, 1018C4T, suggesting that 924T and 1018C alleles are 2 4 involved in aspirin resistance. N Miyajima , T Yamamoto , The Pharmacogenomics Journal (2007) -

The Human in Vivo Biomolecule Corona Onto Pegylated Liposomes
RevisedView metadata, Manuscript citation and similar papers at core.ac.uk brought to you by CORE provided by Nottingham Trent Institutional Repository (IRep) 1 2 3 4 5 6 The human in vivo biomolecule corona onto PEGylated 7 8 liposomes: a proof-of-concept clinical study 9 10 11 Marilena Hadjidemetriou1, Sarah McAdam2, Grace Garner2, Chelsey Thackeray3, David Knight4, Duncan 12 Smith5, Zahraa Al-Ahmady1, Mariarosa Mazza1, Jane Rogan2, Andrew Clamp3 and Kostas Kostarelos1* 13 14 15 16 17 1Nanomedicine Lab, Faculty of Biology, Medicine & Health, AV Hill Building, The University of Manchester, Manchester, United Kingdom; 2 18 Manchester Cancer Research Centre Biobank, The Christie NHS Foundation Trust, CRUK Manchester Institute, Manchester, United Kingdom 3Institute of Cancer Sciences and The Christie NHS Foundation Trust, Manchester Cancer Research Centre (MCRC), 19 University of Manchester, Manchester, United Kingdom 20 4Bio-MS Facility, Michael Smith Building, The University of Manchester, Manchester, United Kingdom; 21 5xCRUK Manchester Institute, The University of Manchester, Manchester, United Kingdom 22 23 24 25 26 27 28 29 30 31 _______________________________________ 32 * Correspondence should be addressed to: [email protected] 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 1 63 64 65 1 2 3 4 5 Abstract 6 7 The self-assembled layered adsorption of proteins onto nanoparticle (NP) surfaces, once in contact 8 with biological fluids, has been termed the ‘protein corona’ and it is gradually seen as a determinant 9 10 factor for the overall biological behavior of NPs.