Working Together to Provide High Quality, Cost Effective Primary
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Geometry of the Butterknowle Fault at Bishop Auckland (County Durham, UK), from Gravity Survey and Structural Inversion
ESSOAr | https:/doi.org/10.1002/essoar.10501104.1 | CC_BY_NC_ND_4.0 | First posted online: Mon, 11 Nov 2019 01:27:37 | This content has not been peer reviewed. Geometry of the Butterknowle Fault at Bishop Auckland (County Durham, UK), from gravity survey and structural inversion Rob Westaway 1,*, Sean M. Watson 1, Aaron Williams 1, Tom L. Harley 2, and Richard Middlemiss 3 1 James Watt School of Engineering, University of Glasgow, James Watt (South) Building, Glasgow G12 8QQ, UK. 2 WSP, 70 Chancery Lane, London WC2A 1AF, UK. 3 School of Physics, University of Glasgow, Kelvin Building, Glasgow G12 8QQ, UK. * Correspondence: [email protected]; Abstract: The Butterknowle Fault is a major normal fault of Dinantian age in northern England, bounding the Stainmore Basin and the Alston Block. This fault zone has been proposed as a source of deep geothermal energy; to facilitate the design of a geothermal project in the town of Bishop Auckland further investigation of its geometry was necessary and led to the present study. We show using three-dimensional modelling of a dense local gravity survey, combined with structural inversion, that this fault has a ramp-flat-ramp geometry, ~250 m of latest Carboniferous / Early Permian downthrow having occurred on a fault surface that is not a planar updip continuation of that which had accommodated the many kilometres of Dinantian extension. The gravity survey also reveals relatively low-density sediments in the hanging-wall of the Dinantian fault, interpreted as porous alluvial fan deposits, indicating that a favourable geothermal target indeed exists in the area. -
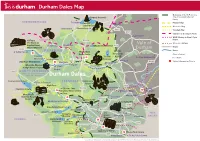
Durham Dales Map
Durham Dales Map Boundary of North Pennines A68 Area of Outstanding Natural Barleyhill Derwent Reservoir Newcastle Airport Beauty Shotley northumberland To Hexham Pennine Way Pow Hill BridgeConsett Country Park Weardale Way Blanchland Edmundbyers A692 Teesdale Way Castleside A691 Templetown C2C (Sea to Sea) Cycle Route Lanchester Muggleswick W2W (Walney to Wear) Cycle Killhope, C2C Cycle Route B6278 Route The North of Vale of Weardale Railway England Lead Allenheads Rookhope Waskerley Reservoir A68 Mining Museum Roads A689 HedleyhopeDurham Fell weardale Rivers To M6 Penrith The Durham North Nature Reserve Dales Centre Pennines Durham City Places of Interest Cowshill Weardale Way Tunstall AONB To A690 Durham City Place Names Wearhead Ireshopeburn Stanhope Reservoir Burnhope Reservoir Tow Law A690 Visitor Information Points Westgate Wolsingham Durham Weardale Museum Eastgate A689 Train S St. John’s Frosterley & High House Chapel Chapel Crook B6277 north pennines area of outstanding natural beauty Durham Dales Willington Fir Tree Langdon Beck Ettersgill Redford Cow Green Reservoir teesdale Hamsterley Forest in Teesdale Forest High Force A68 B6278 Hamsterley Cauldron Snout Gibson’s Cave BishopAuckland Teesdale Way NewbigginBowlees Visitor Centre Witton-le-Wear AucklandCastle Low Force Pennine Moor House Woodland ButterknowleWest Auckland Way National Nature Lynesack B6282 Reserve Eggleston Hall Evenwood Middleton-in-Teesdale Gardens Cockfield Fell Mickleton A688 W2W Cycle Route Grassholme Reservoir Raby Castle A68 Romaldkirk B6279 Grassholme Selset Reservoir Staindrop Ingleton tees Hannah’s The B6276 Hury Hury Reservoir Bowes Meadow Streatlam Headlam valley Cotherstone Museum cumbria North Balderhead Stainton RiverGainford Tees Lartington Stainmore Reservoir Blackton A67 Reservoir Barnard Castle Darlington A67 Egglestone Abbey Thorpe Farm Centre Bowes Castle A66 Greta Bridge To A1 Scotch Corner A688 Rokeby To Brough Contains Ordnance Survey Data © Crown copyright and database right 2015. -

Teesdale Local Plan Chapter 5 Population and Housing
Teesdale Local Plan – Adopted June 2002 CHAPTER 5 POPULATION & HOUSING Teesdale Local Plan – Adopted June 2002 5) POPULATION & HOUSING 5.0 INTRODUCTION 5.0.1 The projected population of the district is inextricably linked to the District’s future housing requirements. The maintenance of a stable population is a realistic goal for the next ten years. Due to the ageing demographic structure of the district, in–migration would be required to achieve this goal. 5.1 POPULATION PROJECTIONS & HOUSING REQUIREMENTS 5.1.1 The housing requirements of the plan are calculated on the basis of Durham County Structure Plan Policy. Policy 7 of the Structure Plan states that Teesdale will require about 1,000 more dwellings between 1991 – 2006. As this Plan extends to 2010 the housing requirement calculation will need to make an estimate for the building requirement between 2006 and 2010. This is achieved by taking the Structure Plan figure, converting that to an annual building rate and thereby providing an estimate for the period 2006-2010. The housing requirement will also need to take into account those dwellings completed between 1991 – 1998. 5.1.2 According to the published 1991 census figures the Population of Teesdale is 24,068 of which 306 are in communal establishments, Population projections based on 1997 estimates show the population is expected to increase slightly to 24,193 by 2010, with the number of persons in communal establishments expected to remain constant, this would lead to 23,887 requiring housing. 5.1.3 As previously mentioned above, latest projections show a slight increase in population added to that the reduction in the average household size would result in the need for additional dwellings. -

County Durham Plan (Adopted 2020)
County Durham Plan ADOPTED 2020 Contents Foreword 5 1 Introduction 7 Neighbourhood Plans 7 Assessing Impacts 8 Duty to Cooperate: Cross-Boundary Issues 9 County Durham Plan Key Diagram and Monitoring 10 2 What the County Durham Plan is Seeking to Achieve 11 3 Vision and Objectives 14 Delivering Sustainable Development 18 4 How Much Development and Where 20 Quantity of Development (How Much) 20 Spatial Distribution of Development (Where) 29 5 Core Principles 71 Building a Strong Competitive Economy 71 Ensuring the Vitality of Town Centres 78 Supporting a Prosperous Rural Economy 85 Delivering a Wide Choice of High Quality Homes 98 Protecting Green Belt Land 124 Sustainable Transport 127 Supporting High Quality Infrastructure 138 Requiring Good Design 150 Promoting Healthy Communities 158 Meeting the Challenge of Climate Change, Flooding and Coastal Change 167 Conserving and Enhancing the Natural and Historic Environment 185 Minerals and Waste 212 Appendices A Strategic Policies 259 B Table of Superseded Policies 261 C Coal Mining Risk Assessments, Minerals Assessments and Minerals and/or Waste 262 Infrastructure Assessment D Safeguarding Mineral Resources and Safeguarded Minerals and Waste Sites 270 E Glossary of Terms 279 CDP Adopted Version 2020 Contents List of County Durham Plan Policies Policy 1 Quantity of New Development 20 Policy 2 Employment Land 30 Policy 3 Aykley Heads 38 Policy 4 Housing Allocations 47 Policy 5 Durham City's Sustainable Urban Extensions 61 Policy 6 Development on Unallocated Sites 68 Policy 7 Visitor Attractions -

Northeast England – a History of Flash Flooding
Northeast England – A history of flash flooding Introduction The main outcome of this review is a description of the extent of flooding during the major flash floods that have occurred over the period from the mid seventeenth century mainly from intense rainfall (many major storms with high totals but prolonged rainfall or thaw of melting snow have been omitted). This is presented as a flood chronicle with a summary description of each event. Sources of Information Descriptive information is contained in newspaper reports, diaries and further back in time, from Quarter Sessions bridge accounts and ecclesiastical records. The initial source for this study has been from Land of Singing Waters –Rivers and Great floods of Northumbria by the author of this chronology. This is supplemented by material from a card index set up during the research for Land of Singing Waters but which was not used in the book. The information in this book has in turn been taken from a variety of sources including newspaper accounts. A further search through newspaper records has been carried out using the British Newspaper Archive. This is a searchable archive with respect to key words where all occurrences of these words can be viewed. The search can be restricted by newspaper, by county, by region or for the whole of the UK. The search can also be restricted by decade, year and month. The full newspaper archive for northeast England has been searched year by year for occurrences of the words ‘flood’ and ‘thunder’. It was considered that occurrences of these words would identify any floods which might result from heavy rainfall. -

( I ) North of England Institute of Mining Engineers
( I ) NORTH OF ENGLAND INSTITUTE OF MINING ENGINEERS. TRANSACTIONS. VOL. XVIII. 1868-9. NEWCASTLE UPON TYNE. A REID. PRINTING COURT BUILDINGS AKENSIDE HILL 1869. ( II ) [blank page ] ( III ) CONTENTS OF VOL. XVIII. page. page Report of Council ....................... v Officers 1869/70 ............... xvii Finance Report .................. ........vii Members .......................... xviii Technical Education Report ......ix Graduates.................... xxxviii Treasurer's Account............ .......xii Subscribing Collieries......... xli General Account ....................... xiv Rules ( as altered to Patrons................................. .......xv August 7, 1869 ).....xliii Honorary and Life Members .....xvi Catalogue of Library. End of Vol. GENERAL MEETINGS. 1868. page Sept. 5. — Model of a new Safety-Cage exhibited by Mr. James Barkus; Mr. J. A. R. Morison's Invention for preventing Tampering with Safety-Lamps explained 2 Oct. 3. — Technical Education Committee's Report read ......... 7 "Remarks on Rivetting," by Mr. W. Boyd............ 9 Discussed........... ............... 4 Hann's Safety-Lamp exhibited and explained .... ... 5 Nov. 7. — Mr. George Elliot's Inaugural Address ...... 19 Report of the Smoke Committee ............... 37 Dec. 5. — Books Presented to Mr. E. Bainbridge ............ 41 Paper "On the Mechanical Stoking of Steam Boilers," by Mr. James Nelson........................ 51 Discussed ....................... 1 41 1869. Feb. 6. — Tail-Rope Committee's Report discussed ............ 61 Paper by Mr. A. L. Steavenson " On some Experiments with the Lemielle Ventilator at Page Bank Colliery " ......... 63 Discussed................ 57 Mar. 6. — Further Discussion on Tail-Rope Committee's Report ...... 71 Mr. Boyd's Paper “On Mechanical Rivetting " discussed...... 82 April 10.— Mr. I. L. Bell elected a Vice-President in place of Mr. J. F. Spencer (resigned) ... ....... 85 Further discussion on Mr. Nelson's Paper "On the Mechanical Firing of Steam Boilers 86 Further discussion on Mr. -

The Slack, Butterknowle, Bishop Auckland, DL13 5HT Asking Price
The Slack, Butterknowle, Bishop Auckland, DL13 5HT TWO BEDROOMS | BUNGALOW | DETACHED | DEVELOPMENT OPPORTUNITY 1.5 ACRE PLOT | RURAL LOCATION | NO ONWARD CHAIN | EPC GRADE TBC Asking Price: £180,000 The Slack, Butterknowle, Bishop DINING ROOM Auckland, DL13 5HT 4.0m (13' 1") x 3.9m (12' 10") The second reception room is another good size A unique opportunity to purchase this two bed with coal fire, feature surround and bay window to detached bungalow set in approximately 1.5 acres. the front elevation. With the right planning consent this fantastic plot could be redeveloped with the current building transformed and extended creating a modern luxury home or the site redeveloped into multiple homes. It is located a short distance from Butterknowle. which has local amenities available in the village such as a post office, doctors practice, pub and primary school. The neighbouring towns of Bishop Auckland and Barnard Castle provide access to further amenities such as supermarkets, cafés, restaurants, healthcare services and both primary and secondary schools. The nearby A688 and the A68 lead to the A1(M) both North and South, ideal for commuters, whilst there is also an extensive public transport system through the villages allowing for access to the neighbouring towns. KITCHEN In brief the property comprises; a living room, 6.4m (21' 0") x 2.7m (8' 10") dining room, kitchen, two bedrooms and the family The kitchen contains a range of wall, base and bathroom. Externally there is a large driveway drawer units, contrasting work surfaces and providing ample off street parking, enclosed lawned sink/drainer unit. -

Stags Head East
EAST STAGS HEAD THE SLACK | BUTTERKNOWLE | DL13 5HU MAXIMISING VALUE EAST STAGS HEAD THE SLACK | BUTTERKNOWLE | DL13 5HU Barnard Castle - 8 Miles | Bishop Auckland - 8 Miles | Durham 19 Miles Substantial semi-detached house • Stone built property • Generously proportioned accommodation • 2 Reception rooms plus study • 3 Bedrooms • Parking facility and adjoining store • Elevated rear garden • Rural situation Guide Price £135,000 Barnard Castle 01833 690390 [email protected] The Area The Slack is situated between Copley and Butterknowle, in the heart of the Gaunless Valley with the neighbouring towns of Barnard Castle, Bishop Auckland and Darlington are all within a short drive. The towns provide a range of shopping, educational and recreational facilities with the neighbouring villages of Butterknowle and Cockfield providing for more immediate needs. For the commuter the A68 and A1 (M) provide links with the major commercial centres of the north east. Darlington Mainline Railway Station and Durham Tees Valley International Airport offer further communications with the rest of the country. The Property East Stags Head is a striking building which forms part of a former public house, which has been divided in recent years into two substantial semi detached homes. It has oil fired central heating and double glazing throughout along with well proportioned accommodation, off street parking and a private elevated rear garden. A substantial wooden entrance door leads through to the entrance vestibule, which in turn leads into the entrance hall, which has doors leading off to the living accommodation and stairs leading up to the first floor. There are two good sized reception rooms both with open grate fires and original surrounds. -

National Evaluation of the DH Integrated Care Pilots: Appendices
CHILDREN AND FAMILIES The RAND Corporation is a nonprofit institution that helps improve policy and EDUCATION AND THE ARTS decisionmaking through research and analysis. ENERGY AND ENVIRONMENT HEALTH AND HEALTH CARE This electronic document was made available from www.rand.org as a public INFRASTRUCTURE AND service of the RAND Corporation. TRANSPORTATION INTERNATIONAL AFFAIRS LAW AND BUSINESS NATIONAL SECURITY Skip all front matter: Jump to Page 16 POPULATION AND AGING PUBLIC SAFETY SCIENCE AND TECHNOLOGY Support RAND TERRORISM AND Browse Reports & Bookstore HOMELAND SECURITY Make a charitable contribution For More Information Visit RAND at www.rand.org Explore RAND Europe View document details Limited Electronic Distribution Rights This document and trademark(s) contained herein are protected by law as indicated in a notice appearing later in this work. This electronic representation of RAND intellectual property is provided for non-commercial use only. Unauthorized posting of RAND electronic documents to a non-RAND Web site is prohibited. RAND electronic documents are protected under copyright law. Permission is required from RAND to reproduce, or reuse in another form, any of our research documents for commercial use. For information on reprint and linking permissions, please see RAND Permissions. This product is part of the RAND Corporation technical report series. Reports may include research findings on a specific topic that is limited in scope; present discussions of the methodology employed in research; provide literature reviews, survey instru- ments, modeling exercises, guidelines for practitioners and research professionals, and supporting documentation; or deliver preliminary findings. All RAND reports un- dergo rigorous peer review to ensure that they meet high standards for research quality and objectivity. -

E R Ic G Atesw It Hsomeofh Is Prom Is In
24th August, | | Wednesday, 24th August, 1994 THE TEESDALE MERCURY 11 FOOTBALL PIGEONS GOLF FIVE A SIDE FOOTBALL 5 Barbara Matthews Super 45 points Parkin nearly All Stars & Castle LF.A. takes first place total earns cup does the trick Wallers crack in Butterknowle Homing Society Even wood Town played well nine goals apiece lications (NOW results for race flown from fo r A n d rew at times hut suffered a bad start Cricketers Arms had a good 4- RATION): Mid Thoresby Hall on Saturday: 1, 3 to their new Northern League 1 win in the Teesdale five a side and 4, Mrs Barbara Matthews Hezmalhalch season when they went down 2-0 football league this week over ember velocities 1382.29, 1341.63 and Andrew Hezmalhalch won the after travelling to meet Brandon Brown Jug, who had several reg 1336.49; 2, Jacqueline Moss Jack Manning Trophy at United. ulars missing due to holidays. 1359.54. Two bird club: 1, Mrs Barnard Castle Golf Club on Evenwood were below The Cricketers are now on 30 mis) claims: 21st Barbara Matthews 1341.63; 2, Sunday with an excellent score strength as several players were points, a 100% record, and must H. Peairs and Son 1313.06; 3, of 45 Stableford points. injured and some were away on be hot favourites to capture the holiday. But they almost took an Barry Blackett 1301.39; 4, Deric Hugill took second place title. Glaxo Club are on 27 after early lead through newcomer rOCK QUOTA Kellett and Makepeace 1287.05. with a very good 44, while shar an exciting 5-4 win over Piston Derek Parkin, whose shot tore UR GROWING ing third place spot, two points Broke. -

(Public Pack)Agenda Document for Area
Area Planning Committee (South and West) Date Thursday 20 April 2017 Time 2.00 pm Venue Council Chamber, Council Offices, Spennymoor Business Part A 1. Apologies for Absence 2. Substitute Members 3. Declarations of Interest (if any) 4. Minutes of the Meeting held on 23 March 2017 (Pages 3 - 12) 5. Applications to be determined a) DM/16/03214/FPA - 33 Cockton Hill Road, Bishop Auckland (Pages 13 - 24) Change of use of first floor from office (B1) to House in Multiple Occupation (C4) (Retrospective). b) DM/17/00517/FPA - Field To The East Of Victoria Cottages, Garden House, Cockfield (Pages 25 - 38) Demolition of dwelling known as 1 Victoria Cottage and erection of dwelling, with associated access and garaging on land between Victoria House and Pine Tops c) DM/17/00463/FPA - Land To The East Of Cobweb Cottage, Loop Lane, Butterknowle (Pages 39 - 50) Demolition of existing outbuildings and erection of 1 no. dwelling (revised scheme to refusal DM/15/03005/FPA). 6. Such other business as, in the opinion of the Chairman of the meeting, is of sufficient urgency to warrant consideration. Clare Pattinson Interim Head of Legal and Democratic Services County Hall Durham 10 April 2017 To: The Members of the Area Planning Committee (South and West) Councillor H Nicholson (Chairman) Councillor M Dixon (Vice-Chairman) Councillors B Armstrong, D Bell, D Boyes, J Clare, K Davidson, E Huntington, C Kay, S Morrison, A Patterson, G Richardson, L Taylor, C Wilson and S Zair Contact: Ian Croft Tel: 03000 269702 Agenda Item 4 DURHAM COUNTY COUNCIL At a Meeting of Area Planning Committee (South and West) held in Council Chamber, Council Offices, Spennymoor on Thursday 23 March 2017 at 2.00 pm Present: Councillor H Nicholson (Chairman) Members of the Committee: Councillors M Dixon (Vice-Chairman), B Armstrong, J Clare, P Conway, E Huntington, C Kay, S Morrison, A Patterson, G Richardson, L Taylor and C Wilson 1 Apologies for Absence Apologies for absence were received from Councillors D Bell, K Davidson and S Zair. -

NOTICE of UNCONTESTED ELECTION Durham County Election of Parish Councillors for Bearpark Parish on Thursday 6 May 2021
NOTICE OF UNCONTESTED ELECTION Durham County Election of Parish Councillors for Bearpark Parish on Thursday 6 May 2021 I, John Hewitt being the Returning Officer at the above election, report that the persons whose names appear below were duly elected Parish Councillors for Bearpark Parish Name of Candidate Home Address Description (if any) ANDERSON 12 South View, Bearpark, Labour Party Norman Mark Durham, DH7 7DE EDWARDS 13 Temperance Terrace, Ushaw Owen Christopher Moor, Durham, DH7 7PQ KEMP 18 Blackburn Close, Bearpark, Rosemary Alison Durham, DH7 7TQ PEART 32 Taylor Avenue, Bearpark, Labour Party John Howe Durham, DH7 7AY THOMPSON 10 Aldin Grange Hall, Bearpark, Labour Party Joseph Matthew George Durham, DH7 7AR WILSON 58 Taylor Avenue, Bearpark, Labour Party Marion Durham, DH7 7AY Dated Friday 9 April 2021 John Hewitt Returning Officer Printed and published by the Returning Officer, Room 1/104-115, County Hall, Durham, DH1 5UL NOTICE OF UNCONTESTED ELECTION Durham County Election of Parish Councillors for Carrville Ward of Belmont Parish on Thursday 6 May 2021 I, John Hewitt being the Returning Officer at the above election, report that the persons whose names appear below were duly elected Parish Councillors for Carrville Ward of Belmont Parish Name of Candidate Home Address Description (if any) APPLEBY 8 Carrsway, Carrville, Durham, Liberal Democrat John DH1 1BB CONWAY 116 Moor Crescent, Durham, DH1 Labour Party Pat 1DL KNIGHT 47 Swinside Drive, Durham, DH1 Labour Party Joe 1AF MAVIN 87 Grange Road, Belmont, Liberal Democrat Lesley