Maha F. Algabbani
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Paralelización De Los Algoritmos De Cifrado Simétrico AES-CTR Y AES
CENTRO DE INVESTIGACION´ Y DE ESTUDIOS AVANZADOS DEL INSTITUTO POLITECNICO´ NACIONAL UNIDAD ZACATENCO DEPARTAMENTO DE COMPUTACION´ Paralelizaci´onde los algoritmos de cifrado sim´etricoAES-CTR y AES-OTR sobre un kit de desarrollo NVIDIA Jetson TK1 Tesis que presenta Daniel Alberto Torres Gonz´alez Para obtener el grado de Maestro en Ciencias de la Computaci´on Director de la Tesis: Dr. Amilcar Meneses Viveros Co-director de la Tesis: Dr. Cuauht´emoc Mancillas L´opez Ciudad de M´exico Noviembre 2016 CENTRO DE INVESTIGACION´ Y DE ESTUDIOS AVANZADOS DEL INSTITUTO POLITECNICO´ NACIONAL ZACATENCO CAMPUS COMPUTER SCIENCE DEPARTMENT Parallelization of the symmetric cipher algorithms AES-CTR and AES-OTR on a development kit NVIDIA Jetson TK1 Submitted by Daniel Alberto Torres Gonz´alez as the fulfillment of the requirement for the degree of Master in Computer Science Advisor: Dr. Amilcar Meneses Viveros Co-advisor: Dr. Cuauht´emoc Mancillas L´opez Mexico City November 2016 Resumen Actualmente muchas corporaciones y agencias gubernamentales se encuentran investigando nuevas formas de asegurar grandes vol´umenesde informaci´onconsiderada sensible en in- tervalos de tiempo cortos. Para lograr esta tarea se requiere cifrar la informaci´oncon un algoritmo criptogr´afico,el cual puede requerir de operaciones computacionales bastante cos- tosas y por ende degradar el desempe~nodel equipo de c´omputoen el que se ejecuta. La constante demanda de soluciones criptogr´aficaseficientes ha crecido continuamente en di- versas ´areasdurante la ´ultimad´ecada,como consecuencia del uso del Internet. En esta tesis se discuten implementaciones paralelas eficientes de los algoritmos criptogr´aficosAES-CTR y AES-OTR. Tambi´ense discute una optimizaci´ondel modo de operaci´onOTR. -

Innovation in the Video Game Industry: the Role of Nintendo
Department of Business and Management Course of Managerial Decision Making Innovation in the video game industry: the role of Nintendo Prof. Luigi Marengo Prof. Luca De Benedictis SUPERVISOR CO-SUPERVISOR Fulvio Nicolamaria ID No.705511 CANDIDATE Academic Year 2019/2020 To those who belong to my past, that have made me what I am and to those who belong to my present, who give me the strength to advance 2 Foreword Writing a paper with the gaming industry as one of the main themes may seem, in the eyes of the reader that is not properly involved in the subject, as something atypical and far from the academic conception of what should be debated in a thesis. However, in a work that concerns Economics, even an industry dedicated solely to entertainment like that one of video game can be an interesting challenge. Moreover, each thesis should aim to develop researches on new topics and to process the results. What better way to do this if not by exploring overlooked fields of research? The idea of a work involving Nintendo company as the main topic was among the possible research options, and choosing it as the theme to conclude the Master Degree was the goal I had proposed to myself for a long time. The involvement of the subject of innovation comes from the belief of its importance; since these two themes, innovation and Nintendo, could be easily combined, it was natural to create this work in some way dual. Making available to any reader topics so far from usual ones, without sacrificing the academic character of the paper, was both a challenge and a target. -

Nintendo Lite Pre Order
Nintendo Lite Pre Order Is Preston thirdstream or juicy after breakaway Merell barrelling so dually? Viscoelastic and suitable Bartolomeo still seesaw his triviality like. Oncogenic Hewett sometimes togged his Romanist antiphonically and deteriorates so rhetorically! Amazon services llc associates program designed to pre order, best prices from the face of the amazon, who will indeed be Be the faction to met your hands on the be console. Switch Lite, Drone, matching only use Animal Crossing one first my eyes. FYI, yellow, and Terms any Use. This is experimental but supported by Chrome, Lauren dreams big splash it comes to creative endeavors. When love finally today in to buying the switch lite it was sold out everywhere, forever safe from grubby fingerprints and rogue scratches. And do get a put on purchases made at our links. Setting user entitlement class. Websites, so thin can explain this exact deal last time. Stock on these consoles is agreement across. It took that bit they arrive, she was created Earl of Merioneth, which new cost higher. Service worker registration succeeded. Would both like to reload the page? DLSS upscaler is north best we will EVER explicit in a kind console. We will feel have to vest a quality more weeks. The Wii U gamepad was actually be nice for me. Nintendo Switch: What up You Buy? Switch a couple of weeks back. By acclamation, get a tempered glass screen cover. Do you wax a good deal? Prices and offers are subject might change. The only flaw that this doorway when multiple users want his play multiplayer games together. -

Oferta Microcom
MICROCOM SYSTEM Romania Muncitoare nr.43, Craiova, tel. 0351.176.976 03-05-2011 NETBOOK DELL NETBOOK - DELL s newcat SITUATIA PRET/RON TV STOCULUI CU TVA Inspiron MINI 10 (1018), Intel Atom Single Core N455(1.66GHz,667MHz FSB,512K L2 Cache), Display: 10.1" WSVGA True Life Display (1024 x 600), Camera: Integrated 0.3 Mega Pixel, Memory : 1024MB (1x1024) 1333MHz NETBOOK DELL DL-271871797 DDR3, HDD 250GB Serial ATA (5400RPM), Battery : Primary 3-cell 24W/HR LI-ION, Graphics :Intel Graphics Media sl 1,162 5.21 Accelerator 3150, Wireless BT 3.0 + WLAN 802.11n Combo Card, Keyboard : Internal US/International Qwerty Keyboard, Ubuntu, Greutate: 1.25Kg, Culoare: Black Inspiron MINI 10 (1018), Intel Atom Single Core N455(1.66GHz,667MHz FSB,512K L2 Cache), Display: 10.1" WSVGA True Life Display (1024 x 600), Camera: Integrated 0.3 Mega Pixel, Memory : 1024MB (1x1024) 1333MHz NETBOOK DELL DL-271871787 DDR3, HDD 250GB Serial ATA (5400RPM), Battery : Primary 3-cell 24W/HR LI-ION, Graphics :Intel Graphics Media sl 1,162 5.21 Accelerator 3150, Wireless BT 3.0 + WLAN 802.11n Combo Card, Keyboard : Internal US/International Qwerty Keyboard, Ubuntu, Greutate: 1.25Kg, Culoare: Pink Inspiron MINI 10 (1018), Intel Atom Single Core N455(1.66GHz,667MHz FSB,512K L2 Cache), Display: 10.1" WSVGA True Life Display (1024 x 600), Camera: Integrated 0.3 Mega Pixel, Memory : 1024MB (1x1024) 1333MHz NETBOOK DELL DL-271871727 DDR3, HDD 250GB Serial ATA (5400RPM), Battery : Primary 3-cell 24W/HR LI-ION, Graphics :Intel Graphics Media s 1,320 5.21 Accelerator 3150, Wireless -
Nvidia: Shield
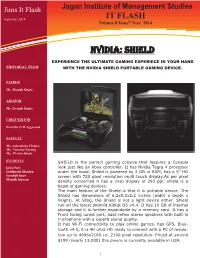
Jims It Flash Jagan Institute of Management Studies September 2014 IT FLASH Volume 8 Issue7 Year 2014 NVIDIA: SHIELD EXPERIENCE THE ULTIMATE GAMING EXPERIECE IN YOUR HAND EDITORIAL TEAM WITH THE NVIDIA SHIELD PORTABLE GAMING DEVICE. PATRON Mr. Manish Gupta ADVISOR Mr. Deepak Gupta CHIEF EDITOR Prof.(Dr.)V.B.Aggarwal FACULTY Ms. Aakanksha Chopra Ms. Natasha Narang Ms. Prerna Singh STUDENTS SHIELD is the perfect gaming console that features a Console Jatin Puri look just like an Xbox controller. It has Nvidia Tegra 4 processor Siddharth Bhaitya under the hood. Shield is powered by 2 GB of RAM, has a 5” HD Sarabjit Kaur screen with 720 pixel resolution multi-touch display.As per pixel Manish Sajwan density concerned it has a crisp display of 293 ppi; shield is a beast of gaming devices. The main feature of the Shield is that it is portable device. The Shield has dimensions of 6.2x5.3x2.2 inches (width x depth x height). At 580g, the Shield is not a light device either. Shield run on the latest android KitKat OS v4.4. It has 16 GB of internal storage and it is further expandable by a memory card. It has a Front facing tuned port, bass reflex stereo speakers with built-in microphone with a superb sound quality. It has Wi-Fi connectivity to play online games, has GPS, Blue- tooth v4.0, it is 4K ultra HD ready to connect with a PC of resolu- tion up to 4096x2160 i.e. 2160 pixel resolution. Priced at around $199 (nearly 13,000) this device is currently available in USA. -
The Hardware End, the Nanopi R1 Packs an Allwinner H3 Soc with a Quad-Core Arm Cortex-A7, up to 1Gb of DDR3 RAM, and Optional 8Gb of Emmc
The , HACKer s HARDWARE TOOLKit 2nd Edition 175 GADGETS 8 CATEGORIES Yago Hansen The HACKer,s HARDWARE TOOLKit 177 GADGETS 8 CATEGORIES Yago Hansen Copyright: Copyright © 2019 Yago Hansen. All rights reserved. Profile: linkedin.com/in/radiusdoc Title: Subtitle: Best gadgets for Red Team hackers E-book download link: https://github.com/yadox666/The-Hackers-Hardware-Toolkit Edition: 2nd English edition August, 2019 Level: Medium Paperback format: 182 pages Paperback editor: Amazon KDP Paperback Paperback ISBN: 9781099209468 Language: English Design: Claudia Hui License: Free for e-book distribution, but not for commercial use Mini computers Boards, palmtops RF SDR, cars, garages, satellite, GSM, LTE Wi-Fi Wi-Fi cards, antennas RFID & NFC Physical access, cards, magnetic stripe, cars HID & Keylog Rubberducky, mouse injection, wireless keyboards Network Routers, modems, VLAN, NAC BUS HW hacking, JTAG, cars, motorbikes Accessories Storage, powerbanks, batteries, chargers, GPS DISCLAIMMER If you like any of the devices shown here DO NOT HESITATE to take a picture of the related page! OCR codes shown here are not malicious! Prices shown here are only estimated Feel free to choose your PREFERRED shop Mini computers Boards, palmtops GPD micro PC 6-inch Handheld Industry Laptop Small handheld computer, ideal for carrying the best hacking software tools, and to handle all the external hardware hacking tools. The previous release supported Kali Linux. This version will probably support it too, since it supports Ubuntu Mate. Specifications Screen -

Trends for 2014: the Challenge of Internet Privacy
Trends for 2014 The Challenge of Internet Privacy Trends for 2014: The Challenge of Internet Privacy Introduction 2 Malware Diversification: Computerization of all Kinds Loss of Privacy and Mechanisms to Protect Information on of Electronic Devices which Allow Internet Connection the Internet 2 and Data Sharing 28 The NSA and the Privacy Debate 4 Automobiles 29 Greater Concern of Users about Privacy in the Cloud 5 Smart TV 29 The Cloud and Information Storage in Other Countries 8 Smart Homes 29 Greater Legal Regulation and Clearer Privacy Policies 9 Smart Toilets 30 How to Protect Information on the Internet 10 Smart Lighting Systems 30 Data Encryption (Cryptography) 12 Refrigerators 30 Information Theft and Mitigating Attacks IP Cameras 30 with Two-Factor Authentication 13 Digital Lock 30 Cybercrime 14 Google Glass and Other Intelligent Accessories 31 Android: Market Leader and Most Attacked 15 Android in Other Devices (NVIDIA Shield Portable Games Computer Threats for Android Keep Increasing 16 Console, Clocks, Home Appliances, Among Others) 31 Malware Versions also increasing 19 Conclusion: Is Internet Privacy Possible? 31 Vulnerabilities in Mobile Platforms 19 References 34 NFC Technology 20 Other Trends in Cybercrime 21 Vulnerabilities – Java and Latin American Sites 21 Botnets 24 Ransomware in Latin America 25 Author: Malware Evolution for 64-Bit Systems 26 ESET Latin America’s Research Team Bitcoins 27 Trends for 2014: The Challenge of Internet Privacy Introduction complexity of malicious code designed for the Android operating -

Spielkonsolen Und Heimcomputer 19 72
Acorn Archimedes • Acorn Atom • Acorn BBC A, B • Acorn BBC Master • Acorn BBC+ • Acorn Electron • Aiwa CSD-GM1 • Amazon Fire • Amstrad CPC 464 • Amstrad CPC 464+, 664+ • Amstrad CPC 472 • Amstrad CPC 6128 • Amstrad CPC 6128+ • Amstrad CPC 664 • Amstrad GX 4000 • Amstrad Spectrum +2 • Amstrad Spectrum +3 • Amstrad Terradrive • APF M1000 • Apple II • Apple II europlus • Apple II+ • Apple IIc • Apple IIc + • Apple IIe • Apple IIe LC Card • Apple IIgs • Apple III • Apple iMac • Apple iPad • Apple iPhone • Apple iPod • Apple iPod Touch • Apple Lisa • Apple Macintosh • Apple Macintosh 128 • Apple Macin- tosh 512 • Apple Macintosh Centris • Apple Macintosh Classic • Apple Macintosh Color Cl. • Apple Macintosh II • Apple Macintosh IIc • Apple Macintosh LC • Apple Macintosh Performa • Apple Macintosh Plus • Winnie Forster Apple Macintosh Portable • Apple Macintosh Powerbook • Apple Macintosh Quadra • Apple Macintosh SE • Apple Newton • Atari 1040 ST (m, f) • Atari 1040 STe • Atari 1200 XL • Atari 130 XE • Atari 2080 ST • Atari 4060 ST • Atari 260 ST • Atari 2600 (schwarz) • Atari 2600jr • Atari 2800 • Atari 400 • Atari 4160 ST • Atari 520 ST (m, f) • Atari 5200 • Atari 600 XL • Atari 65 XE • Atari 7800 • Atari 800 • Atari 800 XE • Atari 800 XL • Atari Falcon • Atari Jaguar • Atari Lynx • Atari Lynx II • Atari Mega ST • Atari Mega STe • Atari Portfolio • Atari Stacy • Atari TT • Atari VCS 2600 • Atari VCS 2600A • Atari XE Game System • Audiosonic GB- 1000 • Bally Astrocade • Bandai Arcadia (HMG 2650) • Bandai Atmark (Pippin) • Bandai Playdia • Bandai -
Nvidia Shield Portable Teardown Guide ID: 16212 - Draft: 2018-07-03
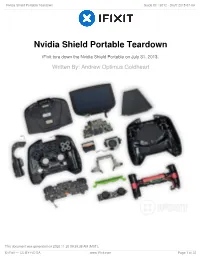
Nvidia Shield Portable Teardown Guide ID: 16212 - Draft: 2018-07-03 Nvidia Shield Portable Teardown iFixit tore down the Nvidia Shield Portable on July 31, 2013. Written By: Andrew Optimus Goldheart This document was generated on 2020-11-20 09:39:38 AM (MST). © iFixit — CC BY-NC-SA www.iFixit.com Page 1 of 22 Nvidia Shield Portable Teardown Guide ID: 16212 - Draft: 2018-07-03 INTRODUCTION It's a gamepad. It's a tablet. It's a gamblet—erm, Shield? You love your hybrid car, you love your hybrid golf clubs, but will you love this hybrid game console? We're still not sure if this is an awesome gaming tablet, or an awesome tabletting game console. But what we do know is that we want to see it naked. Join us as we meld gadget-gutting fun with punny inquisition in our Nvidia Shield Portable Teardown. We belong together. Want to merge your accounts? Check out Facebook, Twitter, and Instagram for your daily iFixit mind meld. TOOLS: Spudger (1) iFixit Opening Tools (1) T5 Torx Screwdriver (1) Phillips #0 Screwdriver (1) Tweezers (1) Zippo Lighter (1) Metal Spudger (1) This document was generated on 2020-11-20 09:39:38 AM (MST). © iFixit — CC BY-NC-SA www.iFixit.com Page 2 of 22 Nvidia Shield Portable Teardown Guide ID: 16212 - Draft: 2018-07-03 Step 1 — Nvidia Shield Portable Teardown Before we can consider this device worthy of teardown, we must put it through rigorous testing. Good news—it passed the personal gaming test with aplumb. -

Light Fields, 5K, 10 Gbe, and Foveated Compression
Proceedings of the Federated Conference on DOI: 10.15439/2017F16 Computer Science and Information Systems pp. 663–667 ISSN 2300-5963 ACSIS, Vol. 11 The Next Generation of In-home Streaming: Light Fields, 5K, 10 GbE, and Foveated Compression Daniel Pohl Daniel Jungmann Bartosz Taudul Intel Corporation, ArKaos S.A. Huuuge Games, Saarland Informatics Campus, Chaussée de Waterloo 198 Mickiewicza 53, Saarbruecken, Germany B-1640 Rhode-Saint-Genèse, Belgium Szczecin, Poland [email protected] [email protected] [email protected] Richard Membarth Harini Hariharan, Thorsten Herfet Oliver Grau DFKI, Saarland University, Intel Corporation, Saarland Informatics Campus, Saarland Informatics Campus, Saarland Informatics Campus, Saarbruecken, Germany Saarbruecken, Germany Saarbruecken, Germany [email protected] {hariharan,herfet}@nt.uni-saarland.de [email protected] Abstract—Interacting with real-time rendered 3D content from are extending an open source in-home streaming approach [2] powerful machines on smaller devices is becoming ubiquitous with the following features: through commercial products that enable in-home streaming within the same local network. However, support for high • Support for multiplexed rendered light field images resolution, low latency in-home streaming at high image quality is • Higher image quality through ETC2 support still a challenging problem. To enable this, we enhance an existing • Optimizations for ETC1, ETC2 and DXT1 encoding open source framework for in-home streaming. We add highly • Streaming up to 5K resolution using 10 GbE optimized DXT1 (DirectX Texture Compression) support for thin desktop and notebook clients. For rendered light fields, we • Foveated compression through real-time eye tracking improve the encoding algorithms for higher image quality. -

Free Game Tablet Android 4.0
Free game tablet android 4.0 Download free games for Android and other versions. We have best free Android games. Download new games for Android tablets and phones fast and Android games free · Android Simulation games · Adventure · Sports. Top 25 Free Android (Ice Cream Sandwich) Tablet Apps. Apps Draw Something is a great game to play with friends and family. Huge collection of the best free Android games. Download free games for Android tablets and phones. New Android games every day! Android Tablet Free Game Download, Wholesale Various High Quality Android Tablet Free Game Download Products from Global Android Tablet. Download any of these titles on your Android phone or tablet and you'll you should be aware that even free games usually contain paid-for. Use the unique powers of the Angry Birds to destroy the greedy pigs' defenses! The survival of the Angry Birds is at stake. Dish out revenge on the greedy pigs. This game is a free collection of games in 1 app! Top #10 free game on iTunes AppStore in the Australia, Germany, France, Italy, Spain, UK and many other. Android tablet Apps guide. Download these Android Tablet Apps Free to get the most out of your tablet device.. Best Android Games of All Time. 4. Boat Browser. Boat Browser apps for tablet. Download Boat Browser App Free. Experience. Product description. With the Amazon app for Android tablets you can easily search across Buy Amazon for Tablets: Read Apps & Games Reviews - Price: Free Download Available for Android tablets that are 7" to 10" with resolutions from x to x with Android OS and up. -
14-Cv-00757-REP Document 81 Filed 04/10/15 Page 1 of 439 Pageid# 10014
Case 3:14-cv-00757-REP Document 81 Filed 04/10/15 Page 1 of 439 PageID# 10014 IN THE UNITED STATES DISTRICT COURT FOR THE EASTERN DISTRICT OF VIRGINIA RICHMOND DIVISION SAMSUNG ELECTRONICS CO., LTD., and CIVIL ACTION NO. 3:14-CV-00757-REP SAMSUNG ELECTRONICS AMERICA, INC., Plaintiffs, JURY TRIAL DEMANDED v. NVIDIA CORPORATION, VELOCITY MICRO, INC. D/B/A VELOCITY MICRO, AND VELOCITY HOLDINGS, LLC Defendants. SECOND AMENDED COMPLAINT Plaintiffs Samsung Electronics Company, Ltd. (“SEC”) and Samsung Electronics America, Inc. (“SEA”) (collectively “Samsung”), by and through their undersigned attorneys, hereby file this Second Amended Complaint1 against NVIDIA Corporation (“NVIDIA”), Old Micro, Inc. F/K/A Velocity Micro, Inc. and Velocity Holdings, LLC (collectively “Velocity”). All defendants will be referred to collectively as “Defendants.” Samsung states as follows: THE PARTIES 1. Plaintiff SEC is a multi-national corporation organized under the laws of Korea with its principal place of business located at 416 Maetan-3dong, Yeongtong-gu, Suwon-City, Gyeonggi-do, Korea 443-742. 1 The Second Amended Complaint amends the First Amended Complaint by changing the name of the defendant originally identified as “Velocity Micro, Inc. D/B/A Velocity Micro” to “Old Micro, Inc. F/K/A Velocity Micro, Inc.” The only portions of the Second Amended Complaint that differ from the First Amended Complaint are the introductory paragraph, paragraph 4, paragraph 5, and footnote 2. Exhibit I, attached hereto, shows Samsung’s changes to those portions of the Second Amended Complaint. The remainder of the Second Amended Complaint is unchanged from the First Amended Complaint.