Environmental and Social Safeguards Audit Public Disclosure Authorized
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Spatial Pattern of Housing Quality in Abuja, Nigeria
International Journal of Coal, Geology and Mining Research Vol.2, No.1, pp.1-20, May 2020 Published by European Centre for Research Training and Development UK(www.eajournals.org) SPATIAL PATTERN OF HOUSING QUALITY IN ABUJA, NIGERIA Saliman Dauda Department of Urban and Regional Planning, Baze University, Abuja, Nigeria ABSTRACT: The study attempted evaluation of Spatial Pattern of Housing Quality of Abuja, Nigeria. The identified 62 political wards were stratified into their various Area Councils namely, Abuja Municipal Area Council (AMAC), Bwari Area Council, Gwagwalada Area Council, KwaliArea Council, Kuje Area Council and Abaji Area Council. Using systematic random sampling, 3593, 1002,641,290,341 and 202 houses were selected in AMAC, Bwari Area Council, Gwagwalada Area Council, Kwali Area Council, Kuje Area Council and Abaji Area Council respectively to give a total of 6069 houses. Socioeconomic characteristics of the households revealed that the youth constituted 14.2% of the respondents, while 79.99% of the respondents were also found to be in the age bracket of 31-60 years. Analysis of Variance (ANOVA) confirmed, that there were significant differences in the age distribution of the residents (F = 4.11, p = 0.005). Analysis of spatial pattern of housing quality using Factor Analysis revealed that housing location quality attributes factor, recorded highest influence on the spatial pattern of housing quality in Area Councils, such as AMAC, Bwari Area Council and Gwagwalada Area Council. The study concluded that a general hierarchical trend in spatial pattern of housing quality had been figured out in Abuja, where housing quality was observed to decrease with increase in distance from the Central Business District(CBD). -

Frugivorous Bird Species Diversity in Relation to the Diversity of Fruit
ISBN: 2141 – 1778 jfewr ©2016 - jfewr Publications E-mail:[email protected] 80 FRUGIVOROUS BIRD SPECIES DIVERSITY IN RELATION TO THE DIVERSITY OF FRUIT TREE SPECIES IN RESERVED AND DESIGNATED GREEN AREAS IN THE FEDERAL CAPITAL TERRITORY, NIGERIA 1Ihuma, J.O; Tella, I. O2; Madakan, S. P.3 and Akpan, M2 1Department of Biological Sciences, Bingham University, P.M.B. 005, Karu, Nasarawa State, Nigeria Email:[email protected] 2Federal University of Technology, Yola, Nigeria, Department of Forestry and Wildlife Management. 3University of Maiduguri, Borno, Nigeria, Department of Biological Sciences ABSTRACT The diversity of frugivorous bird species in relation to tree species diversity was investigated in Designated and Reserved Green Areas of Abuja, Nigeria. The study estimated, investigated and examined trees species and avian frugivore in terms of their diversity. Point-Centered Quarter Method (PCQM) was used for vegetation analysis while random walk and focal observation was used for bird frugivore identification and enumeration. data was collected from six locations coinciding with the local administrative areas within the Federal Capital Territory. These were, the Abuja Municipal Area Council (AMAC), Abaji, Bwari, Gwagwalada, Kuje and Kwali. AMAC is designated as urban while the remaining five sites are designated as sub-urban. The highest number of fruit tree species was encountered in AMAC (30), followed by Abaji (29) while 27, 25, 19 and 11 fruit tree species were encountered in Kwali, Bwari Gwagwalada and Kuje respectively. The similarity or otherwise dissimilarity in fruit tree species composition between each pair of the enumerated sites showed Gwagwalada and Kuje as the most similar, and the similarity or otherwise dissimilarity in frugivorous bird species composition between each pair of the enumerated showed higher species similarity between the AMAC and each of the other sites, and between each pair of the sites than that of the fruit trees in the respective sites. -

Nigeria - Accessibility to Emonc Facilities in the State of Cross River
Nigeria - Accessibility to EmONC facilities in the State of Cross River Last Update: March 2016 Nigeria - Accessibility to EmONC facilities for the Cross River State Table of Contents Acknowledgements ..................................................................................................................... 4 1. Introduction ............................................................................................................................. 5 2. Measured indicators and assumptions .................................................................................... 5 3. Tool used for the different analyses: AccessMod 5.0 ............................................................. 7 4. Data and national norms used in the different analyses .......................................................... 8 4.1 Statistical Data ............................................................................................................... 9 4.1.1 LGA Number of pregnant women for 2010 and 2015 ........................................... 9 4.2 Geospatial Data ........................................................................................................... 12 4.2.1 Administrative boundaries and extent of the study area ...................................... 13 4.2.2 Geographic location of the EmONC facilities and associated information ......... 17 4.2.4 Transportation network ........................................................................................ 26 4.2.5 Hydrographic network ........................................................................................ -

Developing the Knowledge, Skills and Talent of Youth to Further Food Security and Nutrition
DEVELOPING THE KNOWLEDGE, SKILLS AND TALENT OF YOUTH TO FURTHER FOOD SECURITY AND NUTRITION The following case study was received as a result of a call issued by the Committee on World Food Security for case studies highlighting examples of initiatives aimed at ‘Developing the knowledge, skills and talent of youth to further food security and nutrition’. The cases received provide the background for a discussion of lessons learned and potential policy implications at a special event on October 15th, 2015 during CFS 42. Find out more at www.fao.org/cfs/youth. Background The registrations of farmers in the Federal Capital Territory in which to encourage the timely distribution of farming input, e.g The Fertilizers and the seedlings and other Agricultural inputs both to the youth and the adult, and the documentations of the various exercises in the facilitation of food distribution, nutrition development and encouraged the farmers to get access to farming input and cultivation of land which is being done in the Five areas council of the Federal Capital Territory Abuja, Nigeria ,Municipal , Gwagwalada, Abaji, Kwali , Bwari. Selected Schools were taken and farmers which includes youth were asked to go and register their names and documentation of some information. This is done with the help of the Agricultural Development Programe , International Fertilizers Development company and Michael Adedotun Oke Foundation. And a data of farmers were produce. Challenges Most of the youths that came for the farmers registration does not have the necessary identification to been register during the period. The cost of moving to the registration centre’s as a great implication of the youth due to the cost implications. -
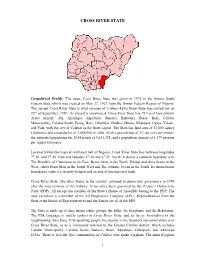
Cross River State
CROSS RIVER STATE Geopolitical Profile: The name Cross River State was given in 1976 to the former South Eastern State which was created on May 27, 1967 from the former Eastern Region of Nigeria. The current Cross River State is what remains of it when Akwa Ibom State was carved out on 23rd of September, 1987. As presently constituted, Cross River State has 18 Local Government Areas namely; Abi, Akamkpa, Akpabuyo, Bakassi, Bekwarra, Biase, Boki, Calabar Municipality, Calabar South, Etung, Ikom, Obanliku, Obubra, Obudu, Odukpani, Ogoja, Yakurr, and Yala; with the city of Calabar as the State capital. The State has land area of 23,000 square kilometres and a population of 2,888,966 in 2006. With a growth rate of 2.9 per cent per annum, the estimated population for 2014 stands at 3,631,328, and a population density of 1,579 persons per square kilometre. Located within the tropical rainforest belt of Nigeria, Cross River State lies between longitudes 7⁰ 50’ and 9⁰ 28’ East and latitudes 4⁰ 28’and 6⁰ 55’ North. It shares a common boundary with The Republic of Cameroun in the East, Benue State in the North, Ebonyi and Abia States in the West, Akwa Ibom State in the South West and The Atlantic Ocean in the South. Its international boundaries make it a security hotspot and an axis of international trade. Cross River State, like other States in the country, returned to democratic governance in 1999 after the interventions of the military. It has since been governed by the People’s Democratic Party (PDP). -

NIGERIA: Registration of Cameroonian Refugees September 2019
NIGERIA: Registration of Cameroonian Refugees September 2019 TARABA KOGI BENUE TAKUM 1,626 KURMI NIGERIA 570 USSA 201 3,180 6,598 SARDAUNA KWANDE BEKWARA YALA DONGA-MANTUNG MENCHUM OBUDU OBANLIKU ENUGU 2,867 OGOJA AKWAYA 17,301 EBONYI BOKI IKOM 1,178 MAJORITY OF THE ANAMBRA REFUGEES ORIGINATED OBUBRA FROM AKWAYA 44,247 ABI Refugee Settlements TOTAL REGISTERED YAKURR 1,295ETUNG MANYU REFUGEES FROM IMO CAMEROON CROSS RIVER ABIA BIOMETRICALLY BIASE VERIFIED 35,636 3,533 AKAMKPA CAMEROON Refugee Settlements ODUKPANI 48 Registration Site CALABAR 1,058MUNICIPAL UNHCR Field Office AKWA IBOM CALABAR NDIAN SOUTH BAKASSI667 UNHCR Sub Office 131 58 AKPABUYO RIVERS Affected Locations 230 Scale 1:2,500,000 010 20 40 60 80 The boundaries and names shown and the designations used on this map do not imply official Kilometers endorsement or acceptance by the United Nations. Data Source: UNHCR Creation Date: 2nd October 2019 DISCLAIMER: The boundaries and names shown, and the designations used on this map do not imply official endorsement or acceptance by the United Nations. A technical team has been conducting a thorough review of the information gathered so as to filter out any data discrepancies. BIOMETRICALLY VERIFIED REFUGEES REGISTRATION TREND PER MONTH 80.5% (35,636 individuals) of the total refugees 6272 counteded at household level has been 5023 registered/verified through biometric capture of iris, 4025 3397 fingerprints and photo. Refugee information were 2909 2683 2371 also validated through amendment of their existing 80.5% information, litigation and support of national 1627 1420 1513 1583 586 VERIFIED documentations. Provision of Refugee ID cards will 107 ensure that credible information will effectively and efficiently provide protection to refugees. -

The Cross River Super Highway: Fact Sheet
The Cross River Super Highway: Fact Sheet TIMELINE After May 2015: Super highway construction announced severally by Governor FOREST ASSETS Ayade, together with the installation of a deep sea port in the mangroves. Cross River State is host to the largest remaining rainforests of Nigeria. September 2015: Groundbreaking ceremony and visit by President Buhari The Cross River National Park has two distinct, non-contiguous divisions: Oban postponed because of non-existing Environmental Impact Assessment. Re-routing and Okwangwo, with a total area of about 4,000 square km. Protected forests of highway to move it outside the National Park. also exist outside the boundaries of the National Park. In total, Cross River 20 October 2015: Buhari performs the groundbreaking ceremony at Obong State hosts at least 5,524 sq km of protected rainforests. Akamkpa LGA, Cross Rivers State. One of the highest bio-diversity forests in the world, Cross River State is home 22 January 2016: Cross River Government Gazette announces revocation of all to highly threatened species including Cross River gorilla, Nigeria-Cameroon occupancy titles within a 20 kilometre wide corridor of land along the highway chimpanzee, drill monkeys and many others, and hosts about 1,568 plant route. species, of which 77 are endangered including medicinal plants and orchids. February, 2016: Bulldozers enter the Ekuri-Eyeyeng, Etara and Okuni areas and Two new species of orchids were found to be unique to Cross River forests: start clearing and felling of trees. Communities in Old and New Ekuri prevent Tridactyle sp nov. and Hebenaria sp nov. bulldozers from logging in their forest. -

Rainfall Variations As the Determinant of Malaria in the Federal Capital Territory Abuja, Nigeria
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by International Institute for Science, Technology and Education (IISTE): E-Journals Journal of Environment and Earth Science www.iiste.org ISSN 2224-3216 (Paper) ISSN 2225-0948 (Online) Vol.4, No.20, 2014 Rainfall Variations as the Determinant of Malaria in the Federal Capital Territory Abuja, Nigeria Yahaya Usman Badaru 1* Akiode Olukemi Adejoke 2 Ahmed Sadauki Abubakar 3 Mohammed Ahmed Emigilati 4 1. Applied Remote Sensing Laboratory, Department of Geography, School of Natural and Applied Science 2. Federal University of Technology, Minna, Nigeria 3. University of Abertay, Dundee, Scotland-UK 4. Department of Geography, Federal University of Technology, Minna, Nigeria 5. Department of Geography, Federal University of Technology, Minna, Nigeria *Emails of the corresponding authors : [email protected] ; [email protected] Abstract This study highlights the increasing interest in identifying the parameters adequate to measure rainfall and wet day’s variations as the determinant of malaria occurrences and distribution for a period of twelve months (2012) in the Federal Capital Territory. Satellite data were developed to identify malaria risk area and to evaluate amounts of rainfall and the durations of wet or rainy days conducive to malaria outbreaks at appropriate scales. Secondly, the studies examine the correlation of monthly and annual malaria cases, and rainfall amounts, including wet days with a lag time of one year. The result of correlation analysis shows that relationship exists between the observed weather variables and malaria. The coefficients of determination R2 of rainfall influencing malaria is 0.3109 (31.1%) and wet days influencing malaria is 0.3920 (39.2%). -

Anti-Bullet Charms, Lie-Detectors and Street Justice: the Nigerian Youth and the Ambiguities of Self-Remaking
At the International Conference, Youth and the Global South: Dakar, Senegal, 13 - 15 October 2006. Anti-Bullet Charms, Lie-Detectors and Street Justice: the Nigerian Youth and the Ambiguities of Self-Remaking Babson Ajibade Cross River University of Technology, Calabar, Nigeria. Abstract The failure of the Nigerian state, its police and judiciary to provide security has eroded citizenship trust. But this failure has tended to implicate the so-called ‘elders’ normally in charge of village, township and urban life-worlds. Disappointedly, Nigeria’s ‘young generations’ creatively assume unofficial yet central positions of ambiguity in the restoration of social order and security. In urban, peri-urban and rural locations ethnic militias and private youth gangs operate as alternative police and adjunct judiciary in place of the state’s failed institutions. These militia and youth gangs use guns, charms and violence to contest pressing concerns and negotiate contemporary realities. While processes of political economy and globalization remain unfavourable, youths – as agents and subjects of social change – are able to subvert status quo by deploying materials appropriated from the local and the global to define ambiguous positions. In one such hybridised situation, youths in Obudu1 have created a device they term ‘lie-detector’ – by fusing ideas gleaned from local and global media spaces. Using this device as central but unconventional social equipment and, drawing validation from traditional social systems, these youths are negotiating new selves in a contemporary milieu. Using the analysis of social practice and popular representation of youth roles, activities and initiatives in Nigeria, this paper shows how sociality and its contestation in urban life moves the Nigerian youth from the periphery to the centre of social, political and economic nationalisms. -

Parametric Investigation of Soil Susceptibility to Compaction Using Temperature Deviation Curves
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Covenant University Repository Science Journal of Civil Engineering & Architecture Published By ISSN: 2276-6332 Science Journal Publication http://www.sjpub.org/sjcea.html International Open Access Publisher © Author(s) 2012. CC Attribution 3.0 License. Research Article Volume 2012, Article ID sjcea-279, 6 Pages, 2012. doi: 10.7237/sjcea/279 Parametric Investigation of Soil Susceptibility to Compaction Using Temperature Deviation Curves Uno E Uno, Moses E Emetere, Adelabu, J. S.* Department of Physics, Federal University of Technology Minna P.M.B 65, Minna. * Department of Physics, University of Abuja, Nigeria. Accepted 17�� March, 2012 capacity point, when a condition known as the optimum Abstract moisture content for compaction is reached. ⁽⁴,¹⁴⁾ The proper estimation of soil moisture content is a fundamental Soil compaction can be explained using basic properties of soil. issue as well in food security research, land management Cohesive soil sample were collected from five major region of the systems, pollution detection, nutrient flows, (wild-)fire main site of investigation. Unlike other method of analyzing soil compaction, temperature deviation curves were used as the detection, (desert) locust and carbon balance modeling.⁽⁴⁾ determinant for testing for compaction. It was discovered also that Soil moisture content is one of the prime environmental the temperature deviation curves can be used to find the annual variables related to land surface climatology, hydrology amplitude of the surface soil temperatures. Soils in Abuja displayed and ecology. It has been discovered that plastic flow some degree of compaction except for Gwagwalada that showed contributes to the complete destruction of soil structure negligible compaction. -

Evaluation of Intensity of Urinary Schistosomiasis in Biase and Yakurr Local Government Areas of Cross River State, Nigeria Afte
Research Journal of Parasitology 10 (2): 58-65, 2015 ISSN 1816-4943 / DOI: 10.3923/jp.2015.58.65 © 2015 Academic Journals Inc. Evaluation of Intensity of Urinary Schistosomiasis in Biase and Yakurr Local Government Areas of Cross River State, Nigeria after Two Years of Integrated Control Measures 1H.A. Adie, 1A. Oyo-Ita, 2O.E. Okon, 2G.A. Arong, 3I.A. Atting, 4E.I. Braide, 5O. Nebe, 6U.E. Emanghe and 7A.A. Otu 1Ministry of Health, Calabar, Nigeria 2Department of Zoology and Environmental Biology, University of Calabar, Nigeria 3Department of Medical Microbiology and Parasitology, University of Uyo/University of Uyo Teaching Hospital, Uyo, Nigeria 4Federal University, Lafia, Nasarawa State, Nigeria 5Federal Ministry of Health, Abuja, Nigeria 6Department of Medical Microbiology/Parasitology, University of Calabar, Nigeria 7Department of Internal Medicine, University of Calabar, Calabar, Nigeria Corresponding Author: H.A. Adie, Ministry of Health, Calabar, Nigeria ABSTRACT A parasitological mapping of urinary schistosomiasis using filtration method was conducted in Biase and Yakurr LGAs of Cross River State, Nigeria by the Neglected Tropical Diseases Control unit in collaboration with the schistosomiasis/soil transmitted helminths unit of the Federal Ministry of Health, Nigeria in November 2012. The results of the study revealed a mean urinary schistosomiasis prevalence of 49% for the six schools under study in Biase and 30% for the six schools under study in Yakurr LGA. The mean ova load was 0.9 for males and 0.8 for females in the two LGAs. Integrated control measures put in place, included chemotherapy of infected individuals with praziquantel and health education on the predisposing factors responsible for the transmission of urinary schistosomiasis. -

List of Candidates FCT Area Council Election 12 February 2022
Final List of Candidates FCT Area Council Election 12 February 2022 www.inecnigeria.org FCT AreaCouncil Elections 3 Table of Contents 03 Introduction 04 Abaji AMAC 10 Bwari 24 35 Gwagwalada Kuje 46 Kwali 52 Summary 58 FCT AreaCouncil Elections 2 Introduction The Independent National Electoral Commission (INEC) is empowered by Section 103(1) of the Electoral Act 2010 (as amended) to conduct elections into the offices of Chairman, Vice Chairman and members of the Area Councils of the Federal Capital Territory (FCT). Pursuant to this power, the Commission will conduct elec- tion into these positions in the FCT Area Councils on Saturday 12th February 2022. In furtherance of the Commission’s continued effort to make information on the candidates contesting for elections available to Nigerians as required by Section 34 of the Electoral Act, this booklet provides detailed information on the particu- lars of candidates for the 2022 FCT Area Council election: their political parties, age, gender, disability status and educational qualifications. The FCT Area Council has a total of 68 constituencies for 6 chairmen and 62 coun- cillors. The election to the chairmanship positions will be contested by 55 candi- dates (52 male and 3 female) while the vice-chairmanship consists of 47 male and 8 female candidates sponsored by 14 political parties. The 363 candidates contest- ing for the councillorship positions consist of 332 males and 31 female contestants. Overall, some 473 candidates and their running mates are vying for 68 elective positions in the FCT. In addition to this booklet, the list is also published in the Commission’s FCT office as well as our website and social media platforms both as a legal requirement and for public information.