Disseminated Verruciform Xanthoma: a Case Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Glossary for Narrative Writing
Periodontal Assessment and Treatment Planning Gingival description Color: o pink o erythematous o cyanotic o racial pigmentation o metallic pigmentation o uniformity Contour: o recession o clefts o enlarged papillae o cratered papillae o blunted papillae o highly rolled o bulbous o knife-edged o scalloped o stippled Consistency: o firm o edematous o hyperplastic o fibrotic Band of gingiva: o amount o quality o location o treatability Bleeding tendency: o sulcus base, lining o gingival margins Suppuration Sinus tract formation Pocket depths Pseudopockets Frena Pain Other pathology Dental Description Defective restorations: o overhangs o open contacts o poor contours Fractured cusps 1 ww.links2success.biz [email protected] 914-303-6464 Caries Deposits: o Type . plaque . calculus . stain . matera alba o Location . supragingival . subgingival o Severity . mild . moderate . severe Wear facets Percussion sensitivity Tooth vitality Attrition, erosion, abrasion Occlusal plane level Occlusion findings Furcations Mobility Fremitus Radiographic findings Film dates Crown:root ratio Amount of bone loss o horizontal; vertical o localized; generalized Root length and shape Overhangs Bulbous crowns Fenestrations Dehiscences Tooth resorption Retained root tips Impacted teeth Root proximities Tilted teeth Radiolucencies/opacities Etiologic factors Local: o plaque o calculus o overhangs 2 ww.links2success.biz [email protected] 914-303-6464 o orthodontic apparatus o open margins o open contacts o improper -

Bilateral Lower Extremity Hyperkeratotic Plaques: a Case Report of Ichthyosis Vulgaris
Faculty & Staff Scholarship 2015 Bilateral lower extremity hyperkeratotic plaques: a case report of ichthyosis vulgaris Hayley Leight Zachary Zinn Omid Jalali Follow this and additional works at: https://researchrepository.wvu.edu/faculty_publications Clinical, Cosmetic and Investigational Dermatology Dovepress open access to scientific and medical research Open Access Full Text Article CASE REPORT Bilateral lower extremity hyperkeratotic plaques: a case report of ichthyosis vulgaris Hayley Leight Abstract: Here, we report a case of a middle-aged woman presenting with severe, long-standing, Zachary Zinn hyperkeratotic plaques of the lower extremities unrelieved by over-the-counter medications. Omid Jalali Initial history and clinical findings were suggestive of an inherited ichthyosis. Ichthyoses are genetic disorders characterized by dry scaly skin and altered skin-barrier function. A diagnosis Department of Dermatology, West Virginia University, of ichthyosis vulgaris was confirmed by histopathology. Etiology, prevalence, and treatment Morgantown, WV, USA options are discussed. Keywords: filaggrin gene, FLG, profilaggrin, keratohyalin granules, hyperkeratosis Introduction For personal use only. Inherited ichthyoses are a diverse group of genetic disorders characterized by dry, scaly skin; hyperkeratosis; and altered skin-barrier function. While these disorders of cutaneous keratinization are multifaceted and varying in etiology, disruption in the stratum corneum with generalized scaling is common to all.1–4 Although not entirely known -

Skin Brief Articles
SKIN BRIEF ARTICLES Nab-paclitaxel/gemcitabine Induced Acquired Ichthyosis Adriana Lopez BAa, Joel Shugar MDb, and Mark Lebwohl MDc aColumbia University Vagelos College of Physicians and Surgeons, New York, NY bIcahn School of Medicine at Mount Sinai, Department of Otolaryngology, New York, NY cIcahn School of Medicine at Mount Sinai, Department of Dermatology, New York, NY ABSTRACT The ichthyoses are a diverse group of cutaneous disorders characterized by abnormalities in cornification. The majority of ichthyoses are inherited with childhood presentation and new onset ichthyosis in adulthood warrants further medical evaluation. Though most well recognized for its association with Hodgkin’s disease, acquired ichthyosis (AI) has been linked to a number of inflammatory, autoimmune, and endocrine processes. However, drug- induced AI is exceedingly rare and remains a poorly understood entity. Here we report a case of a male patient who developed AI while receiving nab-paclitaxel plus gemcitabine for treatment of pancreatic adenocarcinoma. months prior, the patient was first seen for INTRODUCTION recurrent, self-healing, pruritic erythematous Acquired ichythyosis (AI) is an uncommon papules. Punch biopsy was performed which non-inherited cutaneous disorder of showed an atypical cellular infiltrate of abnormal keratinization that is most scattered large CD30+ cells with clonal T-cell frequently associated with underlying receptor-β gene rearrangement. Though the malignancy. Drug induced AI is uncommon clinicopathologic diagnosis was most and has been rarely linked to consistent with lymphomatoid papulosis chemotherapeutic agents. Herein, we report (LyP), imaging was pursued to exclude the case of a man with pancreatic extracutaneous lymphoproliferative disease. adenocarcinoma who developed an CT scan incidentally detected a mass in the ichthyosiform eruption upon starting body of the pancreas and biopsy was chemotherapy with nab-paclitaxel plus concordant with pancreatic adenocarcinoma. -

Lymphatic Complaints in the Dermatology Clinic: an Osteopathic
Volume 35 JAOCDJournal Of The American Osteopathic College Of Dermatology Lymphatic Complaints in the Dermatology Clinic: An Osteopathic Approach to Management A five-minute treatment module makes lymphatic OMT a practical option in busy practices. Also in this issue: A Case of Acquired Port-Wine Stain (Fegeler Syndrome) Non-Pharmacologic Interventions in the Prevention of Pediatric Atopic Dermatitis: What the Evidence Says Inflammatory Linear Verrucous Epidermal Nevus Worsening in Pregnancy last modified on June 9, 2016 10:54 AM JOURNAL OF THE AMERICAN OSTEOPATHIC COLLEGE OF DERMATOLOGY Page 1 JOURNAL OF THE AMERICAN OSTEOPATHIC COLLEGE OF DERMATOLOGY 2015-2016 AOCD OFFICERS PRESIDENT Alpesh Desai, DO, FAOCD PRESIDENT-ELECT Karthik Krishnamurthy, DO, FAOCD FIRST VICE-PRESIDENT Daniel Ladd, DO, FAOCD SECOND VICE-PRESIDENT John P. Minni, DO, FAOCD Editor-in-Chief THIRD VICE-PRESIDENT Reagan Anderson, DO, FAOCD Karthik Krishnamurthy, DO SECRETARY-TREASURER Steven Grekin, DO, FAOCD Assistant Editor TRUSTEES Julia Layton, MFA Danica Alexander, DO, FAOCD (2015-2018) Michael Whitworth, DO, FAOCD (2013-2016) Tracy Favreau, DO, FAOCD (2013-2016) David Cleaver, DO, FAOCD (2014-2017) Amy Spizuoco, DO, FAOCD (2014-2017) Peter Saitta, DO, FAOCD (2015-2018) Immediate Past-President Rick Lin, DO, FAOCD EEC Representatives James Bernard, DO, FAOCD Michael Scott, DO, FAOCD Finance Committee Representative Donald Tillman, DO, FAOCD AOBD Representative Michael J. Scott, DO, FAOCD Executive Director Marsha A. Wise, BS AOCD • 2902 N. Baltimore St. • Kirksville, MO 63501 800-449-2623 • FAX: 660-627-2623 • www.aocd.org COPYRIGHT AND PERMISSION: Written permission must be obtained from the Journal of the American Osteopathic College of Dermatology for copying or reprinting text of more than half a page, tables or figures. -

Cytoplasmic Plaque Formation in Hemidesmosome Development Is Dependent on Soxf Transcription Factor Function
Cytoplasmic Plaque Formation in Hemidesmosome Development Is Dependent on SoxF Transcription Factor Function Shelly Oommen1, Mathias Francois2, Maiko Kawasaki1, Melanie Murrell2, Katsushige Kawasaki1, Thantrira Porntaveetus1, Sarah Ghafoor1, Neville J. Young2, Yoshimasa Okamatsu3, John McGrath4, Peter Koopman2, Paul T. Sharpe1, Atsushi Ohazama1,3* 1 Craniofacial Development and Stem Cell Biology, and Biomedical Research Centre, Dental Institute, King’s College London, London, United Kingdom, 2 Institute for Molecular Bioscience, The University of Queensland, Brisbane, Australia, 3 Department of Periodontology, Showa University Dental School, Tokyo, Japan, 4 Genetic Skin Disease Group, St John’s Institute of Dermatology, Division of Skin Sciences, King’s College London, London, United Kingdom Abstract Hemidesmosomes are composed of intricate networks of proteins, that are an essential attachment apparatus for the integrity of epithelial tissue. Disruption leads to blistering diseases such as epidermolysis bullosa. Members of the Sox gene family show dynamic and diverse expression patterns during development and mutation analyses in humans and mice provide evidence that they play a remarkable variety of roles in development and human disease. Previous studies have established that the mouse mutant ragged-opossum (Raop) expresses a dominant-negative form of the SOX18 transcription factor that interferes with the function of wild type SOX18 and of the related SOXF-subgroup proteins SOX7 and 217. Here we show that skin and oral mucosa in homozygous Raop mice display extensive detachment of epithelium from the underlying mesenchymal tissue, caused by tearing of epithelial cells just above the plasma membrane due to hemidesmosome disruption. In addition, several hemidesmosome proteins expression were found to be dysregulated in the Raop mice. -

Oral Verruciform Xanthoma: Report of 13 New Cases and Review of the Literature
Med Oral Patol Oral Cir Bucal. 2018 Jul 1;23 (4):e429-35. Oral verruciform xanthoma Journal section: Oral Medicine and Pathology doi:10.4317/medoral.22342 Publication Types: Review http://dx.doi.org/doi:10.4317/medoral.22342 Oral verruciform xanthoma: Report of 13 new cases and review of the literature Paris Tamiolakis 1, Vasileios I. Theofilou 1, Konstantinos I. Tosios 2, Alexandra Sklavounou-Andrikopoulou 3 1 DDS, Postgraduate Student, Department of Oral Medicine and Oral Pathology, School of Dentistry, National and Kapodistrian University of Athens, Greece, 2 Thivon Str, 115 27 Athens, Greece 2 DDS, PhD, Assistant Professor, Department of Oral Medicine and Oral Pathology, School of Dentistry, National and Kapodis- trian University of Athens, Greece, 2 Thivon Str, 115 27 Athens, Greece 3 DDS, MSc, PhD, Professor, Head of Department of Oral Medicine and Oral Pathology, School of Dentistry, National and Ka- podistrian University of Athens, Greece, 2 Thivon Str, 115 27 Athens, Greece Correspondence: Department of Oral Medicine and Oral Pathology School of Dentistry National and Kapodistrian University of Athens Greece, 2 Thivon Str, 11527, Goudi, Athens, Greece [email protected] Tamiolakis P, Theofilou VI, Tosios KI, Sklavounou-Andrikopoulou A. Oral verruciform xanthoma: Report of 13 new cases and review of the literature. Med Oral Patol Oral Cir Bucal. 2018 Jul 1;23 (4):e429-35. http://www.medicinaoral.com/medoralfree01/v23i4/medoralv23i4p429.pdf Received: 05/01/2018 Accepted: 09/05/2018 Article Number: 22342 http://www.medicinaoral.com/ © Medicina Oral S. L. C.I.F. B 96689336 - pISSN 1698-4447 - eISSN: 1698-6946 eMail: [email protected] Indexed in: Science Citation Index Expanded Journal Citation Reports Index Medicus, MEDLINE, PubMed Scopus, Embase and Emcare Indice Médico Español Abstract Background: Oral verruciform xanthoma (OVX) is a rare lesion. -

Oral and Maxillo-Facial Manifestations of Systemic Diseases: an Overview
medicina Review Oral and Maxillo-Facial Manifestations of Systemic Diseases: An Overview Saverio Capodiferro *,† , Luisa Limongelli *,† and Gianfranco Favia Department of Interdisciplinary Medicine, University of Bari Aldo Moro, Piazza G. Cesare, 11, 70124 Bari, Italy; [email protected] * Correspondence: [email protected] (S.C.); [email protected] (L.L.) † These authors contributed equally to the paper. Abstract: Many systemic (infective, genetic, autoimmune, neoplastic) diseases may involve the oral cavity and, more generally, the soft and hard tissues of the head and neck as primary or secondary localization. Primary onset in the oral cavity of both pediatric and adult diseases usually represents a true challenge for clinicians; their precocious detection is often difficult and requires a wide knowledge but surely results in the early diagnosis and therapy onset with an overall better prognosis and clinical outcomes. In the current paper, as for the topic of the current Special Issue, the authors present an overview on the most frequent clinical manifestations at the oral and maxillo-facial district of systemic disease. Keywords: oral cavity; head and neck; systemic disease; oral signs of systemic diseases; early diagnosis; differential diagnosis Citation: Capodiferro, S.; Limongelli, 1. Introduction L.; Favia, G. Oral and Maxillo-Facial Oral and maxillo-facial manifestations of systemic diseases represent an extensive and Manifestations of Systemic Diseases: fascinating study, which is mainly based on the knowledge that many signs and symptoms An Overview. Medicina 2021, 57, 271. as numerous systemic disorders may first present as or may be identified by head and https://doi.org/10.3390/ neck tissue changes. -

Vulvar Verruciform Xanthoma Ten Cases Associated with Lichen Sclerosus, Lichen Planus, Or Other Conditions
OBSERVATION ONLINE FIRST Vulvar Verruciform Xanthoma Ten Cases Associated With Lichen Sclerosus, Lichen Planus, or Other Conditions Charlotte Fite, MD; Franc¸oise Plantier, MD; Nicolas Dupin, MD, PhD; Marie-Franc¸oise Avril, MD; Micheline Moyal-Barracco, MD Background: Verruciform xanthoma (VX) is a rare be- acanthosis without atypia, and elongated rete ridges. nign tumor that usually involves the oral cavity. Since Xanthomatous cells were aggregated in the papillary the first report of this tumor in 1971, only 9 cases have dermis. been reported on the vulva, and 3 of these were associ- ated with another vulvar condition. We describe the clini- Conclusions: Vulvar VX is a benign tumor with mis- copathologic features of 10 patients with vulvar VX and leading clinical features. All 10 cases were associated with focus on their associated conditions. a vulvar condition, mainly a lichen sclerosus. There- fore, VX might represent a reaction pattern induced by Observation: The mean age of the patients was 68 years different conditions, mainly characterized by damage to (range, 51-80 years). The VX lesions were asymptom- the dermoepidermal junction. When confronted with the atic, yellowish-orange verrucous plaques. The diagno- diagnosis of vulvar VX, clinicians may look for an asso- sis was clinically suspected in 2 cases; other suggested ciated vulvar condition. diagnoses were condyloma or squamous cell carci- noma. All of the patients had an associated vulvar con- dition: lichen sclerosus (6 patients), lichen planus (2 Arch Dermatol. 2011;147(9):1087-1092. patients), Paget disease, or radiodermatitis. Under mi- Published online May 16, 2011. croscopy, the VX lesions displayed parakeratosis, doi:10.1001/archdermatol.2011.113 ERRUCIFORM XANTHOMA location, histologic findings, history of dyslip- (VX) is a rare benign tu- idemia, treatment, follow-up, and associated mor which was first vulvar conditions. -

Oral Pathology Final Exam Review Table Tuanh Le & Enoch Ng, DDS
Oral Pathology Final Exam Review Table TuAnh Le & Enoch Ng, DDS 2014 Bump under tongue: cementoblastoma (50% 1st molar) Ranula (remove lesion and feeding gland) dermoid cyst (neoplasm from 3 germ layers) (surgical removal) cystic teratoma, cyst of blandin nuhn (surgical removal down to muscle, recurrence likely) Multilocular radiolucency: mucoepidermoid carcinoma cherubism ameloblastoma Bump anterior of palate: KOT minor salivary gland tumor odontogenic myxoma nasopalatine duct cyst (surgical removal, rare recurrence) torus palatinus Mixed radiolucencies: 4 P’s (excise for biopsy; curette vigorously!) calcifying odontogenic (Gorlin) cyst o Pyogenic granuloma (vascular; granulation tissue) periapical cemento-osseous dysplasia (nothing) o Peripheral giant cell granuloma (purple-blue lesions) florid cemento-osseous dysplasia (nothing) o Peripheral ossifying fibroma (bone, cartilage/ ossifying material) focal cemento-osseous dysplasia (biopsy then do nothing) o Peripheral fibroma (fibrous ct) Kertocystic Odontogenic Tumor (KOT): unique histology of cyst lining! (see histo notes below); 3 important things: (1) high Multiple bumps on skin: recurrence rate (2) highly aggressive (3) related to Gorlin syndrome Nevoid basal cell carcinoma (Gorlin syndrome) Hyperparathyroidism: excess PTH found via lab test Neurofibromatosis (see notes below) (refer to derm MD, tell family members) mucoepidermoid carcinoma (mixture of mucus-producing and squamous epidermoid cells; most common minor salivary Nevus gland tumor) (get it out!) -

Diagnostic Discussion
Diagnostic Discussion Diagnostic Discussion By Drs. Indraneel Bhattacharyya and Nadim Islam A 44-year-old female was referred to Dr. Daniel Lauer, a periodontist in Palm Beach Gardens, Fla., for evaluation of a mildly symptomatic lesion on the palate (Fig. 1) by her dentist, Dr. Jimmy Chen, also of Palm Beach Gardens. The patient reported a his- tory of food-related trauma to her palate four to six weeks before the lesion appeared. She complained of mild irritation in the area, especially on food con- sumption. Her medical history was non-contributory and she reports no prior history of similar lesions. Fig. 1 She is a non-smoker. The lesion appeared slightly “bumpy” on the surface and was slightly reddish- to flesh-colored. It measured approximately 1 x 0.4 cm and was roughly rectangular in shape. Slight ery- thema was noted around the lesion. The lesion was entirely excised and submitted to the University of Florida College of Dentistry Oral Pathology Biopsy Service. The biopsy showed a papillary proliferation of epithelium with significantly thickened keratin with elongated rete ridges and foamy cells in the connec- tive tissue (Fig. 2). Question: Which of the following is the most likely diagnosis? A. Verrucous Leukoplakia B. Verruca Vulgaris C. Condyloma Acuminatum (venereal wart) D. Focal Epithelial Hyperplasia (Heck’s Disease) E. Verruciform Xanthoma Fig. 2 Please see DIAGNOSTIC, 50 www.floridadental.org May/June 2014 Today's FDA 49 Diagnostic Discussion DIAGNOSTIC from 49 ated with the human papilloma virus are mostly reported on the lingual fre- (HPV). Verruca vulgaris is associated num, soft palate and the labial mucosa, Diagnostic with HPV, HPV-2, HPV-4 and HPV- supposedly related to sites of abrasion 40. -

April 2011 Preventiongenetics Newsletter
News from PreventionGenetics IN THIS ISSUE Volume 3, Number 1 New Tests Welcome to the April 2011 PreventionGenetics Newsletter. In New Hires this issue, we present new DNA sequencing tests for 40 President's Corner disorders. In addition, we introduce two new geneticists to our staff. In the President's Corner, Dr. Jim Weber discusses recent progress at PreventionGenetics. QUICK LINKS Our Website Requisition Form New Tests at PreventionGenetics Please follow the gene links for the corresponding test description. · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · Achondrogenesis (SLC26A2) Achondrogenesis Type II-Hypochondrogenesis (COL2A1) Amyotrophic Lateral Sclerosis and Primary Open-Angle Glaucoma (OPTN) Atelosteogenesis (SLC26A2) Camurati-Engelmann Disease (TGFB1) Cartilage-hair Hypoplasia and Related Disorders (RMRP) Chediak-Higashi Syndrome (LYST) Chondrodysplasia Punctata, X-Linked Dominant (EBP) Cleidocranial Dysplasia (RUNX2) Cranioectodermal Dysplasia 1 (IFT122) Diastrophic Dysplasia (SLC26A2) Dilated Cardiomyopathy and Limb-Girdle Muscular Dystrophy Type 2F (SGCD) Dentinogenesis Imperfecta (DSPP) Ellis-van Creveld Syndrome (EVC, EVC2) Emery-Dreifuss Muscular Dystrophy-1 (EMD) Fanconi Anemia (FANCL) Hennekam Lymphangiectasia-Lymphedema (CCBE1) Hereditary Breast Cancer (CHEK2) Hermansky Pudlak Syndrome (HPS1, HPS2/AP3B1, HPS3, HPS4, HPS5, HPS6, HPS7/DTNBP1, HPS8/BLOC1S3) Hirschsprung Disease (RET) Holt-Oram Syndrome (TBX5) Kneist Dysplasia (COL2A1) Lynch Syndrome (PMS2) Menkes Disease and X-Hereditary -
Hand and Arm Guidelines After Your Axillary Lymph Node Dissection
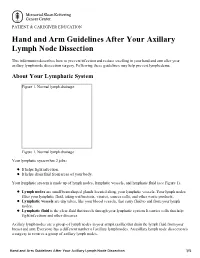
PATIENT & CAREGIVER EDUCATION Hand and Arm Guidelines After Your Axillary Lymph Node Dissection This information describes how to prevent infection and reduce swelling in your hand and arm after your axillary lymph node dissection surgery. Following these guidelines may help prevent lymphedema. About Your Lymphatic System Figure 1. Normal lymph drainage Figure 1. Normal lymph drainage Your lymphatic system has 2 jobs: It helps fight infection. It helps drain fluid from areas of your body. Your lymphatic system is made up of lymph nodes, lymphatic vessels, and lymphatic fluid (see Figure 1). Lymph nodes are small bean-shaped glands located along your lymphatic vessels. Your lymph nodes filter your lymphatic fluid, taking out bacteria, viruses, cancer cells, and other waste products. Lymphatic vessels are tiny tubes, like your blood vessels, that carry fluid to and from your lymph nodes. Lymphatic fluid is the clear fluid that travels through your lymphatic system. It carries cells that help fight infections and other diseases. Axillary lymph nodes are a group of lymph nodes in your armpit (axilla) that drain the lymph fluid from your breast and arm. Everyone has a different number of axillary lymph nodes. An axillary lymph node dissection is a surgery to remove a group of axillary lymph nodes. Hand and Arm Guidelines After Your Axillary Lymph Node Dissection 1/5 About Lymphedema Sometimes, removing lymph nodes can make it hard for your lymphatic system to drain properly. If this happens, lymphatic fluid can build up in the area where the lymph nodes were removed. This extra fluid causes swelling called lymphedema.