A Comilation of Anabolics and Nutritional Supplements
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Comparison of the Effects of High Dose Testosterone and 19-Nortestosterone to a Replacement Dose of Testosterone on Strength and Body Composition in Normal Men
J. Steroid Biochem. Molec. Biol. Vol. 40, No. 4-6, pp. 607~12, 1991 0960-0760/91 $3.00 + 0.00 Printed in Great Britain Pergamon Press plc COMPARISON OF THE EFFECTS OF HIGH DOSE TESTOSTERONE AND 19-NORTESTOSTERONE TO A REPLACEMENT DOSE OF TESTOSTERONE ON STRENGTH AND BODY COMPOSITION IN NORMAL MEN KARL E. FRIEDL,* JOSEPH R. DETTORI, CHARLES J. HANNAN JR, TROY H. PATIENCE and STEPHENR. PLYMATE Exercise Physiology Division, U.S. Army Research Institute of Environmental Medicine, Natick, MA and Department of Clinical Investigation, Madigan Army Medical Center, Tacoma, WA, U.S.A. Summary--We examined the extent to which supraphysiological doses of androgen can modify body composition and strength in normally virilized men. In doubly blind tests, 30 healthy young men received testosterone enanthate (TE) or 19-nortestosterone decanoate (ND), at 100mg/wk or 300mg/wk for 6 weeks. The TE-100mg/wk group served as replacement dose comparison, maintaining pretreatment serum testosterone levels, while keeping all subjects blinded to treatment, particularly through reduction in testicular volumes. Isokinetic strength measurements were made for the biceps brachii and quadriceps femoris muscle groups before treatment and 2-3 days after the 6th injection. Small improvements were noted in all groups but the changes were highly variable; a trend to greater and more consistent strength gain occurred in the TE-300mg/wk group. There was no change in weight for TE-100 mg/wk but an average gain of 3 kg in each of the other groups. No changes in 4 skinfold thicknesses or in estimated percent body fat were observed. -

Ranvet's Filybol
Ranvet's Filybol Ranvet Chemwatch Hazard Alert Code: 2 Chemwatch: 4787-83 Issue Date: 08/02/2016 Version No: 5.1.1.1 Print Date: 10/28/2016 Safety Data Sheet according to WHS and ADG requirements S.GHS.AUS.EN SECTION 1 IDENTIFICATION OF THE SUBSTANCE / MIXTURE AND OF THE COMPANY / UNDERTAKING Product Identifier Product name Ranvet's Filybol Chemical Name peanut oil Synonyms Not Available Other means of Not Available identification Relevant identified uses of the substance or mixture and uses advised against Relevant identified Non-virilising anabolic combination for fillies, mares, colts and stallions. uses Details of the supplier of the safety data sheet Registered company Ranvet name Address 10-12 Green Street Banksmeadow NSW 2019 Australia Telephone +61 2 9666 1744 Fax +61 2 9666 1755 Website https://www.ranvet.com.au/other_msds.htm Email [email protected] Emergency telephone number Association / Not Available Organisation Emergency telephone +61 425 061 584 numbers Other emergency Not Available telephone numbers SECTION 2 HAZARDS IDENTIFICATION Classification of the substance or mixture Poisons Schedule S4 Carcinogenicity Category 2, Reproductive Toxicity Category 2, Acute Aquatic Hazard Category 2, Chronic Aquatic Hazard Classification [1] Category 2 1. Classified by Chemwatch; 2. Classification drawn from HSIS ; 3. Classification drawn from EC Directive 1272/2008 - Annex Legend: VI Label elements GHS label elements SIGNAL WORD WARNING Continued... Chemwatch: 4787-83 Page 2 of 10 Issue Date: 08/02/2016 Version No: 5.1.1.1 Ranvet's Filybol Print Date: 10/28/2016 Hazard statement(s) H351 Suspected of causing cancer. H361 Suspected of damaging fertility or the unborn child. -

TESTOSTERONE and ANABOLIC STEROIDS Summary Testosterone Is a Hormone Naturally Produced by the Body
FactSHEET TESTOSTERONE AND ANABOLIC STEROIDS Summary Testosterone is a hormone naturally produced by the body. Low levels of testosterone can cause symptoms of fatigue, malaise, loss of sex drive, and loss of muscle tissue. These symptoms can often be treated with synthetic testosterone. Anabolic steroids are compounds related to testosterone. Using synthetic testosterone or anabolic steroids may help people with HIV-related wasting gain weight, especially muscle mass. What is testosterone? Sometimes HIV-positive men develop low testosterone levels which can cause symptoms Although it is usually thought of as a male of fatigue, muscle wasting, low (or no) sex hormone, women’s bodies also make drive, impotence, and loss of facial or body testosterone, but at much lower levels than hair. This condition is called hypogonadism. men’s. Testosterone has two different effects on Hormone replacement therapy with synthetic the body: anabolic effects which promote growth testosterone may help to relieve those and muscle building, and androgenic effects symptoms. which develop the male sex organs and secondary sex characteristics such as deepening HIV-positive women may also develop low of the voice and growth of facial hair. testosterone levels and experience symptoms of fatigue, loss of sex drive, and a decreased sense of well-being. Because the androgenic What are anabolic steroids? (masculinizing) effects of testosterone and Anabolic steroids are synthetic compounds anabolic steroids can be permanent, that resemble the natural hormone researchers have been cautious about studying testosterone. Makers of anabolic steroids these drugs in women. change the testosterone molecule slightly to 2. To treat weight loss change the balance of androgenic and anabolic effects, which can allow these drugs to build Anabolic steroids can be used in order to build muscle with fewer masculinizing effects. -

Anabolic Androgenic Steroid Use Prevalence, Knowledge, and Practice Among Male Athletes in Eastern Province of Saudi Arabia
Electronic Journal of General Medicine 2020, 17(2), em187 e-ISSN: 2516-3507 https://www.ejgm.co.uk/ Original Article OPEN ACCESS Anabolic Androgenic Steroid Use Prevalence, Knowledge, and Practice among Male Athletes in Eastern Province of Saudi Arabia Huda Hassan Aldarweesh 1, Alyaa Hassan Alhajjaj 1* 1 Qatif Central Hospital, SAUDI ARABIA *Corresponding Author: [email protected] Citation: Aldarweesh HH, AlHajjaj AH. Anabolic Androgenic Steroid Use Prevalence, Knowledge, and Practice among Male Athletes in Eastern Province of Saudi Arabia. Electron J Gen Med. 2020;17(2):em187. https://doi.org/10.29333/ejgm/7617 ARTICLE INFO ABSTRACT Received: 25 Oct. 2019 Background: Anabolic androgenic steroids (AAS) are synthetic testosterone like hormones. AAS usage by athletes Accepted: 30 Dec. 2019 has increased dramatically over the past decade. Material and Methods: This study was designed to examine the prevalence, attitude and awareness of AAS abuse among athletes n the Eastern province of Saud Arabia. This was a cross-sectional survey that was conducted among male athletes attending twenty fitness centres in the Eastern Province. It was done during the period from April to August, 2018. Results: A total of 573 questionnaires were distributed but only 503 participants were included n the final analysis. The frequency of AAS use was 17.69%. The man reason for AAS use was muscle building (68.54%). The man source of AAS was the coaches. 56.18% of the users recognize the harmful effects of AAS. The most commonly used oral AAS form was oxandrolone (61.80%). The most commonly used substance for post cycle therapy was Tamoxifen citrate n 67.42% of the users. -

Testosterone, Injectable
Clinical Criteria Subject: Testosterone, Injectable Document #: ING-CC-0026 Publish Date: 06/10/201909/23/2019 Status: ReviewedRevised Last Review Date: 03/18/201908/16/2019 Table of Contents Overview Coding References Clinical criteria Document history Overview This document addresses indications for the intramuscular (IM) and subcutaneous (SC) administration of testosterone injectables for the treatment of hormone deficient conditions. The following testosterone injection agents are included: • Testosterone cypionate intramuscular: Depo-Testosterone, generic testosterone cypionate • Testosterone enanthate: o Intramuscular: generic testosterone enanthate o Subcutaneous: Xyosted (auto-injector) • Testosterone undecanoate intramuscular: Aveed Testosterone is an androgen hormone responsible for normal growth and development of male sex characteristics. In certain medical conditions such as hypogonadism, the endogenous level of testosterone falls below normal levels. Primary hypogonadism includes conditions such as testicular failure due to cryptorchidism, bilateral torsion, orchitis, or vanishing testis syndrome; bilateral orchidectomy; and inborn errors in the biosynthesis of testosterone. Secondary hypogonadism, also called hypogonadotropic hypogonadism includes conditions such as gonadotropin-releasing hormone (GnRH) deficiency or pituitary-hypothalamic injury resulting from tumors, trauma, surgery, or radiation. In 2015, the Endocrine Society added the following amended recommendations: • Men with metabolic syndrome, who were previously unexamined by the 2010 Endocrine Society Clinical Practice Guidelines, may benefit from testosterone replacement therapy (TRT) based on improvements in biometrics and insulin sensitivity. Effects of TRT on similar endpoints in men with type 2 diabetes mellitus remain unclear; • Effects of TRT on erectile function, even in men refractory to phosphodiesterase type 5 inhibitors, and on quality of life in men with erectile dysfunction remain inconclusive (Seftel, 2015). -

New Zealand Data Sheet 1. Product Name
NEW ZEALAND DATA SHEET 1. PRODUCT NAME SUSTANON 250 (250 mg testosterone esters solution for injection) (SUSTANON) TESTOSTERONE ESTERS 250mg/mL for injection Presentations that are not currently available The vials are currently not available 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Name and strength of the active substances - testosterone proprionate 30mg testosterone phenylpropionate 60mg testosterone isocaproate 60mg testosterone decanoate 100mg All four compounds are esters of the natural hormone testosterone. The total amount of testosterone per 1 mL is 176mg. List of excipients - 1 mL arachis oil and the solution also contains 10 per cent benzyl alcohol. For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Oily solution for intramuscular use. A clear, pale yellow solution. Each clear glass ampoule or vial contains 1 mL in arachis oil. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Testosterone replacement therapy in males for conditions associated with primary and secondary hypogonadism, either congenital or acquired. In female to male transsexuals: • masculinization Moreover, in men testosterone therapy may be indicated in osteoporosis caused by androgen deficiency. 4.2 Dose and method of administration In general, the dose should be adjusted according to the response of the individual patient. Dose Adults (incl. elderly): Usually, one injection of 1ml per three weeks is adequate. Paediatric population: Safety and efficacy in children and adolescents, have not yet been established. Pre-pubertal children treated with SUSTANON should be treated with caution (see Warnings and Precautions). SUSTANON contains benzyl alcohol and is contraindicatedin children under 3 years of age. Method of administration SUSTANON should be administered by deep intramuscular injection. -

MMC International BV
M.M.C. International Steroid Substances Steroid Test A Colour Steroid Test B Colour Steroid Test B Colour with UV Light Stanozolol/ Oxandrolone Test Clenbuterol/ Oxymetholone Test Ephedrine Test Alfadolone Orange Yellow Nil - - - Androsterone Orange Yellow White - - - Beclometasone Brown–yellow Orange Nil - - - Betamethasone Orange–brown Pink–Orange Nil - - - Boldenone Base (Equipoise, Ganabol) (pure powder) Warm red after 2 min. Dark Orange after 2 min. Bright Light Orange - - - Boldenone Undecanoate (oil) Dark brownish-red Dark Red Bright Light Orange - - - Boldenone Undecylenate (oil) Orange - Light Brown Dark Orange → Brown Bright Light Orange-Yellow - - - Carbenoxolone (CBX) Orange Yellow Yellow - - - Cholesterol Violet Orange White - - - Clenbuterol (Spiropent, Ventipulmin) - - - - Purple - Dark brown with yellow-green on the Dark brown with yellow-green on the Clomiphene (Androxal, Clomid, Omifin) Nil Dark brown to black No reaction Dark brown to black sides of the ampoule sides of the ampoule Cortisone Orange Yellow Green - - - Desoxycortone Blue–black Yellow Yellow - - - Dexamethasone Yellow Orange–pink Nil - - - Dienestrol Yellow Orange–red Nil - - - Diethylstilbestrol (DES) Orange (→yellow–green) Nil - - - Dimethisterone Brown–green Orange–red Yellow - - - Drostanolone Propionate (Masteron) (oil) Bright green Yellow-Orange Orange - - - Dydrogesterone (Duphaston) - Orange Green-Yellow - - - Enoxolone Orange Yellow Green-Yellow - - - Ephedrine (also for Pseudo- and Nor-Ephedrine) - - - - - Orange Estradiol (Oestradiol) Orange -

Chemical Muscle Enhancement (The BDR) by Author L
Chemical Muscle Enhancement (The BDR) By Author L. Rea TABLE OF CONTENTS 1. AAS INTRODUCTION ..PG’S 1-12 WARNING: READ FIRST OVER 20 YEARS AGO... WHY STEROIDS AND WHAT IS POSSIBLE? WHAT ARE STEROIDS? FEMALE HORMONE SYNTHESIS MALE HORMONE SYNTHESIS TESTOSTERONE... WHAT DOES IT DO? STEROIDS INCREASE PC SYNTHESIS STEROIDS EFFECT BLOOD VOLUME WHAT HAPPENS AFTER TESTOSTERONE MOLECULES LEAVE RECEPTORS? STEROIDS...GROWTH ON THE CELULAR LEVEL 2. DRUG REFERENCES AND DESCRIPTIONS..PG 12 ORAL ANABOLIC / ANDROGENIC STEROIDS..PG’S 13-30 INJECTABLE ANABOLIC / ANDROGENIC STEROIDS..PG’S 31-45 TESTOSTERONE AND ITS ESTERS..PG’S 45-61 NORTESTOSTERONE (NANDROLONE) AND ITS ESTER..PG’S 62-70 TRENBOLONE AND DERIVATIVES..PG’S 71-78 ESTROGEN CONTROL AND HPTA REGENERATION DRUGS..PG’S 79-94 DIURETICS..PG’S 95-102 THYROID HORMONES ..PG’S 103-116 NON-AAS GROWTH FACTORS AND RELATED SUBSTANCES..PG’S 117-141 OTHER SUBSTANCES..PG’S 142-152 3. REPORTED CYCLES AND EFFECTS.. (Introduction) PG’S 153-159 REPORTED CYCLES AND EFFECTS EXAMPLES (MALE)...PG’S 160-169 REPORTED CYCLES AND EFFECTS EXAMPLES (FEMALE)...PG’S 170-174 REPORTED ADVANCED CYCLES AND EFFECTS-BLITZ CYCLES..PG’S 175-200 (More Reported Cycles and Effects) 4. NUTRITION..PG’S..201-211 5. SUPPLEMENTAL CREATINE..PG’S 212-216 6. REFERENCES AND AVAILABLE LITERATURE..PG’S 217-223 All Rights Reserved CHEMICAL MUSCLE ENHANCEMENT (The Report) and BODYBUILDERS DESK REFERENCE COPYRIGHT ©2002 by AUTHOR L. REA No part of this book may be reproduced or transmitted in any form or by any means, electronic or mechanical including photocopy, recording, or by any information storage and retrieval system, without the permission in writing of the author and publisher. -

M.M.C. International
M.M.C. International Clenbuterol/ Oxymetholone Steroid Substances Steroid Test A Colour Steroid Test B Colour Steroid Test B Colour with UV Light Stanozolol/ Oxandrolone Test Ephedrine Test Test Alfadolone Orange Yellow Nil - - - Androsterone Orange Yellow White - - - Beclometasone Brown–yellow Orange Nil - - - Betamethasone Orange–brown Pink–Orange Nil - - - Boldenone Base (Equipoise, Ganabol) (pure powder) Warm red after 2 min. Dark Orange after 2 min. Bright Light Orange - - - Boldenone Undecanoate (oil) Dark brownish-red Dark Red Bright Light Orange - - - Boldenone Undecylenate (oil) Orange - Light Brown Dark Orange → Brown Bright Light Orange-Yellow - - - Carbenoxolone (CBX) Orange Yellow Yellow - - - Cholesterol Violet Orange White - - - Clenbuterol (Spiropent, Ventipulmin) - - - - Purple - Dark brown with yellow-green on Dark brown with yellow-green on the Clomiphene (Androxal, Clomid, Omifin) Nil Dark brown to black No reaction Dark brown to black the sides of the ampoule sides of the ampoule Cortisone Orange Yellow Green - - - Desoxycortone Blue–black Yellow Yellow - - - Dexamethasone Yellow Orange–pink Nil - - - Dienestrol Yellow Orange–red Nil - - - Diethylstilbestrol (DES) Orange (→yellow–green) Nil - - - Dimethisterone Brown–green Orange–red Yellow - - - Drostanolone Propionate (Masteron) (oil) Bright green Yellow-Orange Orange - - - Dydrogesterone (Duphaston) - Orange Green-Yellow - - - Enoxolone Orange Yellow Green-Yellow - - - Ephedrine (also for Pseudo- and Nor-Ephedrine) - - - - - Orange Estradiol (Oestradiol) Orange -
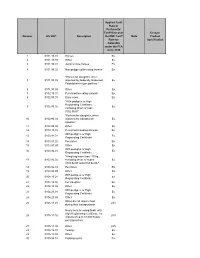
Number HS 2007 Description Applied Tariff Rate Or Preferential Tariff Rate
Applied Tariff Rate or Preferential Tariff Rate over Ex-out / Number HS 2007 Description the NMF Tariff Note Product Rate for Specification Colombia under the FTA since 2010 1 0101.10.01 Horses Ex. 2 0101.10.99 Other Ex. 3 0101.90.01 Jump or race horses Ex. 4 0101.90.02 Non pedigreed breeding horses Ex. "Horses for slaughter, when 5 0101.90.03 imported by Federally Inspected Ex. Establishment type packers." 6 0101.90.99 Other Ex. 7 0102.10.01 Pure-bred breeding animals Ex. 8 0102.90.01 Dairy cows Ex. "With pedigree or High Registrating Certificate, 9 0102.90.02 Ex. excluding those of code 0102.90.01" "Bovines for slaughter, when 10 0102.90.03 imported by Industrial de Ex. Abastos." 11 0102.90.99 Other Ex. 12 0103.10.01 Pure-bred breeding animals Ex. With pedigree or High 13 0103.91.01 Ex. Registrating Certificate. 14 0103.91.02 Peccaries Ex. 15 0103.91.99 Other Ex. With pedigree or High 16 0103.92.01 Ex. Registrating Certificate. "Weighing more than 110 kg., 17 0103.92.02 excluding those of codes Ex. 0103.92.01 and 0103.92.03." 18 0103.92.03 Peccaries Ex. 19 0103.92.99 Other Ex. With pedigree or High 20 0104.10.01 Ex. Registrating Certificate. 21 0104.10.02 For slaughter. Ex. 22 0104.10.99 Other Ex. With pedigree or High 23 0104.20.01 Ex. Registrating Certificate. 24 0104.20.99 Other Ex. When do not require food 25 0105.11.01 28% during their transportation Newly born breeding birds, with High Registrating Certificate, for 26 0105.11.02 28% imports of up to 18,000 heads per transaction. -

A28 Anabolic Steroids
Anabolic SteroidsSteroids A guide for users & professionals his booklet is designed to provide information about the use of anabolic steroids and some of the other drugs Tthat are used in conjunction with them. We have tried to keep the booklet free from technical jargon but on occasions it has proven necessary to include some medical, chemical or biological terminology. I hope that this will not prevent the information being accessible to all readers. The first section explaining how steroids work is the most complex, but it gets easier to understand after that (promise). The booklet is not intended to encourage anyone to use these drugs but provides basic information about how they work, how they are used and the possible consequences of using them. Anabolic Steroids A guide for users & professionals Contents Introduction .........................................................7 Formation of Testosterone ...............................................................8 Method of Action ..............................................................................9 How Steroids Work (illustration).......................................................10 Section 1 How Steroids are Used ....................................... 13 What Steroid? ................................................................................ 14 How Much to Use? ......................................................................... 15 Length of Courses? ........................................................................ 15 How Often to Use Steroids? -

Pdf 86.39 Kb
“Detection of Testosterone Esters in Blood Sample” Dr. G. Gmeiner, Dr. G. Forsdahl, Dr. Erceg (Seibersdorf Labor GmbH, Austria) Project Summary Testosterone is still regarded as the major contributor to steroid doping world-wide. Among the most common forms of application are injections of different sorts of esters. State-of-the-Art detection of Testosterone doping includes the quantification of the Testosterone /Epitestosterone – Ratio (T/E – ratio) as well as subsequent Isotope ratio mass spectrometry (IRMS). Previous published studies of our research group have demonstrated that a comparably high percentage of testosterone preparations do not significantly differ from endogenous values of testosterone and markers of testosterone doping. Consequently when such preparations with endogenous – like 13CVPDB values are applied, IRMS - technology fails to detect testosterone doping. Direct detection of the testosterone ester leads to an unequivocal proof of doping with testosterone preparations, because such esters are not built endogenously. Previous studies indicate that a direct detection of testosterone esters in both hair and plasma is possible. Aim of the proposed project is the investigation and optimisation of the direct detection of testosterone esters in body fluids like serum, whole blood and stabilized blood with an already developed detection method using modern and sensitive technology. The project will gain information on diagnostic windows for detection of doping using testosterone esters and proper sampling conditions. Additional aim of the proposed project is to evaluate the suitability of already collected blood samples in doping control (e.g. samples collected for blood parameter measurement or growth hormone detection) for a possible reanalysis for testosterone esters.