Radiology Fundamentals: Introduction to Imaging & Technology
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cardiothoracic Fellowship Program
Cardiothoracic Fellowship Program Table of Contents Program Contact ............................................................................................ 3 Other contact numbers .................................................................................. 4 Introduction ........................................................................................................... 5 Goals and Objectives of Fellowship: ..................................................................... 6 Rotation Schedule: ........................................................................................ 7 Core Curriculum .................................................................................................... 8 Fellow’s Responsibilities ..................................................................................... 22 Resources ........................................................................................................... 23 Facilities ....................................................................................................... 23 Educational Program .......................................................................................... 26 Duty Hours .......................................................................................................... 29 Evaluation ........................................................................................................... 30 Table of Appendices .................................................................................... 31 Appendix A -
High Yield Points
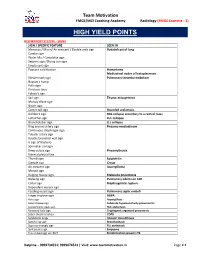
Team Motivation FMGE/MCI Coaching Academy Radiology (FMGE Essentia - 3) HIGH YIELD POINTS RESPIRATORY SYSTEM – SIGNS SIGN / SPECIFIC FEATURE SEEN IN Meniscus / Moon/ Air crescent / Double arch sign Hydatid cyst of lung Cumbo sign Water lilly / Camalotte sign Serpent sign / Rising sun sign Empty cyst sign Popcorn calcification Hamartoma Mediastinal nodes of histoplasmosis Westermark sign Pulmonary thrombo-embolism Hapton’s hump Palla sign Fleishner lines Felson’s sign Sail sign Thymic enlargement Mulvay Wave sign Notch sign Comet tail sign Rounded atelectasis Golden S sign RUL collapse secondary to a central mass Luftsichel sign LUL collapse Broncholobar sign LLL collapse Ring around artery sign Pneumo-mediastinum Continuous diaphragm sign Tubular artery sign Double bronchial wall sign V sign of Naclerio Spinnaker sail sign Deep sulcus sign Pneumothorax Visceral pleural line Thumb sign Epiglottitis Steeple sign Croup Air crescent sign Aspergilloma Monod sign Bulging fissure sign Klebsiella pneumonia Batwing sign Pulmonary edema on CXR Collar sign Diaphragmatic rupture Dependant viscera sign Feeding vessel sign Pulmonary septic emboli Finger in glove sign ABPA Halo sign Aspergillosis Head cheese sign Subacute hypersensitivity pneumonitis Juxtaphrenic peak sign RUL atelectasis Reversed halo sign Cryptogenic organized pneumonia Saber sheath trachea COPD Sandstorm lungs Alveolar microlithiasis Signet ring sign Bronchiectasis Superior triangle sign RLL atelectasis Split pleura sign Empyema Tree in bud sign on HRCT Endobronchial spread in TB -

1 Department of Radiology Residency Program Manual
DEPARTMENT OF RADIOLOGY RESIDENCY PROGRAM MANUAL 1 TABLE OF CONTENTS Table of Contents WELCOME....................................................................................................................................2 GOALS AND OBJECTIVES.................................................................................................. 3-98 DAILY RESPONSIBILITIES....................................................................................................99 CALL RESPONSIBILITIES....................................................................................................101 TRAVEL GUIDELINES...........................................................................................................105 BOOK ALLOWANCE..............................................................................................................107 FINGERPRITING REIMBURSEMENT................................................................................107 HOLIDAY COMP DAY............................................................................................................107 EVALUATIONS ........................................................................................................................108 WELCOME The faculty and staff here at the Department of Radiology, New Jersey Medical School welcome all of you as you embark on this important facet of your training. We are the longest running academic training program in New Jersey, and have trained over 120 residents in the past 30 years. Our trainees have excelled in their -

100 CASES in Radiology This Page Intentionally Left Blank 100 CASES in Radiology
100 CASES in Radiology This page intentionally left blank 100 CASES in Radiology Robert Thomas Specialist Registrar, Guy’s and St Thomas’ Hospital, London, UK James Connelly Specialist Registrar, Guy’s and St Thomas’ Hospital, London, UK Christopher Burke Specialist Registrar, Guy’s and St Thomas’ Hospital, London, UK 100 Cases Series Editor: Professor P John Rees MD FRCP Dean of Medical Undergraduate Education, King’s College London School of Medicine at Guy’s, King’s and St Thomas’ Hospitals, London, UK First published in Great Britain in 2012 by Hodder Arnold, an imprint of Hodder Education, Hodder and Stoughton Ltd, a division of Hachette UK 338 Euston Road, London NW1 3BH http://www.hodderarnold.com © 2012 Robert Thomas, James Connelly and Christopher Burke All rights reserved. Apart from any use permitted under UK copyright law, this publication may only be reproduced, stored or transmitted, in any form, or by any means with prior permission in writing of the publishers or in the case of reprographic production in accordance with the terms of licences issued by the Copyright Licensing Agency. In the United Kingdom such licences are issued by the Copyright Licensing Agency: Saffron House, 6–10 Kirby Street, London EC1N 8TS. Hachette UK’s policy is to use papers that are natural, renewable and recyclable products and made from wood grown in sustainable forests. The logging and manufacturing processes are expected to conform to the environmental regulations of the country of origin. Whilst the advice and information in this book are believed to be true and accurate at the date of going to press, neither the author[s] nor the publisher can accept any legal responsibility or liability for any errors or omissions that may be made. -

Juerg Hodler Rahel A. Kubik-Huch Gustav K. Von Schulthess Editors Diagnostic and Interventional Imaging
IDKD Springer Series Series Editors: Juerg Hodler · Rahel A. Kubik-Huch · Gustav K. von Schulthess Juerg Hodler Rahel A. Kubik-Huch Gustav K. von Schulthess Editors Diseases of the Chest, Breast, Heart and Vessels 2019–2022 Diagnostic and Interventional Imaging IDKD Springer Series Series Editors Juerg Hodler Department of Radiology University Hospital of Zürich Zürich, Switzerland Rahel A. Kubik-Huch Department of Radiology Kantonsspital Baden Zürich, Switzerland Gustav K. von Schulthess Deptartment of Nuclear Medicine University Hospital of Zürich Zürich, Switzerland The world-renowned International Diagnostic Course in Davos (IDKD) represents a unique learning experience for imaging specialists in training as well as for experienced radiologists and clinicians. IDKD reinforces his role of educator offering to the scientific community tools of both basic knowledge and clinical practice. Aim of this Series, based on the faculty of the Davos Course and now launched as open access publication, is to provide a periodically renewed update on the current state of the art and the latest developments in the field of organ- based imaging (chest, neuro, MSK, and abdominal). More information about this series at http://www.springer.com/series/15856 Juerg Hodler • Rahel A. Kubik-Huch Gustav K. von Schulthess Editors Diseases of the Chest, Breast, Heart and Vessels 2019–2022 Diagnostic and Interventional Imaging Editors Juerg Hodler Rahel A. Kubik-Huch Department of Radiology Department of Radiology University Hospital of Zürich Kantonsspital Baden -

Rotation: VGH Chest Radiography VGH 899 West 12Th Ave., Vancouver, BC V5Z 1M9
Rotation: VGH Chest Radiography VGH 899 West 12th Ave., Vancouver, BC V5Z 1M9 Level: PGY 2‐5 Rotation Supervisor: Dr. Ana‐Maria Bilawich During the course of the four years, residents will receive one month of chest radiography training as a junior resident and one month of chest radiography training as a senior resident. Residents are expected to develop graded responsibility as they rise from junior to senior resident level. Each resident will be given guidance at the beginning of a rotation, an interim evaluation will occur mid rotation, and a final evaluation will be given at the end of each rotation. Each final evaluation will be submitted to the residency training program director. All residents are expected to arrive in the department by 0800 hours and stay until the conclusion of the working day. Ongoing teaching and interaction with the staff occurs throughout the day. If a resident is absent from his/her chest plain radiography rotation for any reason, he/she should give ample warning to Dr. Mayo (Chest Section Head) and Dr. Bilawich (rotation supervisor). Vacation and conference requests must be booked with Dr. Mayo and Dr. Bilawich in advance, at least two weeks prior to any planned absence from the rotation. Medical Expert: 1. Basic Science: a) Knowledge of anatomy (PA and lateral chest radiographs) At the end of first Chest radiography rotation, the junior resident (PGY2/3) will demonstrate learning all of the following anatomy on PA and lateral chest radiographs. At the end of the second Chest radiography rotation, the senior resident (PGY4/5) will demonstrate learning all of the following anatomy on PA and lateral chest radiographs. -
Chest-Mostly-Fixed-1
Chest 1997-2008 2008 Chest L-Transposition (Recall): A. AV disconcordance, Arteriovent concordance B. AV/Arterioventricular discordance C. Atrioventricular Discordance, Ventriculoarterial Discordance L-Transposition of Great Vessels. A. Artioventricular concordance Arterioventricular concordance B. Every other possible combination L-Transposition of Great Vessels. Artioventricular concordance Arterioventricular concordance ArtioventriculardisconcordanceArterioventriculardisconcordance Every other possible combination L transposition A. Arteriorventricular concordance and Atrioventricular discordance B. And multiple variations of this 2008 Chest L-Transposition (Recall): A. AV disconcordance, Arteriovent concordance B. AV/Arterioventricular discordance C. Atrioventricular Discordance, Ventriculoarterial Discordance L-Transposition of Great Vessels. A. Artioventricular concordance Arterioventricular concordance B. Atrioventricular Discordance, Ventriculoarterial Discordance C. Every other possible combination L-Transposition of Great Vessels. Artioventricular concordance Arterioventricular concordance ArtioventriculardisconcordanceArterioventriculardisconcordance Every other possible combination L transposition A. Arteriorventricular concordance and Atrioventricular discordance B. Atrioventricular Discordance, Ventriculoarterial Discordance C. And multiple variations of this Levo-Transposition of the Great Arteries Commonly referred to as congenitally corrected transposition of the great arteries (CC-TGA) -
Revised Curriculum on Cardiothoracic Radiology for Diagnostic Radiology Residency with Goals and Objectives Related to General Competencies1
Radiology Resident Education Revised Curriculum on Cardiothoracic Radiology for Diagnostic Radiology Residency With Goals and Objectives Related to General Competencies1 Prepared by the Education Committee of the Society of Thoracic Radiology: Jannette Collins, MD, MEd, FCCP, Gerald F. Abbott, MD, John M. Holbert, MD, FCCP, Brian F. Mullan, MD, FCCP, Ella A. Kazerooni, MD, Michael B. Gotway, MD, Michelle S. Ginsberg, MD, Joan M. Lacomis, MD, Shawn D. Teague, MD, Gautham P. Reddy, MD, John A. Worrell, MD, Andetta Hunsaker, MD This document is a revision of a previously published cardiothoracic curriculum for diagnostic radiology residency (1), and reflects interval changes in the clinical practice of cardiothoracic radiology and changes in the Accreditation Council for Graduate Medical Education (ACGME) requirements for diagnostic radiology training programs. The revised ACGME Program Requirements for Residency Education in Diagnostic Radiology (2) went into effect December 2003. © AUR, 2005 The residency program director is responsible for the tudes required and provide educational experiences as “preparation of a written statement outlining the educa- needed for their residents to demonstrate competence in tional goals of the program with respect to knowledge, the following six areas: patient care, medical knowledge, skills, and other attributes of residents for each major as- professionalism, interpersonal/communication skills, prac- signment and each level of the program” (2). Since the tice-based learning and improvement, and systems-based first cardiothoracic curriculum was published, the practice. These six areas, as they specifically relate to ACGME has added new language to the program require- radiology, have been defined previously (3). ments regarding six areas of competency. -

Radiology Fundamentals
Radiology Fundamentals Harjit Singh ● Janet A Neutze Editors Jonathan R Enterline ● Joseph S Fotos Associate Editors Jonathan J Douds ● Megan Jenkins Kalambo ● Marsha J Bluto Contributing Editors Radiology Fundamentals Introduction to Imaging & Technology Fourth Edition Editors Harjit Singh, MD, FSIR Janet A Neutze, MD Professor of Radiology, Surgery, Associate Professor of Radiology and Medicine Associate Division Chief, Ultrasound Director of Education, Penn State Heart Co-director, Radiology Medical Student and Vascular Institute Education Program Fellowship Director, Cardiovascular Pennsylvania State College of Medicine and Interventional Radiology Penn State Hershey Medical Center Pennsylvania State College of Medicine Hershey, PA, USA Penn State Hershey Medical Center [email protected] Hershey, PA, USA [email protected] Associate Editors Jonathan R Enterline, MD Joseph S Fotos, MD Resident, Department of Radiology Resident, Department of Radiology Pennsylvania State College of Medicine Pennsylvania State College of Medicine Penn State Hershey Medical Center Penn State Hershey Medical Center Hershey, PA, USA Hershey, PA, USA Contributing Editors Jonathan J Douds, BS Megan Jenkins Kalambo, MD Medical Student Resident, Department of Radiology Pennsylvania State College of Medicine University of Texas Health Science Center Penn State Hershey Medical Center at Houston, Houston, TX, USA Hershey, PA, USA Marsha J Bluto, MD Practicing Physician Physical Medicine and Rehabilitation Mill Valley, CA, USA ISBN 978-1-4614-0943-4 e-ISBN 978-1-4614-0944-1 DOI 10.1007/978-1-4614-0944-1 Springer New York Dordrecht Heidelberg London Library of Congress Control Number: 2011938463 © Springer Science+Business Media, LLC 2012 All rights reserved. This work may not be translated or copied in whole or in part without the written permission of the publisher (Springer Science+Business Media, LLC, 233 Spring Street, New York, NY 10013, USA), except for brief excerpts in connection with reviews or scholarly analysis. -

Chest Radiology
RADIOLOGY RESIDENCY HANDBOOK FOR CHEST RADIOLOGY Section of Cardiothoracic Radiology Department of Diagnostic Radiology Beaumont Health – Farmington Hills Botsford Campus Reehan Ali, DO Section Chief Cardiothoracic Radiology Rocky Saenz, DO – Program Director Timothy McKnight, DO – Assistant Program Director Michael Schwartz, MD – Department Chairman Updated July 2015 to meet NAS Standards GOALS AND OBJECTIVES ROTATION 1 Competency-Based Goals & Objectives Medical Knowledge Understand the various factors that affect a quality radiograph Understand the technique and quality control for chest radiography from patient positioning to the images on PACS Learn a methodical approach to analyzing a chest radiograph. Develop skills in interpretation of chest radiography Correlate pathologic and clinical data with radiographic findings. Monitor chest exams and determine if additional images are necessary. Begin to develop skills in differential diagnosis Demonstrate ability to appropriately order follow-up imaging. State clinical indications for performing chest radiography. Dictate accurate, concise radiography reports. Patient Care Read and/or dictate images with the assistance/review of faculty radiologists. Make preliminary decisions on all matters of image interpretation and consultation, recognizing need for and obtaining assistance in situations that require expertise of faculty radiologist. Develop an understanding of ACR appropriateness criteria for chest radiology imaging. Demonstrate knowledge of parameters contributing to patient radiation exposure and techniques used to limit radiation exposure. Act as a consultant to referring clinicians and recommend appropriate use of imaging studies. Professionalism Recognize limitations in personal knowledge and skills, being careful to not make decisions beyond the level of personal competence. Demonstrate compassion (be understanding and respectful of patient, their families, and medical colleagues). -
Core Exam Study Guide
Diagnostic Radiology CORE Examination Study Guide Updated 8/25/2018 C o r e E x a m i n a t i o n S t u d y G u i d e Contents Contents Preamble ...................................................................................................................................................... 3 Exam Purpose Statements ............................................................................................................................4 Breast Imaging ............................................................................................................................................. 5 Cardiac Imaging............................................................................................................................................7 Gastrointestinal Imaging............................................................................................................................. 12 Interventional Radiology............................................................................................................................. 18 Musculoskeletal Imaging ............................................................................................................................ 20 Neuroradiology ........................................................................................................................................... 30 Nuclear Radiology ....................................................................................................................................... 45 Pediatric Radiology .................................................................................................................................... -

Cardiothoracic Radiology Resident Rotations Academic Year 2016-2017
Cardiothoracic Radiology Resident Rotations Academic Year 2016-2017 Goals and Objectives based on Core Competencies Introduction: Components of a cardiothoracic radiology curriculum may occur during one or more organ- specific or technology-specific rotations during residency, including rotations in chest radiology, cardiac radiology, pediatric radiology, nuclear medicine, magnetic resonance imaging, computed tomography, fluoroscopy (e.g. sniff test) and interventional radiology (e.g. lung biopsy procedure skills) and include training and experience in plain film interpretation, computed tomography (CT), magnetic resonance imaging (MRI), ultrasonography, angiography, and nuclear radiology examinations related to pulmonary, pleural, mediastinal and cardiovascular disease. Cardiothoracic radiology rotations at DHMC combine chest radiography (CXR) and CT and cardiac CT and MRI. This structure reflects the proposed guidelines for diagnostic radiology core curriculum as laid out by the Residency Restructuring Committee of the Association of Program Directors in Radiology (J Am Coll Radiol 2010;7:507-511) which DHMC Radiology Chair Dr. Jocelyn Chertoff co-authored. Non-cardiac chest MR are typically covered by the Body MR service. Chest interventional procedures, e.g. lung biopsies and pleural fluid drainage, are services provided by Interventional Radiology and Body CT. Body CT also helps read Chest CTs, depending on volumes, but may defer certain CTs to chest imagers based on diagnosis and/or findings that would benefit from cardiothoracic specialist interpretation. General Clinical Responsibilities and Workload: Cardiothoracic radiology at DHMC consists of at least three rotations, usually four weeks in length. During the first rotation, emphasis is primarily on CXR but also with significant exposure to the entire gamut of chest CT examinations.