Anti Anginal Drugs
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Tolerance and Resistance to Organic Nitrates in Human Blood Vessels
\ö-\2- Tolerance and Resistance to Organic Nitrates in Human Blood Vessels Peter Radford Sage MBBS, FRACP Thesis submit.ted for the degree of Doctor of Philosuphy Department of Medicine University of Adelaide and Cardiology Unit The Queen Elizabeth Hospital I Table of Gontents Summary vii Declaration x Acknowledgments xi Abbreviations xil Publications xtil. l.INTRODUCTION l.L Historical Perspective I i.2 Chemical Structure and Available Preparations I 1.3 Cellular/biochemical mechanism of action 2 1.3.1 What is the pharmacologically active moiety? 3 1.3.2 How i.s the active moiety formed? i 4 1.3.3 Which enzyme system(s) is involved in nitrate bioconversi<¡n? 5 1.3.4 What is the role of sulphydryl groups in nitrate action? 9 1.3.5 Cellular mechanism of action after release of the active moiety 11 1.4 Pharmacokinetics t2 1.5 Pharmacological Effects r5 1.5.1 Vascular effects 15 l.5.2Platelet Effects t7 1.5.3 Myocardial effects 18 1.6 Clinical Efhcacy 18 1.6.1 Stable angina pectoris 18 1.6.2 Unstable angina pectoris 2t 1.6.3 Acute myocardial infarction 2l 1.6.4 Congestive Heart Failure 23 ll 1.6.5 Other 24 1.7 Relationship with the endothelium and EDRF 24 1.7.1 EDRF and the endothelium 24 1.7.2 Nitrate-endothelium interactions 2l 1.8 Factors limiting nitrate efficacy' Nitrate tolerance 28 1.8.1 Historical notes 28 1.8.2 Clinical evidence for nitrate tolerance 29 1.8.3 True/cellular nitrate tolerance 31 1.8.3.1 Previous studies 31 | .8.3.2 Postulated mechanisms of true/cellular tolerance JJ 1.8.3.2.1 The "sulphydryl depletion" hypothesis JJ 1.8.3.2.2 Desensitization of guanylate cyclase 35 1 8.i.?..3 Impaired nitrate bioconversion 36 1.8.3.2.4'Ihe "superoxide hypothesis" 38 I.8.3.2.5 Other possible mechanisms 42 1.8.4 Pseudotolerance ; 42 1.8.4. -

Molecular Mechanisms Underlying Ketamine-Mediated Inhibition Of
Anesthesiology 2005; 102:93–101 © 2004 American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. Molecular Mechanisms Underlying Ketamine-mediated Inhibition of Sarcolemmal Adenosine Triphosphate- sensitive Potassium Channels Takashi Kawano, M.D.,* Shuzo Oshita, M.D.,† Akira Takahashi, M.D.,‡ Yasuo Tsutsumi, M.D.,* Katsuya Tanaka, M.D.,§ Yoshinobu Tomiyama, M.D., Hiroshi Kitahata, M.D.,# Yutaka Nakaya, M.D.** Background: Ketamine inhibits adenosine triphosphate-sen- sensitive channel pore.3 These channels, as metabolic sitive potassium (KATP) channels, which results in the blocking sensors, are associated with such cellular functions as of ischemic preconditioning in the heart and inhibition of va- insulin secretion, cardiac preconditioning, vasodilata- sorelaxation induced by KATP channel openers. In the current 4–7 Downloaded from http://pubs.asahq.org/anesthesiology/article-pdf/102/1/93/357819/0000542-200501000-00017.pdf by guest on 27 September 2021 study, the authors investigated the molecular mechanisms of tion, and neuroprotection. ketamine’s actions on sarcolemmal KATP channels that are re- In cardiac myocytes, intravenous general anesthetics, associated by expressed subunits, inwardly rectifying potas- such as ketamine racemate, propofol, and thiamylal, di- sium channels (Kir6.1 or Kir6.2) and sulfonylurea receptors 8–10 rectly inhibit native sarcolemmal KATP channels. Al- (SUR1, SUR2A, or SUR2B). though these observations suggest that intravenous an- Methods: The authors used inside-out patch clamp configura- tions to investigate the effects of ketamine on the activities of esthetics may impair the endogenous organ protective reassociated Kir6.0/SUR channels containing wild-type, mutant, mechanisms mediated by KATP channels, the possibility or chimeric SURs expressed in COS-7 cells. -
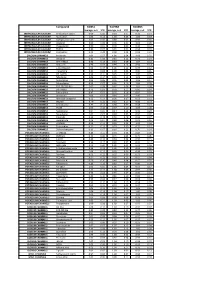
Biomol Average and SD Table S1.Xlsx
Compound GliNS1 G179NS G166NS average, n=5 STD average, n=3 STD average, n=3 STD INTRACELLULAR CALCIUM Antibiotic A-23187 0.00 0.00 0.10 0.07 0.15 0.14 INTRACELLULAR CALCIUM Ryanodine 1.04 0.14 1.03 0.03 1.03 0.03 INTRACELLULAR CALCIUM Cyclopiazonic acid 1.01 0.06 0.88 0.05 0.92 0.06 INTRACELLULAR CALCIUM Gingerol 1.00 0.06 0.91 0.01 1.01 0.06 INTRACELLULAR CALCIUM Thapsigargin 0.00 0.01 0.00 0.00 0.10 0.12 INTRACELLULAR CALCIUM TMB-8 0.89 0.07 0.91 0.05 0.94 0.03 INTRACELLULAR CALCIUM Dantrolene 0.91 0.08 0.98 0.05 0.94 0.01 CALCIUM CHANNELS Amiloride 1.01 0.07 1.01 0.04 1.03 0.05 CALCIUM CHANNELS Benzamil 0.83 0.08 0.83 0.12 0.96 0.04 CALCIUM CHANNELS BAY K-8644 0.93 0.13 0.93 0.09 1.07 0.14 CALCIUM CHANNELS Diltiazem 0.96 0.07 0.99 0.12 0.94 0.14 CALCIUM CHANNELS L-cis-Diltiazem 0.91 0.17 1.01 0.12 0.95 0.12 CALCIUM CHANNELS Flunarizine 0.85 0.08 1.00 0.06 0.85 0.05 CALCIUM CHANNELS FPL-64176 0.99 0.11 0.95 0.07 1.05 0.05 CALCIUM CHANNELS Nifedipine 1.06 0.17 0.95 0.12 1.03 0.09 CALCIUM CHANNELS Nimodipine 1.05 0.06 0.95 0.03 1.06 0.17 CALCIUM CHANNELS Nitrendipine 0.99 0.07 0.96 0.10 1.04 0.09 CALCIUM CHANNELS SDZ-202791 R(-) 1.01 0.08 0.92 0.06 1.01 0.08 CALCIUM CHANNELS SKF-96365 0.73 0.05 0.70 0.11 0.69 0.04 CALCIUM CHANNELS Tetrandrine 0.47 0.07 0.76 0.16 0.87 0.20 CALCIUM CHANNELS Verapamil 1.01 0.02 0.89 0.07 1.06 0.20 CALCIUM CHANNELS Methoxy Verapamil 0.93 0.14 0.96 0.07 0.93 0.13 CALCIUM CHANNELS Bepridil 0.70 0.16 0.92 0.15 0.84 0.14 CALCIUM CHANNELS Amiodarone 0.32 0.12 0.58 0.07 0.48 0.23 CALCIUM CHANNELS YS035 1.00 0.16 -

Alphabetical Listing by Therapeutic Category GOODFELLOW AFB ROSS CLINIC FORMULARY
GOODFELLOW AFB ROSS CLINIC FORMULARY Alphabetical Listing by Therapeutic Category This document is current as of October 8, 2020. The availability of formulary items is subject to change. ACARBOSE Acarbose ALPRAZolam Outpatient Dosage Forms Outpatient Formulary Brands Available Xanax Tablet, Oral: Outpatient Dosage Forms Generic: 25 mg, 50 mg, 100 mg Tablet, Oral: Xanax: 0.5 mg, 1 mg [scored] Acetaminophen Generic: 0.5 mg, 1 mg Outpatient Formulary Brands Available Mapap Children's [OTC]; Mapap [OTC] Aluminum Chloride Hexahydrate Outpatient Dosage Forms Outpatient Formulary Brands Available Drysol Suspension, Oral: Outpatient Dosage Forms Mapap Children's: 160 mg/5 mL (118 mL) [ethanol free; contains propylene Solution, External: glycol, sodium benzoate; cherry flavor] Drysol: 20% (60 mL) Tablet, Oral: Mapap: 325 mg Aluminum Hydroxide, Magnesium Hydroxide, and Simethicone Generic: 325 mg Outpatient Dosage Forms Liquid, Oral: Acetaminophen and Codeine Generic: Aluminum hydroxide 200 mg, magnesium hydroxide 200 mg, and Outpatient Dosage Forms simethicone 20 mg per 5 mL (360 mL) Solution, Oral [C-V]: Generic: Acetaminophen 120 mg and codeine phosphate 12 mg per 5 mL Amantadine (118 mL) [BCF] Outpatient Dosage Forms Tablet, Oral [C-III]: Capsule, Oral, as hydrochloride: Generic: Acetaminophen 300 mg and codeine phosphate 30 mg [BCF] Generic: 100 mg [BCF] AcetaZOLAMIDE Amiodarone Outpatient Dosage Forms Outpatient Dosage Forms Tablet, Oral: Tablet, Oral, as hydrochloride: Generic: 250 mg Generic: 200 mg [BCF] Acetic Acid, Propylene Glycol Diacetate, -

The In¯Uence of Medication on Erectile Function
International Journal of Impotence Research (1997) 9, 17±26 ß 1997 Stockton Press All rights reserved 0955-9930/97 $12.00 The in¯uence of medication on erectile function W Meinhardt1, RF Kropman2, P Vermeij3, AAB Lycklama aÁ Nijeholt4 and J Zwartendijk4 1Department of Urology, Netherlands Cancer Institute/Antoni van Leeuwenhoek Hospital, Plesmanlaan 121, 1066 CX Amsterdam, The Netherlands; 2Department of Urology, Leyenburg Hospital, Leyweg 275, 2545 CH The Hague, The Netherlands; 3Pharmacy; and 4Department of Urology, Leiden University Hospital, P.O. Box 9600, 2300 RC Leiden, The Netherlands Keywords: impotence; side-effect; antipsychotic; antihypertensive; physiology; erectile function Introduction stopped their antihypertensive treatment over a ®ve year period, because of side-effects on sexual function.5 In the drug registration procedures sexual Several physiological mechanisms are involved in function is not a major issue. This means that erectile function. A negative in¯uence of prescrip- knowledge of the problem is mainly dependent on tion-drugs on these mechanisms will not always case reports and the lists from side effect registries.6±8 come to the attention of the clinician, whereas a Another way of looking at the problem is drug causing priapism will rarely escape the atten- combining available data on mechanisms of action tion. of drugs with the knowledge of the physiological When erectile function is in¯uenced in a negative mechanisms involved in erectile function. The way compensation may occur. For example, age- advantage of this approach is that remedies may related penile sensory disorders may be compen- evolve from it. sated for by extra stimulation.1 Diminished in¯ux of In this paper we will discuss the subject in the blood will lead to a slower onset of the erection, but following order: may be accepted. -

Drug Class Review Antianginal Agents
Drug Class Review Antianginal Agents 24:12.08 Nitrates and Nitrites 24:04.92 Cardiac Drugs, Miscellaneous Amyl Nitrite Isosorbide Dinitrate (IsoDitrate ER®, others) Isosorbide Mononitrate (Imdur®) Nitroglycerin (Minitran®, Nitrostat®, others) Ranolazine (Ranexa®) Final Report May 2015 Review prepared by: Melissa Archer, PharmD, Clinical Pharmacist Carin Steinvoort, PharmD, Clinical Pharmacist Gary Oderda, PharmD, MPH, Professor University of Utah College of Pharmacy Copyright © 2015 by University of Utah College of Pharmacy Salt Lake City, Utah. All rights reserved. Table of Contents Executive Summary ......................................................................................................................... 3 Introduction .................................................................................................................................... 4 Table 1. Antianginal Therapies .............................................................................................. 4 Table 2. Summary of Agents .................................................................................................. 5 Disease Overview ........................................................................................................................ 8 Table 3. Summary of Current Clinical Practice Guidelines .................................................... 9 Pharmacology ............................................................................................................................... 10 Table 4. Pharmacokinetic Properties -

(12) United States Patent (10) Patent No.: US 6,641,839 B1 Geoghegan Et Al
USOO6641839B1 (12) United States Patent (10) Patent No.: US 6,641,839 B1 Geoghegan et al. (45) Date of Patent: Nov. 4, 2003 (54) PHARMACEUTICAL FORMULATIONS FOR JP 59 84.820 5/1984 PREVENTING DRUG TOLERANCE JP 62126127 * 6/1987 (75) Inventors: Edward James Geoghegan, Athlone OTHER PUBLICATIONS (IE); Seamus Mulligan, Athlone (IE); “Isosorbide-5-Nitrate Sustained-release pellets-an Mary Margaret Foynes, Athlone (IE) example of computer Supported drug development', Zerbe et al., Pharmacuetical Resarch 1985, No. 1, Jan., pp. 30–36. (73) Assignee: Athpharma Limited, Roscommon (IE) “Glyceryl trinitrate (nitroglycerine) and the Organic nitrates choosing the method of administration”, J. Abrahms, Drugs (*) Notice: Subject to any disclaimer, the term of this 34; 391-403 (1987). patent is extended or adjusted under 35 “Dose Dependence of Tolerance during treatment with U.S.C. 154(b) by 407 days. mono-nitrates', M. Tauchert et al., Z. Cardiol. 72, Suppl. 3, 218–228 (1983). (21) Appl. No.: 08/797,318 “Tolerance Development during isosorbide dinitrate treat ment: Can it be circumvented?”, W. Rudolf et al., Z. Cardiol. (22) Filed: Feb. 7, 1997 72, Supple. 3, 195-198 (1983). Related U.S. Application Data “Anti-ischemic effects of 80mg tablet of isosorbide dinitrate in Sustained-release form before and after two weeks treat (63) Continuation of application No. 08/419,520, filed on Apr. ment with 80mg once daily or twice daily', S.Silver et al., 10, 1995, which is a continuation of application No. 08/320, Z.Cardiol. 72, Suppl. 3, 211-217 (1983). 599, filed on Oct. 11, 1994, which is a continuation of application No. -

Cardiovascular Drugs and Therapies NITRATES COMPARISON CHART
Cardiovascular Drugs and Therapies NITRATES COMPARISON CHART Isosorbide Generic Nitroglycerin Nitroglycerin Nitroglycerin Nitroglycerin Dinitrate Isosorbide Isosorbide Name Intravenous Patch Ointment Sublingual Sublingual Dinitrate 5-Mononitrate Trade Name TRIDIL, NITRODUR, NITROL NITROLINGUAL generics generics (for IMDUR, generics TRANSDERM- Pumpspray, immediate generics NITRO, RHO-NITRO release) MINITRAN, Pumpspray, SR: no longer TRINIPATCH NITROLINGUAL available Metered dose spray NITROSTAT sublingual tablet Dosage 100 mg/250 mL 0.2 mg/h 30 g/30 inches SL spray: SL tablet: 5mg Immediate SR tablet: Forms premixed bottle 0.4 mg/h ointment 0.4 mg/ dose release 60 mg SR - UHN 0.6 mg/h SL tablet: tablet: Note: 0.84 mL 0.8 mg/h 0.3 mg, 0.6 mg 10 mg *Non- alcohol per 100 mL 30 mg formulary at solution UHN 100 mcg/mL 200 mcg/mL 400 mcg/mL 10 mg/10 mL vial - UHN 50 mg/10 mL vial - UHN CARDIOVASCULAR PHARMACOTHERAPY HANDBOOK All contents copyright © University Health Network. All rights reserved Cardiovascular Drugs and Therapies NITRATES COMPARISON CHART Isosorbide Generic Nitroglycerin Nitroglycerin Nitroglycerin Nitroglycerin Dinitrate Isosorbide Isosorbide Name Intravenous Patch Ointment Sublingual Sublingual Dinitrate 5-Mononitrate Dosing Starting and 0.2 to 0.8 ½ inch to 1 inch SL spray: SL tablet: Immediate 60-240 mg SR Usual dose target doses mg/h once tid-qid; remove 0.4 mg prn; 5-10 mg q2-4h release: once daily range are determined daily. for 8-10 hours dose may be for prophylaxis 10-45 mg tid by clinical per 24-hour repeated after of acute angina on qid situation and 12-14 hour period; 5 minutes for schedule the number and patch-free response to interval e.g., ON 0600, total of 3 doses (e.g. -
2013 ESC Guidelines on the Management of Stable Coronary
European Heart Journal Advance Access published August 30, 2013 European Heart Journal ESC GUIDELINES doi:10.1093/eurheartj/eht296 2013 ESC guidelines on the management of stable coronary artery disease The Task Force on the management of stable coronary artery disease of the European Society of Cardiology Task Force Members: Gilles Montalescot* (Chairperson) (France), Udo Sechtem* (Chairperson) (Germany), Stephan Achenbach (Germany), Felicita Andreotti (Italy), Chris Arden (UK), Andrzej Budaj (Poland), Raffaele Bugiardini (Italy), Filippo Crea Downloaded from (Italy), Thomas Cuisset (France), Carlo Di Mario (UK), J. Rafael Ferreira (Portugal), Bernard J. Gersh (USA), Anselm K. Gitt (Germany), Jean-Sebastien Hulot (France), Nikolaus Marx (Germany), Lionel H. Opie (South Africa), Matthias Pfisterer (Switzerland), Eva Prescott (Denmark), Frank Ruschitzka (Switzerland), Manel Sabate´ http://eurheartj.oxfordjournals.org/ (Spain), Roxy Senior (UK), David Paul Taggart (UK), Ernst E. van der Wall (Netherlands), Christiaan J.M. Vrints (Belgium). ESC Committee for Practice Guidelines (CPG): Jose Luis Zamorano (Chairperson) (Spain), Stephan Achenbach (Germany), Helmut Baumgartner (Germany), Jeroen J. Bax (Netherlands), He´ctor Bueno (Spain), Veronica Dean (France), Christi Deaton (UK), Cetin Erol (Turkey), Robert Fagard (Belgium), Roberto Ferrari (Italy), David Hasdai (Israel), Arno W. Hoes (Netherlands), Paulus Kirchhof (Germany/UK), Juhani Knuuti (Finland), Philippe Kolh (Belgium), Patrizio Lancellotti (Belgium), Ales Linhart (Czech Republic), Petros Nihoyannopoulos (UK), Massimo F. Piepoli (Italy), Piotr Ponikowski (Poland), Per Anton Sirnes (Norway), Juan Luis Tamargo (Spain), Michal Tendera (Poland), by guest on September 16, 2015 Adam Torbicki (Poland), William Wijns (Belgium), Stephan Windecker (Switzerland). Document Reviewers: Juhani Knuuti (CPG Review Coordinator) (Finland), Marco Valgimigli (Review Coordinator) (Italy), He´ctor Bueno (Spain), Marc J. -

Exogenous Nitric Oxide Inhibits Rho-Associated Kinase Activity in Patients with Angina Pectoris: a Randomized Controlled Trial
Hypertension Research (2015) 38, 485–490 & 2015 The Japanese Society of Hypertension All rights reserved 0916-9636/15 www.nature.com/hr ORIGINAL ARTICLE Exogenous nitric oxide inhibits Rho-associated kinase activity in patients with angina pectoris: a randomized controlled trial Tatsuya Maruhashi1,5, Kensuke Noma2,5, Noritaka Fujimura1, Masato Kajikawa1, Takeshi Matsumoto1, Takayuki Hidaka1, Ayumu Nakashima3, Yasuki Kihara1, James K Liao4 and Yukihito Higashi2 The RhoA/Rho-associated kinase (ROCK) pathway has a key physiological role in the pathogenesis of atherosclerosis. Increased ROCK activity is associated with cardiovascular diseases. Endogenous nitric oxide (NO) has an anti-atherosclerotic effect, whereas the exogenous NO-mediated cardiovascular effect still remains controversial. The purpose of this study was to evaluate the effect of exogenous NO on ROCK activity in patients with angina pectoris. This is a prospective, open-label, randomized, controlled study. A total of 30 patients with angina pectoris were randomly assigned to receive 40 mg day − 1 of isosorbide mononitrate (n = 15, 12 men and 3 women, mean age of 63 ± 12 years, isosorbide mononitrate group) or conventional treatment (n = 15, 13 men and 2 women, mean age of 64 ± 13 years, control group) for 12 weeks. ROCK activity in peripheral leukocytes was measured by western blot analysis. ROCK activities at 4 and 12 weeks after treatment were decreased in the isosorbide mononitrate group (0.82 ± 0.33 at 0 week, 0.62 ± 0.20 at 4 weeks, 0.61 ± 0.19 at 12 weeks, n = 15 in each group, Po0.05, respectively) but not altered in the control group. ROCK1 and ROCK2 expression levels were similar in all treatment periods in the two groups. -
Label-Free Cell Phenotypic Profiling Decodes the Composition And
OPEN Label-free cell phenotypic profiling SUBJECT AREAS: decodes the composition and signaling POTASSIUM CHANNELS SENSORS AND PROBES of an endogenous ATP-sensitive Received potassium channel 28 January 2014 Haiyan Sun1*, Ying Wei1, Huayun Deng1, Qiaojie Xiong2{, Min Li2, Joydeep Lahiri1 & Ye Fang1 Accepted 24 April 2014 1Biochemical Technologies, Science and Technology Division, Corning Incorporated, Corning, NY 14831, United States of Published America, 2The Solomon H. Snyder Department of Neuroscience and High Throughput Biology Center, Johns Hopkins University 12 May 2014 School of Medicine, Baltimore, Maryland 21205, United States of America. Current technologies for studying ion channels are fundamentally limited because of their inability to Correspondence and functionally link ion channel activity to cellular pathways. Herein, we report the use of label-free cell requests for materials phenotypic profiling to decode the composition and signaling of an endogenous ATP-sensitive potassium should be addressed to ion channel (KATP) in HepG2C3A, a hepatocellular carcinoma cell line. Label-free cell phenotypic agonist Y.F. (fangy2@corning. profiling showed that pinacidil triggered characteristically similar dynamic mass redistribution (DMR) com) signals in A431, A549, HT29 and HepG2C3A, but not in HepG2 cells. Reverse transcriptase PCR, RNAi knockdown, and KATP blocker profiling showed that the pinacidil DMR is due to the activation of SUR2/ Kir6.2 KATP channels in HepG2C3A cells. Kinase inhibition and RNAi knockdown showed that the pinacidil * Current address: activated KATP channels trigger signaling through Rho kinase and Janus kinase-3, and cause actin remodeling. The results are the first demonstration of a label-free methodology to characterize the Biodesign Institute, composition and signaling of an endogenous ATP-sensitive potassium ion channel. -

Use of Sildenafil in Patients with Cardiovascular Disease
Arq Bras Cardiol GuimarãesReview et al volume 73, (nº6), 1999 Sildenafil in patients with cardiovascular disease Use of Sildenafil in Patients with Cardiovascular Disease Armênio Costa Guimarães, Marcus Vinícius Bolívar Malachias, Otávio Rizzi Coelho, Emílio Cesar Zilli, Rafael Leite Luna Introduction of phosphodiesterase inhibitors. The erectile action of sildenafil combines increase in arterial flow with reduction Erectile dysfunction, formerly called impotence, is the in the venous flow of cavernous body of penis. Sildenafil inability of the male to achieve or maintain penile erection and leads to relaxation of smooth muscle of penile arteries and thus engage in coitus1. It is common among patients with trabeculae surrounding the sinusoidal spaces, resulting in cardiovascular diseases or their risk factors. This dysfunc- a greater engorgement of cavernous body. The trabeculae tion occurs mainly among individuals with coronary artery of engorged sinusoidal spaces compress the penile disease, after episodes of acute ischemic syndrome, hyper- venules against the tunica albuginea, reducing venous tensive patients underpharmacologic treatment, and among flow, contributing to maintenance of engorgement of patients with heart failure. In approximately 85% of these ca- cavernous body8. Relaxation of this smooth muscle ses, the fear of a cardiac event during coitus constitutes an results from a decrease in intracellular calcium mediated important factor for erectile dysfunction 2-4. by accumulation of the second messenger, the cyclic Discovery of sildenafil citrate has represented a great de- guanosine monophosphate (cGMP), whose production velopment in the treatment of erectile dysfunction; it may results from activation of guanyl cyclase by nitric oxide benefit, among many others, those patients with cardiovascu- produced by the stimulus of endothelial cells generated lar diseases or with their risk factors 5.