OCCUPATIONAL NEOPLASTIC DISEASE the Extensive
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Recognizing When a Child's Injury Or Illness Is Caused by Abuse
U.S. Department of Justice Office of Justice Programs Office of Juvenile Justice and Delinquency Prevention Recognizing When a Child’s Injury or Illness Is Caused by Abuse PORTABLE GUIDE TO INVESTIGATING CHILD ABUSE U.S. Department of Justice Office of Justice Programs 810 Seventh Street NW. Washington, DC 20531 Eric H. Holder, Jr. Attorney General Karol V. Mason Assistant Attorney General Robert L. Listenbee Administrator Office of Juvenile Justice and Delinquency Prevention Office of Justice Programs Innovation • Partnerships • Safer Neighborhoods www.ojp.usdoj.gov Office of Juvenile Justice and Delinquency Prevention www.ojjdp.gov The Office of Juvenile Justice and Delinquency Prevention is a component of the Office of Justice Programs, which also includes the Bureau of Justice Assistance; the Bureau of Justice Statistics; the National Institute of Justice; the Office for Victims of Crime; and the Office of Sex Offender Sentencing, Monitoring, Apprehending, Registering, and Tracking. Recognizing When a Child’s Injury or Illness Is Caused by Abuse PORTABLE GUIDE TO INVESTIGATING CHILD ABUSE NCJ 243908 JULY 2014 Contents Could This Be Child Abuse? ..............................................................................................1 Caretaker Assessment ......................................................................................................2 Injury Assessment ............................................................................................................4 Ruling Out a Natural Phenomenon or Medical Conditions -

Nasolabial and Forehead Flap Reconstruction of Contiguous Alar
Journal of Plastic, Reconstructive & Aesthetic Surgery (2017) 70, 330e335 Nasolabial and forehead flap reconstruction of contiguous alareupper lip defects Jonathan A. Zelken a,b, Sashank K. Reddy c, Chun-Shin Chang a, Shiow-Shuh Chuang a, Cheng-Jen Chang a, Hung-Chang Chen a, Yen-Chang Hsiao a,* a Department of Plastic and Reconstructive Surgery, Chang Gung Memorial Hospital, College of Medicine, Chang Gung University, Taipei, Taiwan b Department of Plastic and Reconstructive Surgery, Breastlink Medical Group, Laguna Hills, CA, USA c Department of Plastic and Reconstructive Surgery, Johns Hopkins Hospital, Baltimore, MD, USA Received 4 May 2016; accepted 31 October 2016 KEYWORDS Summary Background: Defects of the nasal ala and upper lip aesthetic subunits can be Nasal reconstruction; challenging to reconstruct when they occur in isolation. When defects incorporate both Nasolabial flap; the subunits, the challenge is compounded as subunit boundaries also require reconstruc- Rhinoplasty; tion, and local soft tissue reservoirs alone may provide inadequate coverage. In such cases, Forehead flap we used nasolabial flaps for upper lip reconstructionandaforeheadflapforalarrecon- struction. Methods: Three men and three women aged 21e79 years (average, 55 years) were treated for defects of the nasal ala and upper lip that resulted from cancer (n Z 4) and trauma (n Z 2). Unaffected contralateral subunits dictated the flap design. The upper lip subunit was excised and replaced with a nasolabial flap. The flap, depending on the contralateral reference, determined accurate alar base position. A forehead flap resurfaced or replaced the nasal ala. Autologous cartilage was used in every case to fortify the forehead flap reconstruction. Results: Patients were followed for 25.6 months (range, 1e4 years). -

Exposure to Carcinogens and Work-Related Cancer: a Review of Assessment Methods
European Agency for Safety and Health at Work ISSN: 1831-9343 Exposure to carcinogens and work-related cancer: A review of assessment methods European Risk Observatory Report Exposure to carcinogens and work-related cancer: A review of assessment measures Authors: Dr Lothar Lißner, Kooperationsstelle Hamburg IFE GmbH Mr Klaus Kuhl (task leader), Kooperationsstelle Hamburg IFE GmbH Dr Timo Kauppinen, Finnish Institute of Occupational Health Ms Sanni Uuksulainen, Finnish Institute of Occupational Health Cross-checker: Professor Ulla B. Vogel from the National Working Environment Research Centre in Denmark Project management: Dr Elke Schneider - European Agency for Safety and Health at Work (EU-OSHA) Europe Direct is a service to help you find answers to your questions about the European Union Freephone number (*): 00 800 6 7 8 9 10 11 (*) Certain mobile telephone operators do not allow access to 00 800 numbers, or these calls may be billed. More information on the European Union is available on the Internet ( 48TU http://europa.euU48T). Cataloguing data can be found on the cover of this publication. Luxembourg: Publications Office of the European Union, 2014 ISBN: 978-92-9240-500-7 doi: 10.2802/33336 Cover pictures: (clockwise): Anthony Jay Villalon (Fotolia); ©Roman Milert (Fotolia); ©Simona Palijanskaite; ©Kari Rissa © European Agency for Safety and Health at Work, 2014 Reproduction is authorised provided the source is acknowledged. European Agency for Safety and Health at Work – EU-OSHA 1 Exposure to carcinogens and work-related cancer: -
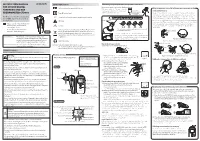
Instruction Manual for Citizen Digital Forehead And
INSTRUCTION MANUAL Symbol Explanations Measuring body temperature (temperature detection) Remove the probe cap and check the probe tip. FOR CITIZEN DIGITAL Refer to instruction manual before use. How to measure correctly in the ear measurement mode * When using it for the first time, open the FOREHEAD AND EAR battery cap and remove the insulation Open the Temperature basics battery cap to THERMOMETER CTD710 Type BF applied part sheet under the battery cap. remove the All objects radiate heat. This device consists of a probe with a built-in insulation sheet. infrared sensor that measures body temperature by detecting the heat Thank you very much for purchasing IP22 Classification for water ingress and particulate matter. radiated by the eardrum and surrounding tissue. Figure 4 shows the the CITIZEN digital forehead and ear Keeping the probe window clean tortuous anatomy of a normal ear canal. As shown in Figure 5, hold the thermometer. Warning Probe window ear and gently pull it back at an angle or pull it straight back to straighten out the ear canal. The shape of the ear canal differs from individual, check • Please read all of the information in before measurement. Accurate temperature measurements make it this instruction manual before Caution essential to straighten the ear canal so that the probe tip directly faces operating the device. the eardrum. • Be sure to have this instruction Indicates this device is subject to the Waste Electrical and Dirt in the probe window will impact the accuracy of temperature detection. External auditory manual to hand during use. 1902LA Electronic Equipment Directive in the European Union. -

2. Bilateral Cleft Anatomy 19
BILATERAL CLEFT ANATOMY IS ATTACHED TO THE SINGLE CLEFT THE PREMAXILLA NORMALLY ROTATED OUTWARD MAXILLA ON ONE SIDE AND THIS ENTIRE COMPONENT IS THE CLEFT SIDE MAXILLA IN AN VARYING DEGREES FROM ASYMMETRICAL DIFFERENT DISTORTION DOUBLE CLEFTS PRESENT AN ENTIRELY CONFIGURA TION IN THE COMPLETE BILATERAL CLEFT THE PREMAXILLA IS UNATTACHED THREE WHICH TO EITHER MAXILLA THUS THERE ARE SEPARATE COMPONENTS IN THEIR DISTORTION THE MAXILLAE ARE MORE OR LESS SYMMETRICAL TWO WHILE THE ARE USUALLY EQUAL TO EACH OTHER IN SIZE AND POSITION FORWARD ITS IN CENTRAL PREMAXILLARY ELEMENT PROCEEDS ON OWN WITHIN ITSELF FOR DIFFERENT DEGREES BUT WITH SYMMETRY EXCEPT IJI POSSIBLE DEVIATION FRONTONASAL THE COMPLETE SEPARATION OF THE CENTRAL COMPONENT OF PROLABIUM AND PREMAXILLA FROM THE LATERAL MAXILLARY SEGMENTS THE VASCULAR ABNORMALLY INFLUENCES NOSE PHILTRUM MUSCULATURE AND OF ALL THREE ELEMENTS ITY NERVE SUPPLY GROWTH DEVELOPMENT WHERE THE CLEFT IS INCOMPLETE ON BOTH SIDES THE DEFORMITY IS LESS AND IS STILL SYMMETRICAL IN SUCH CASE THERE IS USUALLY MORE OR LESS INTACT ALVEOLUS AND LITTLE OR NO PROTRUSION OF THE PRE THE MAXILLA THE COLUMELLA IS LIKELY TO BE LONGER THAN IN COMPLETE CLEFT BUT NOT OF NORMAL LENGTH SOMETIMES SOMETIMES THE DEGREE OF CLEFT VARIES ON EACH SIDE SIDE THE INCOMPLETENESS SHOWS AS ONLY THE SLIGHTEST NOTCH ON ONE SIDE OR THERE CLEFT ON THE OPPOSITE AND HALFWAY OR THREEQUARTER ON THE CLEFT ONE SIDE AND AN INCOMPLETE ONE CAN BE COMPLETE ON OF THE EXASPERATING ASPECT OTHER WHICH CONDITION EXAGGERATES THE ROTATION OF THE IN THE AND NOSE -

Ear and Forehead Thermometer
Ear and Forehead Thermometer INSTRUCTION MANUAL Item No. 91807 19.PJN174-14_GA-USA_HHD-Ohrthermometer_DSO364_28.07.14 Montag, 28. Juli 2014 14:37:38 USAD TABLE OF CONTENTS No. Topic Page 1.0 Definition of symbols 5 2.0 Application and functionality 6 2.1 Intended use 6 2.2 Field of application 7 3.0 Safety instructions 7 3.1 General safety instructions 7 3.3 Environment for which the DSO 364 device is not suited 9 3.4 Usage by children and adolescents 10 3.5 Information on the application of the device 10 4.0 Questions concerning body temperature 13 4.1 What is body temperature? 13 4.2 Advantages of measuring the body tempera- ture in the ear 14 4.3 Information on measuring the body tempera- ture in the ear 15 5.0 Scope of delivery / contents 16 6.0 Designation of device parts 17 7.0 LCD display 18 8.0 Basic functions 19 8.1 Commissioning of the device 19 8.2 Warning indicator if the body temperature is 21 too high 2 19.PJN174-14_GA-USA_HHD-Ohrthermometer_DSO364_28.07.14 Montag, 28. Juli 2014 14:37:38 TABLE OF CONTENTS USA No. Topic Page 8.3 Backlighting / torch function 21 8.4 Energy saving mode 22 8.5 Setting °Celsius / °Fahrenheit 22 9.0 Display / setting time and date 23 9.1 Display of time and date 23 9.2 Setting time and date 23 10.0 Memory mode 26 11.0 Measuring the temperature in the ear 28 12.0 Measuring the temperature on the forehead 30 13.0 Object temperature measurement 32 14.0 Disposal of the device 33 15.0 Battery change and information concerning batteries 33 16.0 Cleaning and care 36 17.0 “Cleaning” warning indicator 37 18.0 Calibration 38 19.0 Malfunctions 39 20.0 Technical specification 41 21.0 Warranty 44 3 19.PJN174-14_GA-USA_HHD-Ohrthermometer_DSO364_28.07.14 Montag, 28. -

Tongue -Tie (Ankyloglossia) and Lip -Tie (Lip Adhesion)
Tongue -Tie (Ankyloglossia) and Lip -Tie (Lip Adhesion) What is Tongue-Tie? Most of us think of tongue -tie as a situation we find ourselves in when we are too excited to speak. Actually, tongue- tie is the non medical term for a relatively common physical condition that limits the use of the tongue, ankyloglossia. Lip -tie is a condition where the upper lip cannot be curled or moved normally. Before we are born, a strong cord of tissue that guides development of mouth structures is positioned in the center of the mouth. It is called a frenulum. As we develop, this frenulum recedes and thins. The lingual (tongue) or labial (lip) frenulum is visible and easily felt if you look in the mirror under your tongue and lip. In some children, the frenulum is especially tight or fails to recede and may cause tongue/lip mobility problems. The tongue and lip are a very complex group of muscles and are important for all oral function. For this reason having tongue tie can lead to nursing, eating, dental, or speech problems, which may be serious in some individuals. When Is Tongue and Lip- Tie a Problem That Needs Treatment? Infants A new baby with a too tight tongue and/or lip frenulum can have trouble sucking and may have poor weight gain. If they cannot make a good seal on the nipple, they may swallow air causing gas and stomach problems. Such feeding problems should be discussed with Dr. Sierra. Nursing mothers who experience significant pain while nursing or whose baby has trouble latching on should have their child evaluated for tongue and lip tie. -

Core Strength Exercises
CORE STRENGTH EXERCISES • The main muscles involved with Core Strength include muscles of the abdomen, hip flexors and low back postural muscles. • It is important to maintain proper strength of these muscles to prevent and rehabilitate from low back / pelvic dysfunction and pain. • All of these exercises should be comfortable and not produce pain or discomfort. Bracing: The Key to preventing low back injuries Abdominal Bracing – Lying down • Lie down, face up with your knees bent and feet on floor. • Contract your stomach muscles so that you imagine pushing your low back to the floor or that you are pulling your belly button to your spine. Abdominal Bracing - Standing • Stand up straight and place one hand on the small of the back and one hand on your abdomen. • Bend Forward at the waist and feel the lower back muscles contract (extensors). • Come back up to neutral to relax the low back muscles. • You will feel the low back muscles contract when you contract your abdominal and gluteal muscles. Bracing technique and curling • Lay on the ground on your back. • One leg is bent and the other leg remains flat on the floor. Your hands can be on your chest or at your side. • Fix your eyes on a spot on the ceiling directly above you. • Tighten your stomach muscles. • Holding the stomach contraction, lift your shoulder blades and head off the floor while looking at that spot on the ceiling. Hold for 3-10 seconds and repeat three times. • Switch leg positions and repeat the technique. Beginner to Intermediate position • Position yourself on your hands and knees with your pelvis and thighs at 90 degrees and upper back and arms at 90 degrees. -

Occupational Cancer Risk Series Diesel Engine Exhaust
Occupational Cancer Risk Series Diesel engine exhaust There may be hazards where you work that increase your risk of developing cancer. This factsheet discusses occupational hazards related to diesel engine exhaust (DEE). Key messages • fuel used (e.g. low-sulphur diesel) • use of emission control system/s • In Australia, it is estimated that 1.2 million workers from many jobs are exposed to diesel • state of engine tuning and maintenance engine exhaust (DEE). • pattern of use (load and acceleration) • DEE contains airborne chemicals that are known • length of time the worker is exposed to cause cancer (carcinogens). Effective controls • Eliminate or reduce exposure to carcinogens by All Australian workplaces must follow work health using recommended controls. and safety laws; however these vary slightly • Refer to Safe Work Australia’s Guidance for between states and territories, but the duty of care Managing the Risks of Diesel Exhaust for more for employers and responsibilities of workers across information or contact your state or territory Australia is similar: work health and safety regulator. • Employers are required to ensure the health and Diesel engine exhaust and cancer safety of their workers at their workplace. DEE is created by burning diesel fuels. It contains a • Employers are required to ensure the health and mixture of airborne chemicals that can be harmful safety other people due to the work carried out. to people. When breathed in, these chemicals • Employers have a duty to control the risks increase your risk of developing long-term health associated with work. problems. This includes lung cancer and possibly bladder cancer. -

Anthropometrical Orofacial Measurement in Children from Three to Five Years Old
899 MEDIDAS ANTROPOMÉTRICAS OROFACIAIS EM CRIANÇAS DE TRÊS A CINCO ANOS DE IDADE Anthropometrical orofacial measurement in children from three to five years old Raquel Bossle(1), Mônica Carminatti(1), Bárbara de Lavra-Pinto(1), Renata Franzon (2), Fernando de Borba Araújo (3), Erissandra Gomes(3) RESUMO Objetivo: obter as medidas antropométricas orofaciais em crianças pré-escolares de três a cinco anos e realizar a correlação com idade cronológica, gênero, raça e hábitos orais. Métodos: estudo transversal com 93 crianças selecionadas por meio de amostra de conveniência consecutiva. Os responsáveis responderam a um questionário sobre os hábitos orais e as crianças foram submetidas a uma avaliação odontológica e antropométrica da face. O nível de significância utilizado foi p<0,05. Resultados: as médias das medidas antropométricas orofaciais foram descritas. Houve diferença estatística nas medidas de altura da face (p<0,001), terço médio da face (p<0,001), canto externo do olho até a comissura labial esquerda/direita (p<0,001) e lábio inferior (p=0,015) nas faixas etárias. O gênero masculino apresentou medidas superiores na altura de face (p=0,003), terço inferior da face (p<0,001), lábio superior (p=0,001) e lábio inferior (p<0,001). Não houve diferença estatisticamente significante na altura do lábio superior em sujeitos não brancos (p=0,03). A presença de hábitos orais não influenciou os resultados. O aleitamento materno exclusivo por seis meses influenciou o aumento da medida de terço médio (p=0,022) e da altura da face (p=0,037). Conclusão: as médias descritas neste estudo foram superiores aos padrões encontrados em outros estudos. -

The Complexity and Origins of the Human Eye: a Brief Study on the Anatomy, Physiology, and Origin of the Eye
Running Head: THE COMPLEX HUMAN EYE 1 The Complexity and Origins of the Human Eye: A Brief Study on the Anatomy, Physiology, and Origin of the Eye Evan Sebastian A Senior Thesis submitted in partial fulfillment of the requirements for graduation in the Honors Program Liberty University Spring 2010 THE COMPLEX HUMAN EYE 2 Acceptance of Senior Honors Thesis This Senior Honors Thesis is accepted in partial fulfillment of the requirements for graduation from the Honors Program of Liberty University. ______________________________ David A. Titcomb, PT, DPT Thesis Chair ______________________________ David DeWitt, Ph.D. Committee Member ______________________________ Garth McGibbon, M.S. Committee Member ______________________________ Marilyn Gadomski, Ph.D. Assistant Honors Director ______________________________ Date THE COMPLEX HUMAN EYE 3 Abstract The human eye has been the cause of much controversy in regards to its complexity and how the human eye came to be. Through following and discussing the anatomical and physiological functions of the eye, a better understanding of the argument of origins can be seen. The anatomy of the human eye and its many functions are clearly seen, through its complexity. When observing the intricacy of vision and all of the different aspects and connections, it does seem that the human eye is a miracle, no matter its origins. Major biological functions and processes occurring in the retina show the intensity of the eye’s intricacy. After viewing the eye and reviewing its anatomical and physiological domain, arguments regarding its origins are more clearly seen and understood. Evolutionary theory, in terms of Darwin’s thoughts, theorized fossilization of animals, computer simulations of eye evolution, and new research on supposed prior genes occurring in lower life forms leading to human life. -

10 Facts You Should Know About Occupational Carcinogens
10 facts you should know about occupational carcinogens Carcinogens are the “time bombs” of hazardous substances in the workplace. But many substances do not develop their deadly effect until years after expo- sure. It’s a risk for the worker that is often underestimated – and represents an enormous challenge for industrial hygienists. The good news is that occup- ational cancer can be prevented through monitoring and protective measures. © Drägerwerk AG & Co. KGaA 1 10 FACTS ABOUT OCCUPATIONAL CARCINOGENS 1. Cancer is a major health hazard in the workplace. Cancer in the workplace is twice as common as occupational accidents. Every year, 660,000 deaths occur worldwide due to work-related cancer.1 2. Plastic is a deadly threat. 3. Carcinogens are toxic to cells. For many years, vinyl chloride was considered to be safe. This com- Carcinogenic substances are a subgroup of toxic agents, which have pound of carbon, hydrogen and chlorine is a raw material used in the the potential to cause cancer in living tissues. Carcinogen exposure production of PVC. In 1974, seven cases of severe (and very rare) can occur from the inhalation, ingestion, or absorption of many dif- liver cancer were found in individuals who worked at a PVC plant in ferent types of substances in our bodies. Louisville, Kentucky. Five of the afflicted workers, all of whom had Carcinogens may increase the risk of cancer by altering cellular worked with vinyl chloride for 20 years, had already died.2 metabolism or damaging substances such as proteins, ribonucleic It is only because of the efforts of the National Institute for Occup- acids, and especially DNA directly in cells – which interferes with ational Safety and Health (NIOSH) and the energetic probing of a biological processes.