Situation Analysis of Health Research in Cameroon
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Page 1 C H a D N I G E R N I G E R I a G a B O N CENTRAL AFRICAN
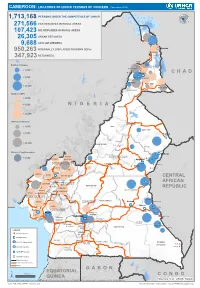
CAMEROON: LOCATIONS OF UNHCR PERSONS OF CONCERN (November 2019) 1,713,168 PERSONS UNDER THE COMPETENCENIGER OF UNHCR 271,566 CAR REFUGEES IN RURAL AREAS 107,423 NIG REFUGEES IN RURAL AREAS 26,305 URBAN REFUGEES 9,688 ASYLUM SEEKERS 950,263 INTERNALLY DISPLACED PERSONS (IDPs) Kousseri LOGONE 347,923 RETURNEES ET CHARI Waza Limani Magdeme Number of refugees EXTRÊME-NORD MAYO SAVA < 3,000 Mora Mokolo Maroua CHAD > 5,000 Minawao DIAMARÉ MAYO TSANAGA MAYO KANI > 20,000 MAYO DANAY MAYO LOUTI Number of IDPs < 2,000 > 5,000 NIGERIA BÉNOUÉ > 20,000 Number of returnees NORD < 2,000 FARO MAYO REY > 5,000 Touboro > 20,000 FARO ET DÉO Beke chantier Ndip Beka VINA Number of asylum seekers Djohong DONGA < 5,000 ADAMAOUA Borgop MENCHUM MANTUNG Meiganga Ngam NORD-OUEST MAYO BANYO DJEREM Alhamdou MBÉRÉ BOYO Gbatoua BUI Kounde MEZAM MANYU MOMO NGO KETUNJIA CENTRAL Bamenda NOUN BAMBOUTOS AFRICAN LEBIALEM OUEST Gado Badzere MIFI MBAM ET KIM MENOUA KOUNG KHI REPUBLIC LOM ET DJEREM KOUPÉ HAUTS PLATEAUX NDIAN MANENGOUBA HAUT NKAM SUD-OUEST NDÉ Timangolo MOUNGO MBAM ET HAUTE SANAGA MEME Bertoua Mbombe Pana INOUBOU CENTRE Batouri NKAM Sandji Mbile Buéa LITTORAL KADEY Douala LEKIÉ MEFOU ET Lolo FAKO AFAMBA YAOUNDE Mbombate Yola SANAGA WOURI NYONG ET MARITIME MFOUMOU MFOUNDI NYONG EST Ngarissingo ET KÉLLÉ MEFOU ET HAUT NYONG AKONO Mboy LEGEND Refugee location NYONG ET SO’O Refugee Camp OCÉAN MVILA UNHCR Representation DJA ET LOBO BOUMBA Bela SUD ET NGOKO Libongo UNHCR Sub-Office VALLÉE DU NTEM UNHCR Field Office UNHCR Field Unit Region boundary Departement boundary Roads GABON EQUATORIAL 100 Km CONGO ± GUINEA The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations Sources: Esri, USGS, NOAA Source: IOM, OCHA, UNHCR – Novembre 2019 Pour plus d’information, veuillez contacter Jean Luc KRAMO ([email protected]). -

Characterisation of Fungi of Stored Common Bean Cultivars Grown in Menoua Division, Cameroon
bioRxiv preprint doi: https://doi.org/10.1101/2020.10.31.363184; this version posted November 1, 2020. The copyright holder has placed this preprint (which was not certified by peer review) in the Public Domain. It is no longer restricted by copyright. Anyone can legally share, reuse, remix, or adapt this material for any purpose without crediting the original authors. CHARACTERISATION OF FUNGI OF STORED COMMON BEAN CULTIVARS GROWN IN MENOUA DIVISION, CAMEROON TEH EXODUS AKWA*1, JOHN M MAINGI1, JONAH K. BIRGEN2 *Corresponding author: TEH EXODUS AKWA 1Department of Biochemistry, Microbiology and Biotechnology, Kenyatta University, Nairobi, Kenya 2Department of Plant Sciences, Kenyatta University, Nairobi, Kenya *Corresponding author: [email protected]; Tel.: +254 792 775729; Medical Microbiology, Department of Biochemistry, Microbiology and Biotechnology, Kenyatta University, Nairobi, Kenya, P.O BOX 43844-00100-NAIROBI 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.10.31.363184; this version posted November 1, 2020. The copyright holder has placed this preprint (which was not certified by peer review) in the Public Domain. It is no longer restricted by copyright. Anyone can legally share, reuse, remix, or adapt this material for any purpose without crediting the original authors. CHARACTERISATION OF FUNGI OF STORED COMMON BEAN CULTIVARS GROWN IN MENOUA DIVISION, CAMEROON. Abstract Common bean is a legume grown globally especially in developing countries including Cameroon for human consumption. In Cameroon it is grown in a wide variety of agro ecological zones in quantities enough to last through the off growing season after harvest. Stored common bean after harvest in Cameroon are prone to fungal spoilage which contributes to post harvest losses. -

Africanprogramme for Onchocerctasts Control (Apoc)
RESERVED FOR PROTECT LOGO/HEADING COUNTRYAIOTF: CAMEROON Proiect Name: CDTI SW 2 Approval vearz 1999 Launchins vegr: 2000 Renortins Period: From: JANUARY 2008 To: DECEMBER 2008 (Month/Year) ( Mont!{eq) Proiectvearofthisrenort: (circleone) I 2 3 4 5 6 7(8) 9 l0 Date submitted: NGDO qartner: "l"""uivFzoog Sightsavers International South West 2 CDTI Project Report 2008 - Year 8. ANNUAL PROJECT TECHNICAL REPORT SUBMITTED TO TECHNICAL CONSULTATTVE COMMITTEE (TCC) DEADLINE FOR SUBMISSION: To APOC Management by 3l January for March TCC meeting To APOC Management by 31 Julv for September TCC meeting AFRICANPROGRAMME FOR ONCHOCERCTASTS CONTROL (APOC) I I RECU LE I S F[,;, ?ur], APOC iDIR ANNUAL I'II().I Ii(]'I"IIICHNICAL REPORT 't'o TECHNICAL CONSU l.',l'A]'tvE CoMMITTEE (TCC) ENDORSEMENT Please confirm you have read this report by signing in the appropriat space. OFFICERS to sign the rePort: Country: CAMEROON National Coordinator Name: Dr. Ntep Marcelline S l) u b Date: . ..?:.+/ c Ail 9ou R Regional Delegate Name: Dr. Chu + C( z z a tu Signature: n rJ ( Date 6t @ RY oF I DE LA NGDO Representative Name: Dr. Oye Joseph E Signature: .... Date:' g 2 JAN. u0g Regional Oncho Coordinator Name: Mr. Ebongo Signature: Date: 51-.12-Z This report has been prepared by Name : Mr. Ebongo Peter Designation:.OPC SWII Signature: *1.- ,l 1l Table of contents Acronyms .v Definitions vi FOLLOW UP ON TCC RECOMMENDATIONS. 7 Executive Summary.. 8 SECTION I : Background information......... 9 1.1. GrrueRruINFoRMATroN.................... 9 1.1.1 Description of the project...... 9 Location..... 9 1. 1. 2. -

Aerial Surveys of Wildlife and Human Activity Across the Bouba N'djida
Aerial Surveys of Wildlife and Human Activity Across the Bouba N’djida - Sena Oura - Benoue - Faro Landscape Northern Cameroon and Southwestern Chad April - May 2015 Paul Elkan, Roger Fotso, Chris Hamley, Soqui Mendiguetti, Paul Bour, Vailia Nguertou Alexandre, Iyah Ndjidda Emmanuel, Mbamba Jean Paul, Emmanuel Vounserbo, Etienne Bemadjim, Hensel Fopa Kueteyem and Kenmoe Georges Aime Wildlife Conservation Society Ministry of Forests and Wildlife (MINFOF) L'Ecole de Faune de Garoua Funded by the Great Elephant Census Paul G. Allen Foundation and WCS SUMMARY The Bouba N’djida - Sena Oura - Benoue - Faro Landscape is located in north Cameroon and extends into southwest Chad. It consists of Bouba N’djida, Sena Oura, Benoue and Faro National Parks, in addition to 25 safari hunting zones. Along with Zakouma NP in Chad and Waza NP in the Far North of Cameroon, the landscape represents one of the most important areas for savanna elephant conservation remaining in Central Africa. Aerial wildlife surveys in the landscape were first undertaken in 1977 by Van Lavieren and Esser (1979) focusing only on Bouba N’djida NP. They documented a population of 232 elephants in the park. After a long period with no systematic aerial surveys across the area, Omondi et al (2008) produced a minimum count of 525 elephants for the entire landscape. This included 450 that were counted in Bouba N’djida NP and its adjacent safari hunting zones. The survey also documented a high richness and abundance of other large mammals in the Bouba N’djida NP area, and to the southeast of Faro NP. In the period since 2010, a number of large-scale elephant poaching incidents have taken place in Bouba N’djida NP. -

Cameroon Watershed
Journal(of(Materials(and(( J. Mater. Environ. Sci., 2018, Volume 9, Issue 11, Page 3094-2104 Environmental(Sciences( ISSN(:(2028;2508( CODEN(:(JMESCN( http://www.jmaterenvironsci.com! Copyright(©(2018,( University(of(Mohammed(Premier(((((( (Oujda(Morocco( A typological study of the physicochemical quality of water in the Menoua- Cameroon watershed Santsa Nguefack Charles Vital1*, Ndjouenkeu Robert1, Ngassoum Martin Benoit2 , 1Laboratory of Food Physicochemistry, Department of Food Science and Nutrition National Advanced School of Agro- Industrial Sciences, University of Ngaoundéré, PO BOX 455,Ngaoundéré, Cameroon. 2Department of Industrial Chemistry and Environment, National Advanced School of Agro-Industrial Sciences, University of Ngaoundéré, PO BOX 455, Ngaoundéré, Cameroon. Received 29 Oct 2017 Abstract Revised 25 Dec 2018 Cameroon, a country in Central Africa with an outlet to the Atlantic Ocean in the Gulf Accepted 28 Dec 2018 of Guinea, holds enormous potentialities of water resources. These resources used for the supply of water for human consumption, etc., would be polluted by the Keywords intensification of anthropogenic activities, of which the most important recorded in the !!physicochemical, Menoua watershedof West Cameroon are agriculture and breeding. The objective of this !!pollution, work was to study the spatiotemporal parameters of the physicochemical quality !!Menoua watershed, parameters (temperature, pH, electrical conductivity, Turbidity, Nitrates, Ortho !!Anthropogenic Phosphates, Sulphates, Chloride, Potassium and Calcium) the Menoua activities, watershedthrough a main Principal Component Analysis (ACP). The results obtained showed that the pH, turbidity and orthophosphate have levels which are in contradiction !!Water for human consumption. with WHO standards. The physicochemical parameters of this water showed significant spatial and seasonal variations, the causes of which probably related to the human activities generating pollutants. -

Dictionnaire Des Villages Du Fako : Village Dictionary of Fako Division
OFFICE DE LA RECHERCHE SCIENTIFIOUE ET TECHNIOUE OUTRE· MER Il REPUBLIQUE UNIE DU CAMEROUN DICTIONNAIRE DES VILLAGES DU FAKO VILLAGE DICTIONARY OF FAKO DIVISION SECTION DE GEOGRAPHIE 1 OFFICE DE LA RECHERCHE SCIm~TIFIQUE REPUBLIQUE UNIE ET TECmUQUE OUTRE-lViER DU CAlvŒROUN UNITED REPUBLIC OF CANEROON CENTRE O.R.S.T.O.N DE YAOUNDE DICTIONNAIRE DES VILLAGES DU FAKO VILLAGE DICTIONARY OF FAKO DIVISION Juillet 1973 July 1973 COPYRIGHT O.R.S.T.O.M 1973 TABLE DES NATIERES CONTENTS i l j l ! :i i ~ Présentation •••••.•.•.....••....•.....•....••••••.••.••••••.. 1 j Introduction ........................................•• 3 '! ) Signification des principaux termes utilisés •.............• 5 î l\lIeaning of the main words used Tableau de la population du département •...••.....•..•.•••• 8 Population of Fako division Département du Fako : éléments de démographie •.•.... ..••.•• 9 Fako division: demographic materials Arrondissements de Muyuka et de Tiko : éléments de . démographie 0 ••••••••••••••••••••••••••••••••••••••• 10 11uyul{a and Tileo sl)..bdivisions:demographic materials Arrondissement de Victoria: éléments de démographie •••.••• 11 Victoria subdivision:demographic materials Les plantations (12/1972) •••••••••••.•••••••••••••••••••••• 12 Plantations (12/1972) Liste des villages par arrondissement, commune et graupement 14 List of villages by subdivision, area council and customary court Signification du code chiffré •..•••...•.•...•.......•.•••.• 18 Neaning of the code number Liste alphabétique des villages ••••••.••••••••.•.•..•••.•.• 19 -

CAMEROON: LOCATIONS of UNHCR PERSONS of CONCERN (January 2021)
CAMEROON: LOCATIONS OF UNHCR PERSONS OF CONCERN (January 2021) ! Maïné-Soroa DIFFA LAC KANEM BARH EL Magaria ZINDER ! PERSONS OF CONCERN GHAZEL e Gashua gu Yob ! 1,960,832 ! omadu K Geidam KATSINA Guri CAR REFUGEES IN! CAMEROON WATER BODY 316,017 HADJER-LAMIS NIG REFUGHEaEdeSji aIN CAMEROON ! YOBE Jakusko 117,826 ! C OTHER NATIONALITIES ha JIGAWA ri 2,466 Kousseri N'Djamena a Kano i ! j e ASYLUM SEEKERS d Maiduguri a LOGONE 7H ,545 Damaturu ET CHARI INTERNALLY DISPLACED PERSOPoNtisSk u(mIDPs) * 1,032,942 ! BORNO C h KANO a r RETURNEES * Waza i 465,757 Waza a g CHARI-BAGUIRMI CAMERuOn ONIAN REFUGEES Limani Magdeme RETURBNED FORM NIGERIA* 18,279 MAYO SAVA ola Gong Mora Number of refugees EXTRÊME-NORD < 10,000 ! Mokolo DIAMARÉ Biu BAUCHI ! Maroua MAYO-KEBBI < 50,000 GOMBE Minawao MAYO EST ! TSANAGA Yagoua Bauchi ! Gombe ! !Mubi Deba MAYO KANI MAYO DANAY > 75000 ! KADUNA Kaele MAYO LOUTI Jos Guider !! Number of IDPs Lo go Lafia Ləre ne N I G E R I A ! ! < 10,000 ADAMAWA ! TANDJILÉ B Yola é n MAYO-KEBBI < 50,000 o u ! BÉNOUÉ é OUEST C H A D PLATEAU Jalingo > 75000 LOGONE NORD OCCIDENTAL ! e u ! Number of returnees en Moundou !Lafia B Poli Tchollire NASSARAWA< 10,000 ! FARO LOGONE MAYO REY < 50,000 ORIENTAL Gondje ! Wukari Amboko ! Touboro TARABA Dosseye !Makurdi Beke Chantier > 75000 Vina FARO ET DÉO Tingere ! Beka Number of asylum seekers BENUE Paoua Ndip ! < 10,000 VINA !Bocaranga Number of refugees returned Borgop OUHAM Djohong < 10,000 Banyo ADAMAOUA OUHAM-PENDÉ ! Nkambe Ngam NORD-OUEST Kounde MENCHUM DJEREM Meiganga DONGA MANTUNG Tibati -

CMR-3W-Cash-Transfer-Partners V3.4
CAMEROON: 3W Operational Presence - Cash Programming [as of December 2016] Organizations working for cash 10 programs in Cameroon Organizations working in Organizations by Cluster Food security 5 International NGO 5 Multi-Sector cash 5 Government 2 Economic Recovery 3 Red Cross & Red /Livelihood 2 Crescent Movement Nutrition 1 UN Agency 1 WASH 1 Number of organizations Multi-Sector Cash by departments 15 5 distinct organizations 9 organizations conducting only emergency programs 1 organizations conducting only regular programs Number of organizations by departments 15 Economic Recovery/Livelihood Food security 3 distinct organizations 5 distinct organizations Number of organizations Number of organizations by department by department 15 15 Nutrition WASH 3 distinct organizations 1 organization Number of organizations Number of organizations by department by department 15 15 Creation: December 2016 Sources: Cash Working group, UNOCHA and NGOs More information: https://www.humanitarianresponse.info/en/operations/cameroon/cash )HHGEDFNRFKDFDPHURRQ#XQRUJ 7KHERXQGDULHVDQGQDPHVVKRZQDQGWKHGHVLJQDWLRQVXVHGRQWKLVPDSGRQRWLPSO\RI̙FLDOHQGRUVHPHQWRUDFFHSWDQFHE\WKH8QLWHG1DWLRQV CAMEROON:CAMEROON: 3W Operational Presence - Cash Programming [as of December 2016] ADAMAOUA FAR NORTH NORTH 4 distinct organizations 9 distinct organizations 1 organization DJEREM DIAMARE FARO MINJEC CRF MINEPAT CRS IRC MAYO-BANYO LOGONE-ET-CHARI MAYO-LOUTI MINEPAT MINEPAT WFP, PLAN CICR MMBERE MAYO-REY PLAN PUI MINEPAT CENTRE MAYO-DANAY 1 organization MINEPAT LITTORAL 1 organization -

Report on the IDB2014 Celebrations in Cameroon
CAMEROON CELEBRATION OF THE INTERNATIONAL DAY FOR BIODIVERSITY Yaounde, Cameroon 14 May 2014 THEME: ISLAND BIODIVERSITY REPORT A cross-section of the exhibition ground including school children and the media Yaounde, 15 May 2014 1 CITATION This document will be cited as MINEPDED 2014. Report on the Celebration of the 2014 International Day for Biodiversity in Cameroon ACKNOWLEDGEMENT The organisation of the 2014 Day for Biodiversity was carried out under the supervision of the Minister of Environment, Protection of Nature and Sustainable Development Mr HELE Pierre and the Minister Delegate Mr. NANA Aboubacar DJALLOH. The contributions of the Organising Committee were highly invaluable for the success of the celebration of the 2014 International Day for Biodiversity. Members were: AKWA Patrick- Secretary General of MINEPDED- Representative of the Minister at the celebration; GALEGA Prudence- National Focal Point for the Convention on Biological Diversity- coordinator of the celebration; WADOU Angele- Sub-Director of Biodiversity and Biosafety, MINEPDED; WAYANG Raphael- Chief of Service for Biodiversity, MINEPDED NFOR Lilian- Environmental Lawyer at the Service of the Technical Adviser No1 of MINEPDED; SHEI Wilson- Project Assistant, ABS; NDIFOR Roland -Representative of IUCN- Cameroon; BANSEKA Hycinth- Representative of Global Water Partnership- Cameroon MBE TAWE Alex- Representative of World Fish Centre- Cameroon 2 TABLE of CONTENT Introduction…………………………………………………………………………………....4 Preparatory activities………………………………………………………………………..5 Media activities………………………………………………………………………………….5 Commemoration of activities…………………………………………………………….6 Exhibition………………………………………………………………………………………....7 Presentation of stands……………………………………………………………………….7 Conclusion…………………………………………………………………………………………12 Photo gallery…………………………………………………………………………………….13 3 INTRODUCTION Cameroon as a member of the 1992 Convention on Biological Diversity joined the international community to celebrate the International Day for Biodiversity 2014 under the theme ‘Island Biodiversity”. -

Assessing Cost Efficiency Among Small Scale Rice Producers in the West Region of Cameroon: a Stochastic Frontier Model Approach
International Journal of Humanities Social Sciences and Education (IJHSSE) Volume 3, Issue 6, June 2016, PP 1-7 ISSN 2349-0373 (Print) & ISSN 2349-0381 (Online) http://dx.doi.org/10.20431/2349-0381.0306001 www.arcjournals.org Assessing Cost Efficiency among Small Scale Rice Producers in the West Region of Cameroon: A Stochastic Frontier Model Approach Djomo, Raoul Fani*1, Ewung, Bethel1, Egbeadumah, Maryanne Odufa2 1Department of Agricultural Economics. University of Agriculture, Makurdi. Benue-State, Nigeria PMB 2373, Makurdi 2Department of Agricultural Economics and Extension, Federal University Wukari, PMB 1020 Wukari. Taraba State, Nigeria *[email protected] Abstract: Local farmers’ techniques and knowledge in rice cultivation being deficient and the aid system and research to support such farmers’ activities likewise insufficient, technological progress and increase in rice production are not yet assured. Therefore, this Study was undertaken to assess cost efficiency among small scale rice farmers in the West Region of Cameroon using stochastic frontier model approach. A purposive, multistage and stratified random sampling technique was used in selecting the respondents. A total of 192 small scale rice farmers were purposively selected from four (4) out of eight divisions. Data were collected using structured questionnaires and interview schedule, administered on the respondents were analyzed using descriptive statistics and stochastic frontier cost functions. The result indicates that the coefficient of cost of labour was found positive and significantly influence cost of production in small scale rice production at 1 percent level of probability, implying that increases in cost of labour by one unit will also increase cost of production in small scale rice farming by the value of it coefficient. -

N I G E R I a C H a D Central African Republic Congo
CAMEROON: LOCATIONS OF UNHCR PERSONS OF CONCERN (September 2020) ! PERSONNES RELEVANT DE Maïné-Soroa !Magaria LA COMPETENCE DU HCR (POCs) Geidam 1,951,731 Gashua ! ! CAR REFUGEES ING CurAi MEROON 306,113 ! LOGONE NIG REFUGEES IN CAMEROON ET CHARI !Hadejia 116,409 Jakusko ! U R B A N R E F U G E E S (CENTRAL AFRICAN REPUBLIC AND 27,173 NIGERIAN REFUGEE LIVING IN URBAN AREA ARE INCLUDED) Kousseri N'Djamena !Kano ASYLUM SEEKERS 9,332 Damaturu Maiduguri Potiskum 1,032,942 INTERNALLY DISPLACED PERSO! NS (IDPs) * RETURNEES * Waza 484,036 Waza Limani Magdeme Number of refugees MAYO SAVA Mora ! < 10,000 EXTRÊME-NORD Mokolo DIAMARÉ Biu < 50,000 ! Maroua ! Minawao MAYO Bauchi TSANAGA Yagoua ! Gom! be Mubi ! MAYO KANI !Deba MAYO DANAY < 75000 Kaele MAYO LOUTI !Jos Guider Number! of IDPs N I G E R I A Lafia !Ləre ! < 10,000 ! Yola < 50,000 ! BÉNOUÉ C H A D Jalingo > 75000 ! NORD Moundou Number of returnees ! !Lafia Poli Tchollire < 10,000 ! FARO MAYO REY < 50,000 Wukari ! ! Touboro !Makurdi Beke Chantier > 75000 FARO ET DÉO Tingere ! Beka Paoua Number of asylum seekers Ndip VINA < 10,000 Bocaranga ! ! Borgop Djohong Banyo ADAMAOUA Kounde NORD-OUEST Nkambe Ngam MENCHUM DJEREM Meiganga DONGA MANTUNG MAYO BANYO Tibati Gbatoua Wum BOYO MBÉRÉ Alhamdou !Bozoum Fundong Kumbo BUI CENTRAL Mbengwi MEZAM Ndop MOMO AFRICAN NGO Bamenda KETUNJIA OUEST MANYU Foumban REPUBLBICaoro BAMBOUTOS ! LEBIALEM Gado Mbouda NOUN Yoko Mamfe Dschang MIFI Bandjoun MBAM ET KIM LOM ET DJEREM Baham MENOUA KOUNG KHI KOUPÉ Bafang MANENGOUBA Bangangte Bangem HAUT NKAM Calabar NDÉ SUD-OUEST -

Evaluating the Constraints and Opportunities of Maize Production in the West Region of Cameroon for Sustainable Development
Journal of Sustainable Development in Africa (Volume 13, No.4, 2011) ISSN: 1520-5509 Clarion University of Pennsylvania, Clarion, Pennsylvania EVALUATING THE CONSTRAINTS AND OPPORTUNITIES OF MAIZE PRODUCTION IN THE WEST REGION OF CAMEROON FOR SUSTAINABLE DEVELOPMENT Godwin Anjeinu Abu1, Raoul Fani Djomo-Choumbou1 and Stephen Adogwu Okpachu2 1. Department of Agricultural Economics, University of Agriculture PMB 2373, Makurdi Benue State- Nigeria 2. Federal College of Education (Technical), Potiskum, Yobe State, Nigeria ABSTRACT A study of Evaluating the constraints and opportunities of Maize production in the West Region of Cameroon was carried out using primary and secondary data collected. One hundred and twenty (120) maize farmers randomly selected from eight (8) villages were interviewed using structured questionnaire. Data from the study were analyzed using descriptive statistics such as frequency distribution, percentages, and inferential statistics such as multiple linear regressions. The study found that most maize farmers in the study area were small scale farmers and are full time farmers, the major maize production constraints was poor access to credit facilities. it was also found any unit increase in the quantity of any of the resources used for maize production will increase maize output by the value of their estimated coefficients respectively , however to raise maize production, the study recommend that financial institutions such as agricultural and community banks should be established in the study area with the simple procedure of securing loans. The relevant government agencies and non- governmental organization should mobilize the maize farmers to form themselves into formidable group so that they can derive maximum benefit of collective union.