The HIV/AIDS Impact on Growth
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
0001S07 Prashant M.Nijasure F 3/302 Rutu Enclave,Opp.Muchal
Effective Membership ID Name Address Contact Numbers from Expiry F 3/302 Rutu MH- Prashant Enclave,Opp.Muchala 9320089329 12/8/2006 12/7/2007 0001S07 M.Nijasure Polytechnic, Ghodbunder Road, Thane (W) 400607 F 3/302 Rutu MH- Enclave,Opp.Muchala Jilpa P.Nijasure 98210 89329 8/12/2006 8/11/2007 0002S07 Polytechnic, Ghodbunder Road, Thane (W) 400607 MH- C-406, Everest Apts., Church Vianney Castelino 9821133029 8/1/2006 7/30/2011 0003C11 Road-Marol, Mumbai MH- 6, Nishant Apts., Nagraj Colony, Kiran Kulkarni +91-0233-2302125/2303460 8/2/2006 8/1/2007 0004S07 Vishrambag, Sangli, 416415 MH- Ravala P.O. Satnoor, Warud, Vasant Futane 07229 238171 / 072143 2871 7/15/2006 7/14/2007 0005S07 Amravati, 444907 MH MH- Jadhav Prakash Bhood B.O., Khanapur Taluk, 02347-249672 8/2/2006 8/1/2007 0006S07 Dhondiram Sangli District, 415309 MH- Rajaram Tukaram Vadiye Raibag B.O., Kadegaon 8/2/2006 8/1/2007 0007S07 Kumbhar Taluk, Sangli District, 415305 Hanamant Village, Vadiye Raibag MH- Popat Subhana B.O., Kadegaon Taluk, Sangli 8/2/2006 8/1/2007 0008S07 Mandale District, 415305 Hanumant Village, Vadiye Raibag MH- Sharad Raghunath B.O., Kadegaon Taluk, Sangli 8/2/2006 8/1/2007 0009S07 Pisal District, 415305 MH- Omkar Mukund Devrashtra S.O., Palus Taluk, 8/2/2006 8/1/2007 0010S07 Vartak Sangli District, 415303 MH MH- Suhas Prabhakar Audumbar B.O., Tasgaon Taluk, 02346-230908, 09960195262 12/11/2007 12/9/2008 0011S07 Patil Sangli District 416303 MH- Vinod Vidyadhar Devrashtra S.O., Palus Taluk, 8/2/2006 8/1/2007 0012S07 Gowande Sangli District, 415303 MH MH- Shishir Madhav Devrashtra S.O., Palus Taluk, 8/2/2006 8/1/2007 0013S07 Govande Sangli District, 415303 MH Patel Pad, Dahanu Road S.O., MH- Mohammed Shahid Dahanu Taluk, Thane District, 11/24/2005 11/23/2006 0014S07 401602 3/4, 1st floor, Sarda Circle, MH- Yash W. -

Animal Rahat's 2015 Annual Review
we supervised population, but for small villages that are not equipped to take the creation on such programmes, Animal Rahat piloted the Animal Birth Financial Statement of India’s Control (ABC) programme. Started in 2014 in Wadji village, first forested this year it expanded to other selected villages throughout captive-elephant Solapur, Sangli and sanctuary at REVENUES Satara that have a Bannerghatta Contributions 34,616,562 large number of stray Biological Park Other Income 1,486,381 dogs. Working with _______________________________________________ (BBP), where the help of village Sunder now lives. panchayats, Animal Total Revenues 36,102,943 © Sreedhar Vijayakrishnan The sanctuary is Rahat veterinarians nearly 50 hectares, visit these villages OPERATING EXPENSES harbouring more than a dozen elephants and allowing them on a routine basis Programmes to roam, swim and socialise in peace. to spay and neuter Community Development dogs. And in a Services & Advocacy 4,202,203 We also assisted PETA India at historic workshops it new strategy that Compassionate Citizen Project 555,611 hosted in Bangalore and Delhi, conducted by international has already been Home for Retired Bullock Expenses 2,586,984 elephant experts Margaret Whittaker and Gail Laule, to successful in one Special Projects 1,217,090 train elephant caregivers from BBP and many central and village in Solapur, we ask community members to contribute Medical Programmes 8,372,874 state government wildlife officials on the principles of financially towards the sterilisation of their animals, which Management and General Expenses 5,817,412 gives the programme more value. We have sterilised all modern, humane protected-contact (PC) management of _______________________________________________ 117 dogs in this village. -
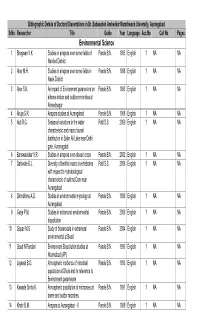
Environmental Science 1 Bhagwan V.K Studies in Airspora Over Some Fields of Pande B.N
Biblographic Details of Doctoral Dissertations in Dr. Babasaheb Ambedkar Marathwada University, Aurangabad SrNo Researcher Title Guide Year Language Acc.No Call No Pages Environmental Science 1 Bhagwan V.K Studies in airspora over some fields of Pande B.N. 1983 English 1 NA NA Nanded District. 2 Aher M.H. Studies in airspora over some fields in Pande B.N. 1998 English 1 NA NA Nasik District 3 Aher S.K. An impact of Environment parameters on Pande B.N. 1993 English 1 NA NA airbone indoor and outdoor microbes at Ahmednagar 4 Ahuja S.R. Airspora studies at Aurangabad Pande B.N. 1988 English 1 NA NA 5 Auti R.G. Seasonal variations in the water Patil S.S. 2009 English 1 NA NA characteristic and macro faunal distribution in Salim Ali Lake near Delhi gate, Auranagabd 6 Banswadekar V.R. Studies in airspora over oilseed crops Pande B.N. 2002 English 1 NA NA 7 Dahiwale B.J. Diversity of benthic macro invertebrates Patil S.S. 2008 English 1 NA NA with respect to hydrobiological characteristic of sukhna Dam near Aurangabad 8 Dhimdhime A.D. Studies in environmental mycology at Pande B.N. 1999 English 1 NA NA Aurangabad 9 Garje P.M. Studies in extramural environmental Pande B.N. 2000 English 1 NA NA biopollution 10 Gopan M.S. Study of bioaerosols in extramural Pande B.N. 2004 English 1 NA NA environmental at Beed 11 Goud N.Pundari Environment Biopollution studies at Pande B.N. 1993 English 1 NA NA Nizamabad (AP) 12 Jayswal B.O. -

Panchayat Samiti Elections in Maharashtra: a Data Analysis (1994-2013)
PANCHAYAT SAMITI ELECTIONS IN MAHARASHTRA: A DATA ANALYSIS (1994-2013) Rajas K. Parchure ManasiV. Phadke Dnyandev C. Talule GOKHALE INSTITUTE OF POLITICS AND ECONOMICS (Deemed to be a University)` Pune (India), 411 001 STUDY TEAM Rajas K. Parchure : Team Leader Manasi V. Phadke : Project Co-ordinator Dnyandev C. Talule Project Co-ordinator Rajesh R. Bhatikar : Editorial Desk Anjali Phadke : Statistical Assistant Ashwini Velankar : Research Assistant Vaishnavi Dande Research Assistant Vilas M. Mankar : Technical Assistance PANCHAYAT SAMITI ELECTIONS IN MAHARASHTRA : A DATA ANALYSIS (1994-2013) 2016 TABLE OF CONTENTS CHAPTER CONTENT PAGE NO. NO. Foreword v Acknowledgements vi 1 A Historical Perspective on Local Governance 1 2 Defining Variables and Research Questions 18 3 Data Analysis: Behaviour of Main Variables 25 Across Different Rounds of Elections 4 Data Analysis: Correlations Between Key 85 Variables 5 Conclusion 86 References Appendix – A Data on VT, POL, SCST and REVERSE COMP 89 Across Rounds of Elections Appendix – B Average Values of VT, POL, RESERVE COMP 105 and IND Appendix – C Cluster Analysis of VT, POL, REVERSE COMP, 124 IND and RES Appendix – D Councils Relevant for Immediate Launch of Voter 144 Awareness Programs Appendix – E Councils Relevant for MCC Implementation 146 Gokhale Institute of Politics and Economics, Pune i PANCHAYAT SAMITI ELECTIONS IN MAHARASHTRA : A DATA ANALYSIS (1994-2013) 2016 LIST OF TABLES Tables Content Page No. No. 3.1 Trends in VT across Successive Rounds of Elections 25 3.2 Panchayat Samitis belonging -
Sangli District COVID
Sangli District COVID - 19 Press Note , Dt.04/08/2020 till 5.00 pm Block Wise Case Reports Todays Total Positive COVID-19 AGE WISE No Block TESTING REPORT Positive Progressive BREAKUP 1 Atpadi 0 145 0 < 1Yr 3 RT- PCR 2 Jath 10 184 1 - 10 Yr 194 Swab Report Received 320 3 Kadegaon 0 76 11 - 20 Yr 330 Swab Report Positive 43 4 K.M. 1 123 21 - 50 Yr 2036 5 Khanapur 0 60 51 - 70 Yr 889 ANTIGEN TESTING 6 Miraj 1 268 > 70 Yr 188 Swab Report Received 0 7 Palus 0 135 Total 3640 Swab Report Positive 0 8 Shirala 0 196 9 Tasgaon 1 93 COVID 19 TOTAL TESTING 10 Walwa 5 150 DISCHARGE Swab Report Received 320 11 SMKC 19 2042 DAILY Progressive Swab Report Positive 43 Out Of State/ 12 6 168 31 1561 Other District Total 43 3640 TOTAL PATIENTS DISCHARGE TILL TODAY 1561 TOTAL DEATHS TILL TODAY 143 TOTAL ACTIVE PATIENT IN THE DISTRICT 1936 COVID-19 DEATH BREAKUP DAILY PROGRESSIVE BLOCK / CORPORATION Total Death 05 143 Atpadi- 02, Jat - 03, Todays Death Kadegaon- 03, K.M.-01, 1 65/M - Kupwad - GMC Miraj Rural Miraj- 12, Palus- 06, 41 2 65/M - Sangliwadi, Sangli - GMC Miraj Shirala- 05, Tasgaon- 02 , 3 80/M - Vishrambag, Sangli - GMC Miraj Walwa- 07 4 55/F - Foujdargalli Sangli - Sangli Civil Jath - 02, Kadegaon - 01, 5 52/M - Govt.Colony Sangli - GMC Miraj Urban K.M. - 02, Tasgaon - 01, 7 Walwa - 01 Sangli - 30, Miraj - 28 SMKC 59 Kupwad - 01 Sangli Total Death 107 Other Kolhapur - 13, Satara - 03, 21 District Ratnagiri - 02, Solapur - 03 Other State Karnataka - 15 15 Other District Total Death 36 District Civil Surgeon, and Incident Cammander COVID Control, -

District-Sangli No.Of Inmates
District-Sangli No.of Inmates In Case of Year of Establishment of the Hostel,no. Nature of management Sr. No. Name of the Institutions & Address Contact Details & E-mail ID Total Present Institution/ Hostel of (Govt.run/aided or Private) Capacity Strength SC/ST/OBC Students 1 vidyarthi vastigrah tadasar 9766657820 24 22 22 Samjkalyan vibhag sangli 2 vitamata vasatigrah devrastre 9096065020 54 34 34 Samjkalyan vibhag sangli 3 Prathamik ashram ashool atpati 02343/220812 May-99 120 120 120 private Krushna Rama Gurav Ashram School 02343/220182 4 Jun-82 120 120 120 private Kharsundi B R Shinde magasvargiy vidhyathi 5 17-Oct 48 48 48 private vastigrah Rajewadi Prerna vidyalaya matimand mulanchi 9970700989 Email ID- 6 nivasi shala vategaon, taluka Walwa prenamatimand 25 25 6 private [email protected] Dr.v.s.nerklekar mukbadhir vidyalay 02342/224485 Email ID- 7 islampur, taluka Walwa [email protected] 75 75 0 Social welfer office ZP sangli m Bharatratna Dr.babasaheb Ambedkar 8530687060 Email ID- matimand mulanchi nivasi shala [email protected] 8 50 40 0 private Koregaon, taluka Walwa Shivsamrth primary Asramshala 9130101000/ 7972017042 Kasegaon, taluka Walwa Email ID- 9 120 120 0 private Aided [email protected] om Prathamik Ashramshala Retharedharan, 02342.257402 Email ID- 10 taluka Walwa [email protected] 120 120 0 private Aided m Prathmik Ashramshala Ashta taluka 02342/241116 Email ID- 11 70 70 78 private Aided Walwa [email protected] Madhyamik Ashramshala Ashta taluka 02342/241116 Email ID- 12 170 170 133 private Aided Walwa [email protected] Magasvargiy mulanche vastigrah Ashta, 02342/241116 Email ID- 13 24 24 20 private Aided taluka Walwa [email protected] prathamik Ashramshala yedenipani, 02342/275048 / 9767679476 taluka Walwa Email ID- 14 120 120 38 private Aided ashramshalayedenipani@gma il.com Bharatratna Dr.babasaheb ambedakar 8530687060 Email ID- asthivyang mulanchi nivasi shala [email protected] 15 30 30 0 private Aided koregaon, taluka Walwa Loknete R.B. -

(II) Basic Information
APPLICATION FOR MINING OF MINOR MINERALS UNDER CATEGORY ‘B2’ FORLESS THAN AND EQUAL TO FIVE HECTARE (II) Basic Information :- 1 Name of the Mining Lease site: M/s. Sou Anuradha Sachin Patil., Gut No-87, Gourgaon, Tal- Tasgaon, Dist- Sangli ,Maharashtra 2 Location / site 17° 10'20.04"N (GPS Co-ordinates): 74° 42' 51.12"E 3 Size of the Mining Lease 1 hector (Hectare): 4 Capacity of Mining Lease (TPA): 38070 T/A average 5 Period of Mining Lease: 5 year 6 Expected cost of the Project: 25 lacks 7 Contact Information: M/s. Sou Anuradha Sachin Patil., Gut No-87, Gourgaon, Tal- Tasgaon, Dist- Sangli, Maharashtra Pre-Feasibility Report (PFR) for Stone Quarry M/s. Sou Anuradha Sachin Patil., Gut No-87, Gourgaon, Tal- Tasgaon, Dist- Sangli Maharashtra Prepared By Mahabal Enviro Engineers Pvt. Ltd. & GMC Engineers & Environmental Services Kolhapur www.gmcenviro.com E-Mail: [email protected], [email protected] Contact: 99211 90356, 8275266011 1.0 Brief Introduction: The M/s. Sou Anuradha Sachin Patil..owner of Gut No-87, Gourgaon, Tal- Tasgaon, Dist- Sangli over a total area of 1 hector. The said land as been converted as non-agriculture for the purpose of small scale industries. Accordingly the quarry plan is prepared along with application form 1, PFR & EMP for the approval. 1 Need for the project: The region is economically backward mostly depends on seasonal forming. The per capita income of the villagers is much below the national average. As a result of this project various facilities like educational medical social benefits will get augmented in the area. -

Sangli District Maharashtra
1803/DBR/2013 भारत सरकार जल संसाधन मंत्रालय कᴂ द्रीय भूजल बो셍ड GOVERNMENT OF INDIA MINISTRY OF WATER RESOURCES CENTRAL GROUND WATER BOARD महाराष्ट्र रा煍य के अंत셍डत सां셍ली जजले की भूजल विज्ञान जानकारी GROUND WATER INFORMATION SANGLI DISTRICT MAHARASHTRA By 饍िारा Abhay Nivasarkar अभय ननिसरकर Scientist-B िैज्ञाननक - ख म鵍य क्षेत्र, ना셍पुर CENTRAL REGION, NAGPUR 2013 SANGLI DISTRICT AT A GLANCE 1. General Information Geographical area 8572 Sq Km Administrative division Shirala, Walwa, Palus, Khanapur, Atpadi, Tasgnon Miraj , Kavathe Mahakal, Jat, AND Khadgaon Villages 724 Population 25,83,524 (Male 13,20,088 , Female12,63,436) Normal rainfall 550 mm 2. Geomorphology Major Physiographic unit Hills and ghat, Foot hill, Pleatodleb, ,Plains 3. Landuse (As on 2010-11) Fprest area 47593 ha Net sownarea 597700 ha Cultivable area 768685ha 4. Soil type Medium black and deep black soil 5. Principal crops (As on 2010-11) Jawar 272765 ha Wheat 30965 ha Ceral 97003 ha Sugarcane 51016 6. Irrigation by different sources (2010-11) Benefited area (ha) Actual Irrigated area (ha) Major irrigation project 84725 82786 Medium irrigation project 15075 6919 Small irrigation project 35614 13486 Dugwell (2010-11) 54064 (nos) 102327Ha Borewell (2010-11) 63 (nos) 7. Ground Water Monitoring Well (As on Jan 2011) Dugwell 36 Piezometer 03 8. Geology Recent Alluvium Upper cretaceous to Eocene Deccan Trap (Basalt) 9. Hydrogeology Water bearing formation Basalt- Wathered /fractured / jointed / vesicular/ massive/ under phreatic ,Semi confined, Confined Minimum (mbgl) Maximum (m.bgl) Pre monsoon depth to water level 0.35 (mbgl) 16.45 (mbgl) Post monsoon water level 0.2 (mbgl) 11.0 (mbgl) Ground water fluctuation 0.15 m 10.28 m Pre monsoon Water level Trend Not any significant decline trend 10. -

Maharashtra Floods: Death Toll in Pune Division Mounts to 56
follow us on reach us on app اردو ਪਜਾਬੀENGLISH ह)ी বাংলা मराठी ુજરાતી ಕನಡ த മലയാളം P* store Home Politics India Opinion Entertainment Tech Auto Buzz VideosAll SectionsCricket Pro Kabaddi LIVE TV Latest Lifestyle Photos Ganesh Chaturthi Immersives Vanity Diaries Lifestyle & Banking Swasth India NEWS18 » INDIA 1-MIN READ Maharashtra Floods: Death Toll in Pune Division Mounts to 56 With most of the rivers in Kolhapur, Sangli and Satara now owing below the danger marks, communication to almost all villages in the region has been restored. PTI Updated:August 18, 2019, 11:01 PM IST A fruit seller sits on a ooded road after monsoon rains in Nala Sopara in Palghar district of Maharashtra, Monday, Aug. 5, 2019. (PTI Photo) close Loading... Mumbai: The death toll in oods in the Pune division of Maharashtra climbed to 56 on Sunday, a senior ocer said. Out of the ve districts that fall under the administrative division, Sangli and Kolhapur were badly affected by oods in the second week of August. Maharashtra Floods: Death Toll in Pune Division Mounts to 56 Mumbai Police Trace and Return Woman's Handbag Containing … Ind Other districts in the division are Solapur, Pune and Satara. With most of the rivers in Kolhapur, Sangli and Satara now owing below the danger marks, communication to almost all villages in the region has been restored. "The death toll in oods in Kolhapur, Sangli, Satara, Solapur and Pune has reached to 56 while two persons are still missing. Most of the deaths have occurred in Kolhapur and Sangli districts, which were worst hit due to oods," said Deepak Mhaisekar, Divisional Commissioner, Pune. -

Current Situation on Maharashtra Floods and Landslides Date: 03-08-2021
Current situation on Maharashtra Floods and Landslides Date: 03-08-2021 Humanitarian Aid International (HAI) is constantly assessing the situation through its local member Dr. Ambedkar Sheti Vikas Va Sanshodhan Sanstha (ASVSS) and techno-humanitarian partner InventGrid. Lifesaving immediate relief assistance to the worst affected people in the districts of Kolhapur, Ratnagiri, and Sangli has also been initiated with the support from Sony Pictures Networks India Private Limited (SPNI), Himalaya Drug Company, and Lung Care Foundation. The current situation is summarized below. Background: Maharashtra witnessed high-intensity floods due to the incessant rains over the past few weeks. At least 209 people have died due to the floods in Maharashtra and eight still remain missing. A total of 4,34,185 people from eight districts have been evacuated to safer places, as rescue operations continue.1Among the 209 fatalities, the Satara district reported 46 deaths, followed by 35 in Ratnagiri, 15 in Thane, seven in Kolhapur, four in Mumbai, three in Pune, four in Sindhudurg and two each in eastern Maharashtra's Wardha and Akola districts. A total of 3,221 animals have died2. Meanwhile, the floodwater has entered the roads and fields, submerging many areas of the Sangli district in Maharashtra making it hard for people to commute from one place to another. According to preliminary estimates, losses to public and private properties are over ₹4,000 crore ($53,88,00,000). Losses due to flooding in Kolhapur and Sangli are ₹700 crore ($94,290,000). Electricity infrastructure worth ₹1,200 crore ($ 16,16,40,000) has been damaged, while damage to roads and bridges is over ₹1,500 crore ($202,050,000). -
SANGLI DISTRICT at a GLANCE M.Phil Project I 2011
n CHAPTER - IV SANGLI DISTRICT AT A GLANCE M.phil Project I 2011 CHAPTER - IV SANGLI DISTRICT AT A GLANCE. 1] GEOGRAPHICAL DETAILS. Sangli district is located in the Western part of Maharashtra. It is bounded by Satara, Solapur Districts to the North and Bijapur district to the East, Kolhapur and Belgaum district to the South and Ratnagiri district to the West. Sangli district is situated in the river basin of the Warna and Krishna River. The physical setting of Sangli district show a contrast of immense dimension and reveals a variety of landscapes influenced by relief, climate and vegetation. The climate ranges from the rainiest in the Chandoli (Shirala) region, which has an average annual all of over 4000 mm to the driest in Atpadi and Jath Tehsils where the average annual rainfall is about 500 mm. The vegetal covers too vary from the typical monsoon forest in the western part to scrub and poor grass in the eastern parts. 2. HISTORY OF SANGLI. The district is named after the district headquarters- Sangli. The Mauryas, the Satvahanas, the Pandavas, the Chalukyas, the Rhstrakulas, the Silaharas, the Bahamanis, the Adil Shahis and Maratha ruled this religion. The Patwardhans, Bramhin general of the Marathas, took over as the rules of the region in the late - 18th century. In 1818 with the defeat of the Marathas at the Hands if the British, Sangli became part of the British dominions. In 1948 it was merged with Indian Union, and in 1949 the southern part of Satara became present - day Sangli district. In 1956, the district was merged with the Bombay state and in 1960 became a district in the new state of Maharashtra and was renamed Sangli. -

A NOTE on CLIMATE CHANGE ANALYSIS USING GEOSPATIAL TECHNOLOGY in WEST CENTRAL INDIA (CASE STUDY) Sreenivasa Rao Guntupalli1, Prof
International Journal of Science, Environment ISSN 2278-3687 (O) and Technology, Vol. 9, No 4, 2020, 586 – 598 2277-663X (P) A NOTE ON CLIMATE CHANGE ANALYSIS USING GEOSPATIAL TECHNOLOGY IN WEST CENTRAL INDIA (CASE STUDY) Sreenivasa Rao Guntupalli1, Prof. Dr. P.V.V. Prasada Rao2, Dr. C.S. Jha3 and Dr. Indal KRamteke4 1,4Scientific Associate, Maharashtra Remote Sensing Applications Centre, VNIT Campus, Nagpur 2Professor and Head of the Department, Department of Environmental Science, Andhra University, Visakhapatnam 3Associate Head and CGM, National Remote Sensing Centre, ISRO, Hyderabad, India. E-mails: [email protected]; [email protected]; [email protected]; [email protected] Abstract: We know that in west central India Climatic spatio-temporal variations are affecting agricultural production. In this paper Sangli district of Maharashtra has been taken as a case study area during the period 1979 to 2013 (35 years). The result shows that, decadal variations in annual precipitation; the number of rainy days gradually decreased, while precipitation intensity and extreme precipitation days and extreme rainfall intensity remained relatively stable. The annual precipitation intensity trends are consistent, whereas overall average temperature also increased. Due to variations in the precipitation values during the period, different dry spell area were observed at different time scales exhibited in 35 years. Keywords: Annual rainfall, Potential Evapotranspiration, Geospatial techniques, agricultural production. Introduction Drought is one of the main natural causes of agricultural, economic, and environmental damage Burton, I. R. W. Kates, and G. F. White [1]. It is very difficult to observe their characteristics in terms of intensity, magnitude, duration, and spatial extent Sergio et al [12].