Differential Methylation of G-Protein Coupled Receptor Signaling Genes In
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Supplementary Table 1: Adhesion Genes Data Set
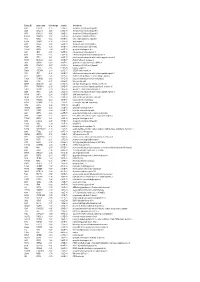
Supplementary Table 1: Adhesion genes data set PROBE Entrez Gene ID Celera Gene ID Gene_Symbol Gene_Name 160832 1 hCG201364.3 A1BG alpha-1-B glycoprotein 223658 1 hCG201364.3 A1BG alpha-1-B glycoprotein 212988 102 hCG40040.3 ADAM10 ADAM metallopeptidase domain 10 133411 4185 hCG28232.2 ADAM11 ADAM metallopeptidase domain 11 110695 8038 hCG40937.4 ADAM12 ADAM metallopeptidase domain 12 (meltrin alpha) 195222 8038 hCG40937.4 ADAM12 ADAM metallopeptidase domain 12 (meltrin alpha) 165344 8751 hCG20021.3 ADAM15 ADAM metallopeptidase domain 15 (metargidin) 189065 6868 null ADAM17 ADAM metallopeptidase domain 17 (tumor necrosis factor, alpha, converting enzyme) 108119 8728 hCG15398.4 ADAM19 ADAM metallopeptidase domain 19 (meltrin beta) 117763 8748 hCG20675.3 ADAM20 ADAM metallopeptidase domain 20 126448 8747 hCG1785634.2 ADAM21 ADAM metallopeptidase domain 21 208981 8747 hCG1785634.2|hCG2042897 ADAM21 ADAM metallopeptidase domain 21 180903 53616 hCG17212.4 ADAM22 ADAM metallopeptidase domain 22 177272 8745 hCG1811623.1 ADAM23 ADAM metallopeptidase domain 23 102384 10863 hCG1818505.1 ADAM28 ADAM metallopeptidase domain 28 119968 11086 hCG1786734.2 ADAM29 ADAM metallopeptidase domain 29 205542 11085 hCG1997196.1 ADAM30 ADAM metallopeptidase domain 30 148417 80332 hCG39255.4 ADAM33 ADAM metallopeptidase domain 33 140492 8756 hCG1789002.2 ADAM7 ADAM metallopeptidase domain 7 122603 101 hCG1816947.1 ADAM8 ADAM metallopeptidase domain 8 183965 8754 hCG1996391 ADAM9 ADAM metallopeptidase domain 9 (meltrin gamma) 129974 27299 hCG15447.3 ADAMDEC1 ADAM-like, -

Human Stem Cell Models Identify Targets of Healthy
HUMAN STEM CELL MODELS IDENTIFY TARGETS OF HEALTHY AND MALIGNANT HEMATOPOIETIC REGULATION BY JENNIFER C REID, BSc A Thesis Submitted to the School of Graduate Studies In Partial Fulfillment of the Requirements For the Degree Doctor of Philosophy McMaster University ÓCopyright by Jennifer C Reid, April 2020 JC Reid <- PhD Thesis ❖ McMaster University $ Biochemistry Descriptive Note McMaster University BACHELOR OF SCIENCE (2015) Hamilton, Ontario (Biomedical Research Specialization, Co-op) Title: Use of human stem cell models to identify targets of healthy and malignant hematopoietic regulation Author: Jennifer C. Reid Supervisor: Dr. Mickie Bhatia Number of pages: xii, 163 ii JC Reid <- PhD Thesis ❖ McMaster University $ Biochemistry AbstrAct Hematopoiesis is the highly regenerative process of producing billions of blood cells each day, including white blood cells, red blood cells, and platelets. Given the relatively short life span of these mature cells, hematopoiesis is dependent on stem and progenitor cells to generate renewed progeny, which represents a tightly regulated process. This includes cell intrinsic and external factors, and where dysregulation can lead to anemia and cancer. As such, the hematopoietic hierarchy has been intensely studied for nearly a century and represents a gold standard model of cell fate and developmental biology, in research and clinical applications. Cellular models, such as in vitro culture and human-mouse xenografts in vivo, have been developed to explain complex phenomena pertaining to hematopoiesis and also interrogate processes which are too invasive to study in humans. Hematopoietic generation is required beyond sustaining homeostasis, and progenitors can be damaged through cytotoxic injuries such as radiation and standard chemotherapy, and also undergo leukemic transformation. -
Entrez ID Gene Name Fold Change Q-Value Description
Entrez ID gene name fold change q-value description 4283 CXCL9 -7.25 5.28E-05 chemokine (C-X-C motif) ligand 9 3627 CXCL10 -6.88 6.58E-05 chemokine (C-X-C motif) ligand 10 6373 CXCL11 -5.65 3.69E-04 chemokine (C-X-C motif) ligand 11 405753 DUOXA2 -3.97 3.05E-06 dual oxidase maturation factor 2 4843 NOS2 -3.62 5.43E-03 nitric oxide synthase 2, inducible 50506 DUOX2 -3.24 5.01E-06 dual oxidase 2 6355 CCL8 -3.07 3.67E-03 chemokine (C-C motif) ligand 8 10964 IFI44L -3.06 4.43E-04 interferon-induced protein 44-like 115362 GBP5 -2.94 6.83E-04 guanylate binding protein 5 3620 IDO1 -2.91 5.65E-06 indoleamine 2,3-dioxygenase 1 8519 IFITM1 -2.67 5.65E-06 interferon induced transmembrane protein 1 3433 IFIT2 -2.61 2.28E-03 interferon-induced protein with tetratricopeptide repeats 2 54898 ELOVL2 -2.61 4.38E-07 ELOVL fatty acid elongase 2 2892 GRIA3 -2.60 3.06E-05 glutamate receptor, ionotropic, AMPA 3 6376 CX3CL1 -2.57 4.43E-04 chemokine (C-X3-C motif) ligand 1 7098 TLR3 -2.55 5.76E-06 toll-like receptor 3 79689 STEAP4 -2.50 8.35E-05 STEAP family member 4 3434 IFIT1 -2.48 2.64E-03 interferon-induced protein with tetratricopeptide repeats 1 4321 MMP12 -2.45 2.30E-04 matrix metallopeptidase 12 (macrophage elastase) 10826 FAXDC2 -2.42 5.01E-06 fatty acid hydroxylase domain containing 2 8626 TP63 -2.41 2.02E-05 tumor protein p63 64577 ALDH8A1 -2.41 6.05E-06 aldehyde dehydrogenase 8 family, member A1 8740 TNFSF14 -2.40 6.35E-05 tumor necrosis factor (ligand) superfamily, member 14 10417 SPON2 -2.39 2.46E-06 spondin 2, extracellular matrix protein 3437 -

ONLINE SUPPLEMENTARY CEACAM3 Decreases Asthma Exacerbations and Modulates Respiratory Syncytial Virus Latent Infection in Childr
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any reliance Supplemental material placed on this supplemental material which has been supplied by the author(s) Thorax ONLINE SUPPLEMENTARY CEACAM3 Decreases Asthma Exacerbations and Modulates Respiratory Syncytial Virus Latent Infection in Children Ching-Hui Tsai, MS1,2, Ann Chen Wu, MD, MPH3, Bor-Luen Chiang, MD, PhD4, Yao-Hsu Yang, MD, PhD4, Shih-Pin Hung, MD5, Ming-Wei Su, PhD1,Ya-Jen Chang, PhD1, Yungling L. Lee, MD, PhD1 1 Institute of Biomedical Sciences, Academia Sinica, Taipei, Taiwan 2 Institute of Epidemiology and Preventive Medicine, National Taiwan University, Taipei, Taiwan 3 Center for Healthcare Research in Pediatrics (CHeRP), PRecisiOn Medicine Translational Research (PROMoTeR) Center, Department of Population Medicine, Harvard Pilgrim Health Care Institute and Harvard Medical School, Boston, Massachusetts 4 Department of Pediatrics, National Taiwan University Hospital, Taipei, Taiwan 5 Department of Pediatrics, Cathay General Hospital, Taiwan Correspondence to: Yungling Leo Lee, MD, PhD, Institute of Biomedical Sciences, Academia Sinica, Taipei 115, Taiwan. E-mail: [email protected]; Tel: 886-2-2652-3013. Tsai C-H, et al. Thorax 2020; 75:725–734. doi: 10.1136/thoraxjnl-2019-214132 BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any reliance Supplemental material placed on this supplemental material which has been supplied by the author(s) Thorax ONLINE SUPPLEMENTARY SUPPLEMENTARY MATERIALS AND METHODS Meta-analysis of RSV-related genes The Gene Expression Omnibus (GEO, https://www.ncbi.nlm.nih.gov/geo/) was searched for RSV-related genes using the search terms “RSV” and “blood”, and five gene expression studies were identified. -

VNN2 Conjugated Antibody
Product Datasheet VNN2 Conjugated Antibody Catalog No: #C31458 Package Size: #C31458-AF350 100ul #C31458-AF405 100ul #C31458-AF488 100ul Orders: [email protected] Support: [email protected] #C31458-AF555 100ul #C31458-AF594 100ul #C31458-AF647 100ul #C31458-AF680 100ul #C31458-AF750 100ul #C31458-Biotin 100ul Description Product Name VNN2 Conjugated Antibody Host Species Rabbit Clonality Polyclonal Isotype IgG Purification Affinity purification Applications most applications Species Reactivity Hu,Ms,Rt Immunogen Description Recombinant fusion protein of human VNN2 (NP_004656.2). Conjugates Biotin AF350 AF405 AF488 AF555 AF594 AF647 AF680 AF750 Other Names VNN2; FOAP-4; GPI-80; vanin 2 Accession No. Swiss-Prot#:O95498NCBI Gene ID:8875 Calculated MW 33kDa Formulation 0.01M Sodium Phosphate, 0.25M NaCl, pH 7.6, 5mg/ml Bovine Serum Albumin, 0.02% Sodium Azide Storage Store at 4°C in dark for 6 months Application Details Suggested Dilution: AF350 conjugated: most applications: 1: 50 - 1: 250 AF405 conjugated: most applications: 1: 50 - 1: 250 AF488 conjugated: most applications: 1: 50 - 1: 250 AF555 conjugated: most applications: 1: 50 - 1: 250 AF594 conjugated: most applications: 1: 50 - 1: 250 AF647 conjugated: most applications: 1: 50 - 1: 250 AF680 conjugated: most applications: 1: 50 - 1: 250 AF750 conjugated: most applications: 1: 50 - 1: 250 Biotin conjugated: working with enzyme-conjugated streptavidin, most applications: 1: 50 - 1: 1,000 Background This gene product is a member of the Vanin family of proteins that share extensive sequence similarity with each other, and also with biotinidase. The family includes secreted and membrane-associated proteins, a few of which have been reported to participate in hematopoietic cell trafficking. -

Modeling and Analysis of Acute Leukemia Using Human Hematopoietic Stem and Progenitor Cells
Modeling and analysis of acute leukemia using human hematopoietic stem and progenitor cells A dissertation submitted to the Graduate School of the University of Cincinnati in partial fulfillment of the requirement for the degree of Doctor of Philosophy in the Molecular &Developmental Biology Graduate Program of the College of Medicine by Shan Lin BS, Tsinghua University, 2009 Dissertation Committee: James C. Mulloy, PhD (Chair) Geraldine Guasch, PhD Ashish R. Kumar, MD, PhD Daniel T. Starczynowski, PhD Yi Zheng, PhD Abstract For decades, elegant mouse models have yielded important insights into the complex biology of acute leukemia development. However, species differences between human and mouse could have significant influences on biological and translational applications. Therefore, human primary hematopoietic cells and xenograft mouse models have become important research tools in the field. In this report, we briefly review the methodologies that use human primary hematopoietic cells to model acute leukemia and examine the effects of leukemic oncogenes. The advantages and limitations of the human model system compared to syngeneic mouse models are discussed. The species-related complexity in human disease modeling is highlighted in the study establishing a faithful model of proB-ALL caused by MLL-AF4, the fusion product of the t(4;11). MLL-AF4 proB-ALL has poor prognosis, the lack of an accurate model hampers the study of disease pathobiology and therapeutic testing. We find human AF4 cDNA inhibits retroviral production and efficient transduction, this limitation can be overcome by fusing MLL with murine Af4, highly conserved with human AF4. Whereas MLL-Af4-transduced murine cells induce only AML, transduced human CD34+ cells produce proB-ALL faithful to t(4;11) disease, fully recapitulating the immunophenotypic and molecular aspects of the disease. -

Transcriptional Profile of Human Anti-Inflamatory Macrophages Under Homeostatic, Activating and Pathological Conditions
UNIVERSIDAD COMPLUTENSE DE MADRID FACULTAD DE CIENCIAS QUÍMICAS Departamento de Bioquímica y Biología Molecular I TESIS DOCTORAL Transcriptional profile of human anti-inflamatory macrophages under homeostatic, activating and pathological conditions Perfil transcripcional de macrófagos antiinflamatorios humanos en condiciones de homeostasis, activación y patológicas MEMORIA PARA OPTAR AL GRADO DE DOCTOR PRESENTADA POR Víctor Delgado Cuevas Directores María Marta Escribese Alonso Ángel Luís Corbí López Madrid, 2017 © Víctor Delgado Cuevas, 2016 Universidad Complutense de Madrid Facultad de Ciencias Químicas Dpto. de Bioquímica y Biología Molecular I TRANSCRIPTIONAL PROFILE OF HUMAN ANTI-INFLAMMATORY MACROPHAGES UNDER HOMEOSTATIC, ACTIVATING AND PATHOLOGICAL CONDITIONS Perfil transcripcional de macrófagos antiinflamatorios humanos en condiciones de homeostasis, activación y patológicas. Víctor Delgado Cuevas Tesis Doctoral Madrid 2016 Universidad Complutense de Madrid Facultad de Ciencias Químicas Dpto. de Bioquímica y Biología Molecular I TRANSCRIPTIONAL PROFILE OF HUMAN ANTI-INFLAMMATORY MACROPHAGES UNDER HOMEOSTATIC, ACTIVATING AND PATHOLOGICAL CONDITIONS Perfil transcripcional de macrófagos antiinflamatorios humanos en condiciones de homeostasis, activación y patológicas. Este trabajo ha sido realizado por Víctor Delgado Cuevas para optar al grado de Doctor en el Centro de Investigaciones Biológicas de Madrid (CSIC), bajo la dirección de la Dra. María Marta Escribese Alonso y el Dr. Ángel Luís Corbí López Fdo. Dra. María Marta Escribese -
Single-Cell Transcriptome and Antigen-Immunoglobin Analysis
Chen et al. Genome Biology (2020) 21:152 https://doi.org/10.1186/s13059-020-02064-6 RESEARCH Open Access Single-cell transcriptome and antigen- immunoglobin analysis reveals the diversity of B cells in non-small cell lung cancer Jian Chen1†, Yun Tan2†, Fenghuan Sun1†, Likun Hou3†, Chi Zhang4, Tao Ge1, Huansha Yu5, Chunxiao Wu6, Yuming Zhu1, Liang Duan1, Liang Wu1, Nan Song1, Liping Zhang3, Wei Zhang3, Di Wang3, Chang Chen1, Chunyan Wu3*, Gening Jiang1* and Peng Zhang1* * Correspondence: wuchunyan581@ 163.com; [email protected]; Abstract [email protected] †Jian Chen, Yun Tan, Fenghuan Sun Background: Malignant transformation and progression of cancer are driven by the co- and Likun Hou contributed equally evolution of cancer cells and their dysregulated tumor microenvironment (TME). Recent to this work. studies on immunotherapy demonstrate the efficacy in reverting the anti-tumoral 3Department of Pathology, Shanghai Pulmonary Hospital, function of T cells, highlighting the therapeutic potential in targeting certain cell types in Tongji University School of TME. However, the functions of other immune cell types remain largely unexplored. Medicine, Shanghai 200433, China 1Department of Thoracic Surgery, Results: We conduct a single-cell RNA-seq analysis of cells isolated from tumor tissue Shanghai Pulmonary Hospital, samples of non-small cell lung cancer (NSCLC) patients, and identify subtypes of tumor- Tongji University School of infiltrated B cells and their diverse functions in the progression of NSCLC. Flow cytometry Medicine, Shanghai 200433, China Full list of author information is and immunohistochemistry experiments on two independent cohorts confirm the co- available at the end of the article existence of the two major subtypes of B cells, namely the naïve-like and plasma-like B cells. -

And Tetranucleotide Short Tandem Repeats N
Nazaripanah et al. Human Genomics (2018) 12:17 https://doi.org/10.1186/s40246-018-0149-3 PRIMARYRESEARCH Open Access Genome-scale portrait and evolutionary significance of human-specific core promoter tri- and tetranucleotide short tandem repeats N. Nazaripanah1, F. Adelirad1, A. Delbari1, R. Sahaf1, T. Abbasi-Asl2 and M. Ohadi1* Abstract Background: While there is an ongoing trend to identify single nucleotide substitutions (SNSs) that are linked to inter/intra-species differences and disease phenotypes, short tandem repeats (STRs)/microsatellites may be of equal (if not more) importance in the above processes. Genes that contain STRs in their promoters have higher expression divergence compared to genes with fixed or no STRs in the gene promoters. In line with the above, recent reports indicate a role of repetitive sequences in the rise of young transcription start sites (TSSs) in human evolution. Results: Following a comparative genomics study of all human protein-coding genes annotated in the GeneCards database, here we provide a genome-scale portrait of human-specific short- and medium-size (≥ 3-repeats) tri- and tetranucleotide STRs and STR motifs in the critical core promoter region between − 120 and + 1 to the TSS and evidence of skewing of this compartment in reference to the STRs that are not human-specific (Levene’s test p <0. 001). Twenty-five percent and 26% enrichment of human-specific transcripts was detected in the tri and tetra human-specific compartments (mid-p < 0.00002 and mid-p < 0.002, respectively). Conclusion: Our findings provide the first evidence of genome-scale skewing of STRs at a specific region of the human genome and a link between a number of these STRs and TSS selection/transcript specificity. -
VNN2 Antibody Cat
VNN2 Antibody Cat. No.: 23-444 VNN2 Antibody Specifications HOST SPECIES: Rabbit SPECIES REACTIVITY: Human, Mouse, Rat Recombinant fusion protein containing a sequence corresponding to amino acids 270-493 IMMUNOGEN: of human VNN2 (NP_004656.2). TESTED APPLICATIONS: WB APPLICATIONS: WB: ,1:500 - 1:2000 POSITIVE CONTROL: 1) Raji 2) Mouse brain 3) Rat brain PREDICTED MOLECULAR Observed: 33kDa WEIGHT: Properties PURIFICATION: Affinity purification CLONALITY: Polyclonal ISOTYPE: IgG September 23, 2021 1 https://www.prosci-inc.com/vnn2-antibody-23-444.html CONJUGATE: Unconjugated PHYSICAL STATE: Liquid BUFFER: PBS with 0.02% sodium azide, 50% glycerol, pH7.3. STORAGE CONDITIONS: Store at -20˚C. Avoid freeze / thaw cycles. Additional Info OFFICIAL SYMBOL: VNN2 FOAP-4, GPI-8vascular non-inflammatory molecule 2, Vannin 2, glycosylphosphatidyl ALTERNATE NAMES: inositol-anchored protein GPI-8pantetheinase GENE ID: 8875 USER NOTE: Optimal dilutions for each application to be determined by the researcher. Background and References This gene product is a member of the Vanin family of proteins that share extensive sequence similarity with each other, and also with biotinidase. The family includes secreted and membrane-associated proteins, a few of which have been reported to participate in hematopoietic cell trafficking. No biotinidase activity has been demonstrated for any of the vanin proteins, however, they possess pantetheinase activity, BACKGROUND: which may play a role in oxidative-stress response. The encoded protein is a GPI- anchored cell surface molecule that plays a role in transendothelial migration of neutrophils. This gene lies in close proximity to, and in same transcriptional orientation as two other vanin genes on chromosome 6q23-q24. -
S41467-018-05357-4.Pdf
ARTICLE DOI: 10.1038/s41467-018-05357-4 OPEN Metaproteomics reveals associations between microbiome and intestinal extracellular vesicle proteins in pediatric inflammatory bowel disease Xu Zhang 1, Shelley A. Deeke1, Zhibin Ning1, Amanda E. Starr1, James Butcher1, Jennifer Li1, Janice Mayne1, Kai Cheng1, Bo Liao1, Leyuan Li1, Ruth Singleton2, David Mack2, Alain Stintzi1 & Daniel Figeys1,3,4 fl 1234567890():,; Alterations in gut microbiota have been implicated in the pathogenesis of in ammatory bowel disease (IBD), however factors that mediate the host–microbiota interactions remain largely unknown. Here we collected mucosal-luminal interface samples from a pediatric IBD inception cohort and characterized both the human and microbiota proteins using meta- proteomics. We show that microbial proteins related to oxidative stress responses are upregulated in IBD cases compared to controls. In particular, we demonstrate that the expression of human proteins related to oxidative antimicrobial activities is increased in IBD cases and correlates with the alteration of microbial functions. Additionally, we reveal that many of these human proteins are present and show altered abundance in isolated free extracellular vesicles (EVs). Therefore, our study suggests that the alteration of intestinal EV proteomes is associated with the aberrant host–microbiota interactions in IBD. 1 Ottawa Institute of Systems Biology and Department of Biochemistry, Microbiology and Immunology, Faculty of Medicine, University of Ottawa, 451 Smyth Road, Ottawa, ON K1H 8M5, Canada. 2 Department of Paediatrics, Faculty of Medicine, University of Ottawa and Children’s Hospital of Eastern Ontario Inflammatory Bowel Disease Centre and Research Institute, 401 Smyth Road, Ottawa, ON K1H 8L1, Canada. 3 Department of Chemistry and Biomolecular Sciences, University of Ottawa, 10 Marie Curie, Ottawa, ON K1N 6N5, Canada. -
Lncrna DRAIR Is Downregulated in Diabetic Monocytes and Modulates Inflammatory Phenotype Via Epigenetic Mechanisms
Supplementary Material LncRNA DRAIR is downregulated in diabetic monocytes and modulates inflammatory phenotype via epigenetic mechanisms Marpadga A. Reddy, Vishnu Amaram, Sadhan Das, Vinay Singh Tanwar, Rituparna Ganguly, Mei Wang, Linda Lanting, Lingxiao Zhang, Maryam Abdollahi, Zhuo Chen, Xiwei Wu, Sridevi Devaraj and Rama Natarajan Supplementary Figure. 1. (A) RNA-seq data showing inflammatory genes upregulated in monocytes from humans with type 2 diabetes versus controls. (B-C) Bubble plots depicting GO Processes enriched in upregulated and downregulated genes. Bubble color represents significance (p-values), and bubble size indicates gene count. (D-E) IPA analysis showing Diseases & Functions enriched in upregulated (D) and downregulated genes (E). (F) IPA analysis showing Canonical pathways enriched in upregulated genes. (G) IPA analysis showing 2 Overlapping Canonical pathways in downregulated genes. Numbers indicate common genes in overlapping networks. SLE: Systemic Lupus Erythematosus. In panels D and F, y-axis represents –log(p-values) from Fisher’s exact test. In panel E, y-axis shows Z-score, where 2 is set as threshold. 3 Supplementary Figure. 2. (A-B) GO Biological processes enriched among differentially expressed gene (DEG)s located nearby the downregulated (A) and upregulated (B) lncRNAs in T2D. DEGs nearby differentially expressed lncRNAs ( 250 kb) in T2D were analyzed using the web-based gene list enrichment analysis tool Enrichr (1-2). 4 Supplementary Figure 3. Characterization of DRAIR coding potential. (A) The Raw PhyloCSF tracks of DRAIR genomic regions, showing the PhyloCSF score of less than zero in all six reading frames, predicting that DRAIR lacks coding potential. In addition, Coding Potential Calculator 2 (CPC2) software (3) also predicted that DRAIR lacks coding potential (coding probability 0.0302545).