Suicidality and Older Adults
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

{PDF EPUB} Invisible Girl the Suicide Journal by Daphine Glenn Robinson Invisible Girl: the Suicide Journal by Daphine Glenn Robinson
Read Ebook {PDF EPUB} Invisible Girl The Suicide Journal by Daphine Glenn Robinson Invisible Girl: The Suicide Journal by Daphine Glenn Robinson. Completing the CAPTCHA proves you are a human and gives you temporary access to the web property. What can I do to prevent this in the future? If you are on a personal connection, like at home, you can run an anti-virus scan on your device to make sure it is not infected with malware. If you are at an office or shared network, you can ask the network administrator to run a scan across the network looking for misconfigured or infected devices. Another way to prevent getting this page in the future is to use Privacy Pass. You may need to download version 2.0 now from the Chrome Web Store. Cloudflare Ray ID: 660ef95f6a614abd • Your IP : 116.202.236.252 • Performance & security by Cloudflare. Kf8 Download. Read or Download Invisible Girl: The Suicide Journal Book by Daphine Glenn Robinson. It is one of the best seller books in this month. Avaliable format in PDF, EPUB, MOBI, KINDLE, E-BOOK and AUDIOBOOK. Invisible Girl: The Suicide Journal by Daphine Glenn Robinson. Category: eBooks Binding: Kindle Edition Author: Daphine Glenn Robinson Number of Pages: 52 Amazon.com Price : $0.99 Lowest Price : $5.25 Total Offers : 1 Rating: 5.0 Total Reviews: 10. Invisible Girl: The Suicide Journal is most popular ebook you need. You can read any ebooks you wanted like Invisible Girl: The Suicide Journal in simple step and you can download it now. Nice ebook you want to read is Invisible Girl: The Suicide Journal. -
![Inmedia, 3 | 2013, « Cinema and Marketing » [Online], Online Since 22 April 2013, Connection on 22 September 2020](https://docslib.b-cdn.net/cover/3954/inmedia-3-2013-%C2%AB-cinema-and-marketing-%C2%BB-online-online-since-22-april-2013-connection-on-22-september-2020-603954.webp)
Inmedia, 3 | 2013, « Cinema and Marketing » [Online], Online Since 22 April 2013, Connection on 22 September 2020
InMedia The French Journal of Media Studies 3 | 2013 Cinema and Marketing Electronic version URL: http://journals.openedition.org/inmedia/524 DOI: 10.4000/inmedia.524 ISSN: 2259-4728 Publisher Center for Research on the English-Speaking World (CREW) Electronic reference InMedia, 3 | 2013, « Cinema and Marketing » [Online], Online since 22 April 2013, connection on 22 September 2020. URL : http://journals.openedition.org/inmedia/524 ; DOI : https://doi.org/10.4000/ inmedia.524 This text was automatically generated on 22 September 2020. © InMedia 1 TABLE OF CONTENTS Cinema and Marketing When Cultural Demands Meet Industrial Practices Cinema and Marketing: When Cultural Demands Meet Industrial Practices Nathalie Dupont and Joël Augros Jerry Pickman: “The Picture Worked.” Reminiscences of a Hollywood publicist Sheldon Hall “To prevent the present heat from dissipating”: Stanley Kubrick and the Marketing of Dr. Strangelove (1964) Peter Krämer Targeting American Women: Movie Marketing, Genre History, and the Hollywood Women- in-Danger Film Richard Nowell Marketing Films to the American Conservative Christians: The Case of The Chronicles of Narnia Nathalie Dupont “Paris . As You’ve Never Seen It Before!!!”: The Promotion of Hollywood Foreign Productions in the Postwar Era Daniel Steinhart The Multiple Facets of Enter the Dragon (Robert Clouse, 1973) Pierre-François Peirano Woody Allen’s French Marketing: Everyone Says Je l’aime, Or Do They? Frédérique Brisset Varia Images of the Protestants in Northern Ireland: A Cinematic Deficit or an Exclusive -

An American Writer Ernest Hemingway's Life Style and Its
НАУЧНИ ТРУДОВЕ НА РУСЕНСКИЯ УНИВЕРСИТЕТ - 2009, том 48, серия 6.3 An American writer Ernest Hemingway’s life style and its influence to his creative activity Ruslan Mammadov Abstract: This dissertation work gives a deeper view of the literary style and philosophy of Ernest Hemingway - the American short story writer, novelist, non-fiction writer, journalist, poet, and dramatist. Mainly, it focuses on the connection between the life of Ernest Hemingway and his literary works. He enjoyed life to the fullest and wanted to show that he could do whatever he wanted and it is truly obvious that these facts deeply influenced to his future career, his creativity and private life. This paper examines reflections of the author’s childhood on his works and the effects of women’s special role on his life and creativity and on the moral and ethical relativism of Hemingway's characters. It also studies the importance and the influence of World War I on his short stories and novels. What’s more, it studies his thirst for cultural knowledge which has left indelible signs in all of his works. The aim of this research is to find out essential features of the writer’s literary activity and to explain why the above coupled with the essential messages on the concept of wealth and goodness, portrayed in Hemingway's novels, are some of the reasons why his works have been rendered classics of the American literature. Key words: Ernest Hemingway INTRODUCTION Every man`s life ends the same way. It is only the details of how he lived and how 1 he died that distinguishes one man from another. -
Of Maxwell Park
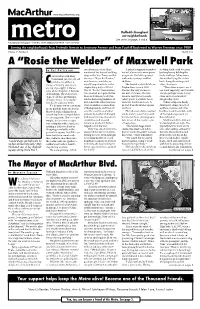
www.macarthurmetro.org TIM CHAPMAN Daffodils throughout our neighborhoods. See stories on pages 3 and 4. A Community Newspaper • P.O. Box 19046, Oakland, CA 94619 • (510) 287-2655 Serving the neighborhoods from Fruitvale Avenue to Seminary Avenue and from Foothill Boulevard to Warren Freeway since 1989 Volume 17 Number 2 March 2005 A “Rosie the Welder” of Maxwell Park B Y P AT P ATTERSON one afternoon, when Mary A friend’s suggestion guided welding torch, with two men mentioned her days of welding her to California for more prom- backing her up holding the ships in the ’40s. Turns out that ising work. She left to go west tanks and hose. Many times PAT PATTERSON onversation with Mary Weinhandl, my 93-year-old she was a “Rosie the Riveter,” with only a suitcase and her she welded lying flat on her Cnext-door neighbor, is or in her case, a welder, an children. back, doing the ceilings and always a learning experience, equally important role in the She landed a job with Moore other close spots. an ongoing supply of life les- shipbuilding days of World Shipbuilders around 1943. “There were inspections of sons, all for the price of decades War II. “Rosies” were women She was the only woman in our work regularly, and I would of friendship. The stories flow who worked in shipyards like her unit of 15 men. She was always get high marks for my of good old days in Oakland, those in Richmond and Oak- issued a heavy brown suede clean and accurate welds,” of happy times, of raising her land as increasing numbers of jacket, pants, a welder’s hood, she proudly states. -

Lire La Suite De L'article
Ernest HEMINGWAY, le guerrier blessé Figure emblématique de la « génération perdue » qui fut jetée, voire pratiquement sacrifiée dans la Première guerre mondiale et dont les survivants sont revenus totalement désabusés, Ernest HEMINGWAY, sans doute le plus lu des écrivains américains du XXe siècle, est né le 21 juillet 1899 à Oak Park dans l’état de l’Illinois aux Etats-Unis. « Son style d'écriture, caractérisé par l'économie et la litote, a influencé le roman du XXe siècle, comme l'ont fait sa vie d'aventurier et l'image publique qu'il entretenait 1 ». Son père, Clarence, dentiste, l’initie très jeune à la chasse et à la pêche lors des vacances familiales passées dans un chalet au bord du Wallon Lake, une région encore sauvage du Michigan. Pour son dixième anniversaire, Ernest reçoit un fusil de chasse. Sa mère, Grace Hall, musicienne ayant sacrifié sa vocation pour élever sa famille, cherche à lui inculquer le goût du violoncelle ce qui devient vite une «source de conflit». Deuxième enfant d’une fratrie de six dont cinq filles (il est le seul garçon), il reçoit une éducation stricte dans le respect des valeurs catholiques. Sa mère souhaite une fille et, déçue, l’habille comme s’il en était une. L’opposition Lune / Vénus, indique ce clivage de l’image féminine entre un maternel rétracté - Lune Capricorne – et un féminin érotique – Vénus en Cancer – servant de sein sécurisant. De fait, il a perçu sa mère comme froide et puritaine et recherché dans ses liaisons amoureuses un sein consolateur. Tour à tour épris de femmes lui apportant un appui social dans sa carrière ou lui servant de nourrices ou d’infirmières, il a toute sa vie oscillé entre ces deux modèles. -

Revisions, Corrections and Additions to the Hemingway Log: a Chronology of His Life and Times
Brewster Chamberlin | 1 Revisions, Corrections and Additions to The Hemingway Log: A Chronology of His Life and Times Brewster Chamberlin (University Press of Kansas, 2015) ny published chronology, regardless of subject, is out of date on the day it is printed. This is the risk writers of chronologies are well aware of Abut take that risk anyway. The Hemingway Log is no exception, which is the justification for what follows. Indeed, the tremendous amount of new and corrected material which the Hemingway industry created since 2015 is both staggering and for me embarrassing. Thus, despite the fact that the Uni- versity Press of Kansas is unable to bring out a new edition of the Log, I have determined that not making this series of revisions available to the scholarly and general public would be a disservice to both readerships. This of course is particularly true in the case of correcting errors which crept into the 2015 volume. As a result, I am particularly grateful to Kirk Curnutt and the board of the Hemingway Society for the opportunity to make this text available on the Society’s web site. In the future, as the Hemingway Letters Project staff uncovers additional information, this chronology could be extended for years, but that task will have to be accomplished by someone other than this author. I hope the following notes are reasonably clear and useful. Inevitably the entries below refer to pages and entries in the Log; this may be cumbersome but I have not been able to come up with an alternative method. -

The Imaginative Nature National Council of Teachers of En
DOCUMENT RESUME ED 404 675 CS 215 781 AUTHOR Pugh, Sharon L.; And Others TITLE Metaphorical Ways of Knowing: The Imaginative Nature of Thought and Expression. INSTITUTION National Council of Teachers of English, Urbana, Ill. REPORT NO ISBN-0-8141-3151-4 PUB DATE 97 NOTE 225p. AVAILABLE FROMNational Council of Teachers of English, 1111 W. Kenyon Road, Urbana, IL 61801-1096 (NCTE Stock No. 31514-3050: $12.95 members, $16.95 nonmembers). PUB TYPE Viewpoints (Opinion/Position Papers, Essays, etc.) (120) Books (010) EDRS PRICE MF01/PC09 Plus Postage. DESCRIPTORS Class Activities; *English; *Imagination; Interdisciplinary Approach; Intermediate Grades; Language Arts; *Language Role; *Metaphors; *Multicultural Education; Rhetoric; Secondary Education IDENTIFIERS *Metaphorical Thought ABSTRACT This book explores the subject of metaphor, using the imagery of cartography to set a course. It explores the creative aspects of thinking and learning through literature, writing, and word play, drawing connections between English and other content areas. Theory and practical applications meet in the book, linking activities and resources to current classroom concerns--to multiculturalism, imagination in reading and writing, critical thinking, and expanding language experiences. The first part of the book examines the uses of metaphor in constructing meaning. The second part takes up issues related to multiple perspectives--using metaphors to experience other lives, and exploring cultures through traditions. The third part of the book is devoted to a consideration of the history and current status of the English language and focuses on using cross-cultural stories in the English classroom, offering a number of resources for teaching multicultural literature in English. The fourth part examines the sensory Ixperience of metaphors by seeing, hearing, tasting, smelling, and touching with the imagination. -

Lanthorn, Vol. 8, No. 25, April 22, 1976 Grand Valley State University
Grand Valley State University ScholarWorks@GVSU Volume 8 Lanthorn, 1968-2001 4-22-1976 Lanthorn, vol. 8, no. 25, April 22, 1976 Grand Valley State University Follow this and additional works at: http://scholarworks.gvsu.edu/lanthorn_vol8 Part of the Archival Science Commons, Education Commons, and the History Commons Recommended Citation Grand Valley State University, "Lanthorn, vol. 8, no. 25, April 22, 1976" (1976). Volume 8. 25. http://scholarworks.gvsu.edu/lanthorn_vol8/25 This Issue is brought to you for free and open access by the Lanthorn, 1968-2001 at ScholarWorks@GVSU. It has been accepted for inclusion in Volume 8 by an authorized administrator of ScholarWorks@GVSU. For more information, please contact [email protected]. • Volume 8 Number 24 [/.£. GRAND VALLEY STATE COLLEGES April 22, 1976 Semester Proposal Submitted To ECS tivc Committee of the All-College Senate) "The members of the ECS will pro and strong opposition. The most common which is the first step in the process of bably be looking for response on the cam objections seemed to identify two prob having it approved.’’ pus to the issue, and act on the proposal lems: 1) it would effectively limit student at their meeting on May 7. From there it choices and 2) rigulify curriculum." "The ECS has accepted the report goes to the All-College Senate, and it will Another group on campus opposed of the Task Force, and has sent copies probably be voted on in their May 21 to the plan is the Veterans Brotherhood, of the report, which includes both the meeting," said Dongvillo. -

Mariel Hemingway Mariel of Courtesy Photo
55 healthy| from Trinitas Regional Medical Center Trinitas from e dg e Mariel Hemingway Photo courtesy of Mariel Hemingway Mariel of courtesy Photo amily is complicated. Mental illness within a family complicates matters exponentially. No one knows this better than actor-author- activist Mariel Hemingway. The granddaughter of Ernest FHemingway and sister of Margaux Hemingway —both of whom took their own lives—she is intimately familiar with the dark places that few of us are willing to go. In Mariel’s search for answers and quest for balance, she has developed a unique point of view—which she shares through her books and speaking engagements. With the release of the documentary Running from Crazy, she told her family’s complex story of mental illness, substance abuse and suicide and became part of a long-overdue national conversation. On October 29, Mariel Hemingway will join Jack Ford on stage at the Park Savoy in Florham Park for Out Came the Sun: Overcoming the Legacy of Mental Illness, Addiction, and Suicide, presented by the Trinitas Health Foundation. Proceeds Simon & Schuster VISIT US ON THE WEB www.edgemagonline.com 56 HEALTH from the evening will benefit the Peace of Mind Campaign, a $4 million initiative to renovate the hospital’s Department of Behavioral Health and Psychiatry. EDGE editor Mark Stewart intruded upon her summer sojourn in the mountains of Idaho to chat about her family, her passion and her career. EDGE: I’m curious about the documentary Running from Crazy. It was extraordinary. How does something like that even get made? MH: It started when one of my best friends, Lisa Erspamer, who worked with Oprah Winfrey at the time she was leaving her talk show and they were starting OWN. -

Peter Buckley
Peter Buckley: An Inventory of His Papers and Photography Collection at the Harry Ransom Center Descriptive Summary Creator: Buckley, Peter, 1925-1997 Title: Peter Buckley Papers and Photography Collection Dates: 1943-2007, undated (bulk 1950s-1970s) Extent: 32 document boxes, 10 oversize boxes (14.8 linear feet); 1 flat file drawer Abstract: The collection consists of photographic prints (approximately 1,100), contact sheets (approximately 1,900), negatives (approximately 2,500), slides (approximately 1,700), scrapbooks, correspondence, clippings, annotated books, handwritten and typed manuscripts, and book dummies, all documenting the life and career of American photographer Peter Buckley. Call Number: Photography Collection PH-2470 Language: English, French, Italian, and Spanish Access: Open for research. Please note: Transparencies may be accessed but require 24 hours advance notice. Negatives cannot be accessed without curatorial approval. Two albums have been restricted due to their fragile condition, but digital copies of these albums are available in the Ransom Center Reading and Viewing Room for patron access. To make an appointment or to reserve photography materials, please contact the Center's staff at [email protected]. Administrative Information Acquisition: Gift, 2011, 2015 (11-06-013-G) Processed by: Daniela Lozano, 2013 and Anne Kofmehl, 2015 Repository: The University of Texas at Austin, Harry Ransom Center Buckley, Peter, 1925-1997 Photography Collection PH-2470 Biographical Sketch Peter Hays Buckley was born September 13, 1925, in New York City. His father, David Augustine Buckley, and his mother, Elinor Hays Buckley, separated when he was just six months old. Buckley spent his childhood years living abroad with his mother and going to school in several European cities including Paris, London, Rome, Geneva, and Vienna. -
Revisions, Corrections and Additions to the Hemingway Log: a Chronology of His Life and Times
Brewster Chamberlin | 1 Revisions, Corrections and Additions to The Hemingway Log: A Chronology of His Life and Times Brewster Chamberlin (University Press of Kansas, 2015) ny published chronology, regardless of subject, is out of date on the day it is printed. This is the risk writers of chronologies are well aware of Abut take that risk anyway. The Hemingway Log is no exception, which is the justification for what follows. Indeed, the tremendous amount of new and corrected material which the Hemingway industry created since 2015 is both staggering and for me embarrassing. Thus, despite the fact that the Uni- versity Press of Kansas is unable to bring out a new edition of the Log, I have determined that not making this series of revisions available to the scholarly and general public would be a disservice to both readerships. This of course is particularly true in the case of correcting errors which crept into the 2015 volume. As a result, I am particularly grateful to Kirk Curnutt and the board of the Hemingway Society for the opportunity to make this text available on the Society’s web site. In the future, as the Hemingway Letters Project staff uncovers additional information, this chronology could be extended for years, but that task will have to be accomplished by someone other than this author. I hope the following notes are reasonably clear and useful. Inevitably the entries below refer to pages and entries in the Log; this may be cumbersome but I have not been able to come up with an alternative method. -
Tim Gunn Fashion Innovators
PUBLISHER’S NOTE Fashion Innovators SUR¿OHV WKH PRVW LQQRYDWLYH DQG 7KHWH[WRIWKHHVVD\VDUHGLYLGHGLQWRWKHIROORZLQJ LQÀXHQWLDO LQGLYLGXDOV LQ WKH GHYHORSPHQW RI IDVKLRQ • Early Life provides facts about the individual’s From the post–World War II revival of haute couture to upbringing. Where little is known about the per- WKH³PDVKXS´VW\OHRIWKHWZHQW\¿UVWFHQWXU\WKHKLV- son’s early life, historical context is provided. tory of fashion is immeasurably rich, with milestones • Life’s Work, the heart of the article, consists of a WKDWKDYHUHYROXWLRQL]HGRXUVRFLHW\7KLVQHZWLWOHH[- straightforward, generally chronological account amines those individuals most responsible for the design of how the individual gained recognition, em- and production behind fashion today, from designers to SKDVL]LQJ WKHLU PRVW VLJQL¿FDQW HQGHDYRUV DQG the models popularizing their designs. achievements—and failures. • Personal Information includes post-achieve- SCOPE OF COVERAGE ment activities or positions, family life, and top- Fashion Innovators features more than 180 biographies ics of general interest. RILQGLYLGXDOVZKRKDYHKDGDVLJQL¿FDQWLQÀXHQFHRQ • Each essay also includes an annotated Further the development of fashion, culminating with the styles Reading section that provides a starting point for of today that borrow from both hip-hop and unisex in- additional research. GLHVW\OHV7KHPDMRULW\RIWKHVHELRJUDSKLFDOHVVD\VDUH derived from Current Biography, which is a monthly SPECIAL FEATURES magazine that H. W. Wilson began publishing in 1940. Several features distinguish this series from other bio- Biographies represent a strong multi-ethnic, cross-gen- JUDSKLFDOUHIHUHQFHZRUNV7KHEDFNPDWWHULQFOXGHVWKH der focus, with accompanying sidebars describing the following aids, appendices, and indexes: DI¿OLDWLRQZLWKZKLFKWKDWLQGLYLGXDOLVPRVWRIWHQDV- • Timeline presents a comprehensive list of mile- sociated. Among the editors’ criteria for inclusion in the stone events in the evolution of fashion since the VHWZDVDQLQGLYLGXDO¶VKLVWRULFDOVLJQL¿FDQFHZKHWKHU 1940s.