167.Full.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Phenacetin Acts As a Weak Genotoxic Compound Preferentially in the Kidney of DNA Repair Deficient Xpa Mice
Mutation Research/Fundamental and Molecular Mechanisms of Mutagenesis Volume 596, Issues 1-2 , 11 April 2006, Pages 143-150 doi:10.1016/j.mrfmmm.2005.12.011 Copyright © 2006 Elsevier B.V. All rights reserved. Phenacetin acts as a weak genotoxic compound preferentially in the kidney of DNA repair deficient Xpa mice Mirjam Luijtena,*, Ewoud N. Speksnijdera, Niels van Alphena, Anja W estermana, Siem H. Heisterkampb, Jan van Benthema, Coen F. van Kreijla, Rudolf B. Beemsa and Harry van Steega aLaboratory of Toxicology, Pathology and Genetics, National Institute for Public Health and the Environment (RIVM), P.O. Box 1, 3720 BA Bilthoven, The Netherlands bCentre for Information Technology and Methodology, National Institute for Public Health and the Environment (RIVM), P.O. Box 1, 3720 BA Bilthoven, The Netherlands Abstract Chronic use of phenacetin-containing analgesics has been associated with the development of renal cancer. To establish genotoxicity as a possible cause for the carcinogenic effect of phenacetin, we exposed wild type and DNA repair deficient XpaÞ/Þ and XpaÞ/Þ/Trp53+/Þ mice (further referred as Xpa and Xpa/p53 mice, respectively), carrying a reporter lacZ gene, to 0.75% (w/w) phenacetin mixed in feed. Xpa mice completely lack the nucleotide excision repair pathway, and as such they are sensitive to some classes of genotoxic compounds. Phenacetin exposure induced a significant increase of lacZ mutations in the kidney of both Xpa and Xpa/p53 mice. A minor response was found in liver, whereas no lacZ mutation induction was observed in the spleen of these animals. Interestingly, the observed phenacetin-induced mutant frequencies were higher in male than those found in female mice. -

Rare Case Botryoid Rhabdomyosarcomas of the Genital Tract
ISSN: 2581-5407 DOI: https://dx.doi.org/10.17352/gjct CLINICAL GROUP Received: 25 April, 2020 Case Report Accepted: 29 April, 2020 Published: 30 April, 2020 *Corresponding author: M Lahfaoui, Department Rare Case Botryoid of Pediatric Visceral and Urogenital Surgery, Oujda Children’s Hospital. Morocco, E-mail: Rhabdomyosarcomas of the https://www.peertechz.com Genital Tract. About a case in a 30-month-old child M Lahfaoui* and H Benhaddou Department of Pediatric Visceral and Urogenital Surgery, Oujda Children’s Hospital. Morocco Abstract Rhabdomyosarcomas are the most common soft tissue sarcomas developed in children under 15 years of age. The reported fi nding is a vaginal tumour developed in a 30-month-old granddaughter. This was a typical botryoid rhabdomyosarcoma that usually occurs in the hollow organs lined with mucous membrane. Rhabdomyosarcomas have multiple aspects that vary according to the degree of cellular differentiation. The majority of these tumours can be classifi ed into four histological categories: embryonic, botryoid, alveolar or pleomorphic. Treatment involves excisional surgery combined with radiotherapy and chemotherapy. The prognosis remains bleak despite therapeutic advances in recent years. Introduction Anatomopathological examination of the specimen showed that it was a polypoid (grape-like) tissue bordered Rhabdomyosarcomas are the most common soft tissue by a slightly hyperplastic squamous epithelium. Beneath sarcomas developed in children under 15 years of age. this epithelium, within a myxoid layer, a proliferation of These tumours respond to multidisciplinary management: disseminated tumour cells was observed with an inconspicuous conservative surgery (Figure1), multi-chemotherapy and cytoplasm, a hyperchromatic, rounded or elongated nucleus, radiotherapy. Although the prognosis is always dire, a sometimes presenting cytonuclear atypia with monstrosity signifi cant proportion of children treated in this way do not metastasize [1]. -

Soft Tissue Sarcoma Classifications
Soft Tissue Sarcoma Classifications Contents: 1. Introduction 2. Summary of SSCRG’s decisions 3. Issue by issue summary of discussions A: List of codes to be included as Soft Tissue Sarcomas B: Full list of codes discussed with decisions C: Sarcomas of neither bone nor soft tissue D: Classifications by other organisations 1. Introduction We live in an age when it is increasingly important to have ‘key facts’ and ‘headline messages’. The national registry for bone and soft tissue sarcoma want to be able to produce high level factsheets for the general public with statements such as ‘There are 2000 soft tissue sarcomas annually in England’ or ‘Survival for soft tissue sarcomas is (eg) 75%’ It is not possible to write factsheets and data briefings like this, without a shared understanding from the SSCRG about which sarcomas we wish to include in our headline statistics. The registry accepts that soft tissue sarcomas are a very complex and heterogeneous group of cancers which do not easily reduce to headline figures. We will still strive to collect all data from cancer registries about anything that is ‘like a sarcoma’. We will also produce focussed data briefings on sites such as dermatofibrosarcomas and Kaposi’s sarcomas – the aim is not to forget any sites we exclude! The majority of soft tissue sarcomas have proved fairly uncontroversial in discussions with individual members of the SSCRG, but there were 7 particular issues it was necessary to make a group decision on. This paper records the decisions made and the rationale behind these decisions. 2. Summary of SSCRG’s decisions: Include all tumours with morphology codes as listed in Appendix A for any cancer site except C40 and C41 (bone). -

Aderomyoma of the Common Bile Duct --Report of a Case
Yamanashl Med. J. 4 (2), 83"v87, 1989 Case Report AdeRomyoma of the Common Bile Duct --Report of a Case Yoshiro MATsuMoTe, Masatoshi MoGAKi, Hidehisa AoyAMA, Takayoshi SEKmAwA, Katsnhiko SuGAHARA, Koichi SuDAi), and Masayuki FuJiNo2) DePa,rt・ment of Surge7pu. i)DePartment of Pathology, 2)DePartment of lnte7"nal Medicine, YamanasJzi Medical Coglege, Tamaho, Nakakoma, Ya?nanashi 409-38, JaPan Abstract: Adenomyomas in the extrahepatic biie duc£ are extremely rare. In a 75-year- old male with acute cholangitis due to adenomyoma £erming a protruding lesion iR the terminal bile duct, pamacreatoduodenectomy was carried out, resulting complete cure, Key words: Adenomyoma of the common bile duct, Early bile dact cancer, Obstructive jaundice formed, aRd £rom the histologic examina- INTRODUCTION tion of the surgical specimen, adenomyoma Adenomyoma in the biliary ductal system of the common bile duct was confirmed. is most freguently fouRd in the gallbladder. Although beRign neoplasma o£ the bile The gallbiadder wall is more abuRdant in duct system are uncommon, the tumors are muscle fibers than is the wall o£ the bile clinically very important because they can duct. Adenomyoma in the gallbladder is cause obstructive jaundice4) and require knowlt to be closely re}ated to the forma- differentiation £rom eary cancer of the bile tion of gallstones. In other parts of the duct. biliary ductal system, kex4xeve]-, adeno- We report here the surgical results and myoma is very rarei)・2), although a few pathologic findings in a case of adeno- cases of a tumor arising from the papil}a myoma of the terminal bile duct. of Vater3) have beelt reported. -

Cellular Pseudosarcomatous Fibroepithelial Stromal Polyp of the Cervix: a Lesion Mimicking As Sarcoma
Advances in Cytology & Pathology Case Report Open Access Cellular pseudosarcomatous fibroepithelial stromal polyp of the cervix: a lesion mimicking as sarcoma Abstract Volume 3 Issue 1 - 2018 Introduction: Fibroepithelial stromal polyps (FESP) are infrequent mesenchymal Mahboob Hasan1 ,Ruquiya Afrose2 ,Mariya lesions found in vulvovaginal region but may also occur in the cervix, usually 1 seen in reproductive age group. FESP exhibiting bizarre cytomorphology, atypical Kamal 1Department of pathology, Aligarh Muslim University, India mitoses, or hypercellularity, raises the possibility of malignancy and continue to be 2Department of pathology, Uttar Pradesh University of Medical underrecognized. Sciences, India Case summary: We report a case of 45 years old, postmenopausal female presented with a large polypoidal cauliflower like growth with ulcerated surface, arising from Correspondence: Ruquiya Afrose, Assistant professor, Department of Pathology, Uttar Pradesh University of Medical exocervix. Cinical diagnosis of cervical malignancy was suggested. Histopathological Sciences, Saifai Etawah, 206301, India, Tel 9219716166, examination revealed a polypoidal tumor mass composed of cellular fibrovascular Email [email protected] stroma covered with stratified squamous epithelium. There are areas showing marked hypercellularity, bizarre cytomorphology and frequent mitotic figures (>10/10 HPF) Received: November 17, 2016 | Published: February 21, 2018 including atypical ones. Important morphologic clues to the diagnosis of FESP were its superficial -
Renal Pyelocalyceal Squamous Cell Carcinoma in a Patient with An
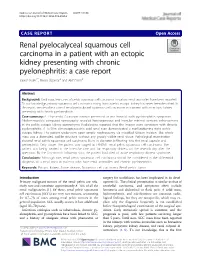
Güler et al. Journal of Medical Case Reports (2019) 13:154 https://doi.org/10.1186/s13256-019-2090-z CASEREPORT Open Access Renal pyelocalyceal squamous cell carcinoma in a patient with an ectopic kidney presenting with chronic pyelonephritis: a case report Yavuz Güler1*, Burak Üçpınar2 and Akif Erbin2 Abstract Background: Until now, few cases of pelvis squamous cell carcinoma in various renal anomalies have been reported. To our knowledge, primary squamous cell carcinoma arising from a pelvic ectopic kidney has never been described. In this report, we describe a case of renal pyelocalyceal squamous cell carcinoma in a patient with an ectopic kidney presenting with chronic pyelonephritis. Case summary: A 73-year-old Caucasian woman presented to our hospital with pyelonephritis symptoms. Abdominopelvic computed tomography revealed heterogeneous and irregular minimal contrast enhancement in the pelvic ectopic kidney parenchyma. Radiologists reported that the images were consistent with chronic pyelonephritis. A Tc-99m dimercaptosuccinic acid renal scan demonstrated a nonfunctioning right pelvic ectopic kidney. The patient underwent open simple nephrectomy via modified Gibson incision. The whole mass was a distended, saclike structure without any grossly visible renal tissue. Pathological examination showed renal pelvis squamous cell carcinoma 8 cm in diameter infiltrating into the renal capsule and perinephritic fatty tissue. The patient was staged as T4N0M1 renal pelvis squamous cell carcinoma. The patient was being treated in the intensive care unit for respiratory distress on the seventh day after the operation. By the first-month follow-up visit, the patient had died of acute respiratory distress syndrome. Conclusions: Although rare, renal pelvis squamous cell carcinoma should be considered in the differential diagnosis of a renal mass in patients who have renal anomalies and chronic pyelonephritis. -

HIV-1: Cancer Evaluation 8/1/16
Report on Carcinogens Monograph on Human Immunodeficiency Virus Type 1 August 2016 Report on Carcinogens Monograph on Human Immunodeficiency Virus Type 1 August 1, 2016 Office of the Report on Carcinogens Division of the National Toxicology Program National Institute of Environmental Health Sciences U.S. Department of Health and Human Services This Page Intentionally Left Blank RoC Monograph on HIV-1: Cancer Evaluation 8/1/16 Foreword The National Toxicology Program (NTP) is an interagency program within the Public Health Service (PHS) of the Department of Health and Human Services (HHS) and is headquartered at the National Institute of Environmental Health Sciences of the National Institutes of Health (NIEHS/NIH). Three agencies contribute resources to the program: NIEHS/NIH, the National Institute for Occupational Safety and Health of the Centers for Disease Control and Prevention (NIOSH/CDC), and the National Center for Toxicological Research of the Food and Drug Administration (NCTR/FDA). Established in 1978, the NTP is charged with coordinating toxicological testing activities, strengthening the science base in toxicology, developing and validating improved testing methods, and providing information about potentially toxic substances to health regulatory and research agencies, scientific and medical communities, and the public. The Report on Carcinogens (RoC) is prepared in response to Section 301 of the Public Health Service Act as amended. The RoC contains a list of identified substances (i) that either are known to be human carcinogens or are reasonably anticipated to be human carcinogens and (ii) to which a significant number of persons residing in the United States are exposed. The NTP, with assistance from other Federal health and regulatory agencies and nongovernmental institutions, prepares the report for the Secretary, Department of HHS. -

Application of Percutaneous Osteoplasty in Treating Pelvic Bone Metastases: Efficacy and Safety
Cardiovasc Intervent Radiol (2019) 42:1738–1744 https://doi.org/10.1007/s00270-019-02320-8 CLINICAL INVESTIGATION NON-VASCULAR INTERVENTIONS Application of Percutaneous Osteoplasty in Treating Pelvic Bone Metastases: Efficacy and Safety 1 1 1 1 1 He-Fei Liu • Chun-Gen Wu • Qing-Hua Tian • Tao Wang • Fei Yi Received: 17 October 2018 / Accepted: 20 August 2019 / Published online: 23 September 2019 Ó Springer Science+Business Media, LLC, part of Springer Nature and the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2019 Abstract 1.87 ± 1.46 at 6 months (P \ 0.05), 1.90 ± 1.47 at Background Percutaneous vertebroplasty has been a good 9 months (P \ 0.05), and 1.49 ± 1.17 at 12 months option to treat vertebral metastases. The pelvic bone is a (P \ 0.05). The ODI also changed after the procedure, common site of spread for many cancers. Using follow-up with significant differences between baseline scores and at data for 126 patients, we evaluated the safety and efficacy each follow-up examination (P \ 0.05). Pain relief was of percutaneous osteoplasty (POP) to treat pelvic bone achieved in 118 patients (93.65%); however, pain relief metastases. was not obvious in seven patients (5.56%), and pain was Materials and Methods In this retrospective study, 126 aggravated in one patient (0.79%). Extraosseous cement patients (mean age 57.45 ± 11.46 years old) with 178 leakage occurred in 35 patients (27.78%) without causing lesions were treated using POP. The visual analog scale any clinical complications. (VAS), Oswestry Disability Index (ODI), and the changes Conclusion Percutaneous osteoplasty is a safe and effec- in the patient’s use of painkillers were used to evaluate pain tive choice for patients with painful osteolytic pelvic bone and quality of life before the procedure, and at 3 days and metastases. -

Sarcoma of the Vagina
570 MCFARLAND: SARCOMA OF VAGINA Thompson and Harris. Jour. Med. Research, 190S, xiv. 135. Thompson. CtbU. f. allg. Path. u. path. Anat., l'JO'J, xx, 91G. Vassalo and Generali. Rivista di patol. Xerv. o Ment., IStHJ, i. 95; Arch. ital. de biol., 189G, xxv. 459; ibid., xxvi, Gl. Vassale. Arch. ital. de biol., 1S9S, xxx, 49. Von VerebOy, Virchow's Archive 1907, clxxxvii. SO. Wasscrtrilling. Alls. Wiener rued. Ztg., 190S. liii. 2S9. 299, 312. Weiss. Ueber Tetanic, Volkmann’s S:numlui)K klin. Vortrage, 1SS1, Nr. 1S9, 1G75. Welsh. Jour. Anat. and Physiol., 1S9S, xxxii, 292 and 3S0. Yanasc. Jalirb. fur Kinderheilkunde. Ixvii, Frsanxunsshcft, 190S, 57. SARCOMA OF THE VAGINA. A STATISTICAL STUDY OF 102 CASES, WITH THE REPORT OF A NEW CASE OF THE GRAPE-LIKE SARCOMA OF THE VAGINA IN AN INFANT. By Joseph McFarland, M.D., ruornssnn or tathologt and r.ACTxniou>cr i.v Tin; ucDtco-cinnunniCAX, coixrcr, nilLADCLFUlA. Sarcoma of the vagina is so rare an affection that the literature contains a total of 101 eases to which I add a new one, making 102 cases upon record. Its rarity and its fatality combine to make it an interesting affection, and when an attempt is made to review the literature of the subject so many features of interest present themselves that the matter becomes quite absorbing. Sarcoma of the female organs of generation may be divided clin¬ ically into those arising from the vulva, from the vagina, from the vesicovagii d septum, from the rectovaginal septum, from the cervix uteri, trout the corpus uteri, and from the ovary. -
A Case of Incidental Schwannoma Mimicking Necrotic Metastatic Lymph Node from Bladder Cancer
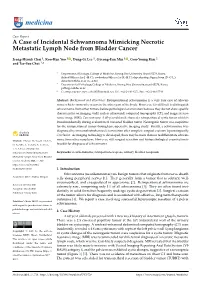
medicina Case Report A Case of Incidental Schwannoma Mimicking Necrotic Metastatic Lymph Node from Bladder Cancer Jeong-Hyouk Choi 1, Koo-Han Yoo 1 , Dong-Gi Lee 1, Gyeong-Eun Min 1 , Gou-Young Kim 2 and Tae-Soo Choi 1,* 1 Department of Urology, College of Medicine, Kyung Hee University, Seoul 05278, Korea; [email protected] (J.-H.C.); [email protected] (K.-H.Y.); [email protected] (D.-G.L.); [email protected] (G.-E.M.) 2 Department of Pathology, College of Medicine, Kyung Hee University, Seoul 05278, Korea; [email protected] * Correspondence: [email protected]; Tel.: +82-2-440-6271; Fax: +82-2-440-7744 Abstract: Background and Objectives: Retroperitoneal schwannoma is a very rare case of schwan- noma which commonly occurs in the other part of the body. However, it is difficult to distinguish schwannoma from other tumors before pathological examination because they do not show specific characteristics on imaging study such as ultrasound, computed tomography (CT), and magnetic reso- nance image (MRI). Case summary: A 60-year-old male showed a retroperitoneal cystic tumor which is found incidentally during evaluation of coexisted bladder tumor. Neurogenic tumor was suspicious for the retroperitoneal tumor through pre-operative imaging study. Finally, a schwannoma was diagnosed by immunohistochemical examination after complete surgical excision laparoscopically. Conclusion: As imaging technology is developed, there may be more chances to differentiate schwan- Citation: Choi, J.-H.; Yoo, K.-H.; Lee, noma from other neoplasm. However, still surgical resection and histopathological examination is D.-G.; Min, G.-E.; Kim, G.-Y.; Choi, feasible for diagnosis of schwannoma. -

Primary Endometrial Stromal Sarcoma Arising from Cervix
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 12 Ver. VI (Dec. 2015), PP 139-144 www.iosrjournals.org Primary Endometrial Stromal Sarcoma arising from Cervix Dr. Jindal Dweep1, Dr. Jindal Manjusha2 1(Ex Senior resident, Department of OBG, Goa Medical College, Bambolim, Goa, India) 2(Associate professor, Department of OBG, Goa Medical College, Bambolim, Goa, India) Abstract:Endometrial stromal sarcomas are rare malignant tumors of the uterus (0.2% of all uterine malignancies). The primary tumor can occur in extra-uterine sites like ovary, fallopian tube, cervix, vulva, vagina, omentum and retro peritoneum. There are only 18 cases reported in literature of ESS arising from cervix till date. Primary tumor arising in the cervix mimics a fibroid polyp and poses a diagnostic dilemma. A pre-operative diagnosis of ESS is difficult and the diagnosis is retrospective from histopathology of a hysterctomy specimen done for presumed benign disease. We report a case of 48 years old perimenopausal lady who presented with irregular bleeding per vaginum and retention of urine. Clinical examination was suggestive of degenerated fibroid polyp. She gave history of removal of similar mass nine months earlier, the details of which were not known. In view of her age and recurrence of symptoms, total hysterectomy with bilateral salpingo-oophrectomy was done. The diagnosis was established on gross findings, cut section, histopathology and immunohistochemistry. The case report emphasises the need to include ESS in the differential diagnosis of cervical polyp.The role of adjuvant hormone therapy, chemotherapy and radiation is discussed. -

A Gastrointestinal Stromal Tumor Presenting As a Pelvic Mass: a Case Report
899-902 4/3/2009 11:12 Ì ™ÂÏ›‰·899 ONCOLOGY REPORTS 21: 899-902, 2009 899 A gastrointestinal stromal tumor presenting as a pelvic mass: A case report ROBERTO ANGIOLI1, CLEONICE BATTISTA1, LUDOVICO MUZII1, GIOVANNA MADONNA TERRACINA1, ESTER VALENTINA CAFÀ1, MARIA ISABELLA SERENI1, ROBERTO MONTERA1, FRANCESCO PLOTTI2, CARLA RABITTI1 and PIERLUIGI BENEDETTI PANICI2 1Department of Obstetrics and Gynecology ‘Campus Biomedico’ University of Rome, Via Alvaro del Portillo 200, 00128 Rome; 2Department of Obstetrics and Gynecology ‘La Sapienza’ University of Rome, V.le del Policlinico 155, 00161 Rome, Italy Received March 18, 2008; Accepted September 19, 2008 DOI: 10.3892/or_00000301 Abstract. Gastrointestinal stromal tumors (GISTs) represent include the gallbladder or bladder (5). In terms of distribution, 0.1-1% of gastrointestinal malignancies. They are commonly 50-60% of lesions arise in the stomach, 20-30% in the small asymptomatic and found incidentally during laparoscopy, bowel, 10% in the large bowel, 5% in the oesophagus and 5% surgical procedures or radiological studies. Diagnosis is elsewhere in the abdominal cavity (5-7). based on histology and immunohistochemistry, while the role Diagnosis is based on histology and immunohisto- of imaging studies is not diagnosis-specific. We present the chemistry. In the past, GISTs were considered to be part of GI case of a 38-year-old patient complaining of an increase in leiomyomas, leiomyosarcomas, leiomyoblastomas and the her abdominal circumference. Consequently, a vaginal schwannomas group (Table I) as a result of their histological examination, a transvaginal ultrasound and an MRI of the findings and apparent origin in the muscolaris propria layer of abdomen and pelvis were carried out.