Mechanical Small Bowel Obstruction Secondary to Acute Cholecystitis in the Context of an Irreducible Inguinal Hernia: a Case Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Inflammatory Bowel Disease Irritable Bowel Syndrome
Inflammatory Bowel Disease and Irritable Bowel Syndrome Similarities and Differences 2 www.ccfa.org IBD Help Center: 888.MY.GUT.PAIN 888.694.8872 Important Differences Between IBD and IBS Many diseases and conditions can affect the gastrointestinal (GI) tract, which is part of the digestive system and includes the esophagus, stomach, small intestine and large intestine. These diseases and conditions include inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS). IBD Help Center: 888.MY.GUT.PAIN 888.694.8872 www.ccfa.org 3 Inflammatory bowel diseases are a group of inflammatory conditions in which the body’s own immune system attacks parts of the digestive system. Inflammatory Bowel Disease Inflammatory bowel diseases are a group of inflamma- Causes tory conditions in which the body’s own immune system attacks parts of the digestive system. The two most com- The exact cause of IBD remains unknown. Researchers mon inflammatory bowel diseases are Crohn’s disease believe that a combination of four factors lead to IBD: a (CD) and ulcerative colitis (UC). IBD affects as many as 1.4 genetic component, an environmental trigger, an imbal- million Americans, most of whom are diagnosed before ance of intestinal bacteria and an inappropriate reaction age 35. There is no cure for IBD but there are treatments to from the immune system. Immune cells normally protect reduce and control the symptoms of the disease. the body from infection, but in people with IBD, the immune system mistakes harmless substances in the CD and UC cause chronic inflammation of the GI tract. CD intestine for foreign substances and launches an attack, can affect any part of the GI tract, but frequently affects the resulting in inflammation. -

Diverticular Abscess Presenting As a Strangulated Inguinal Hernia: Case Report and Review of the Literature
Ulster Med J 2007; 76 (2) 107-108 Presidential Address 107 Case Report Diverticular Abscess Presenting as a Strangulated Inguinal Hernia: Case Report and review of the literature. S Imran H Andrabi, Ashish Pitale*, Ahmed AS El-Hakeem Accepted 22 December 2006 ABSTRACT noted nausea, anorexia and increasing abdominal pain. She had no previous history of any surgery or trauma and was on Potentially life threatening diseases can mimic a groin hernia. warfarin for atrial fibrillation. We present an unusual case of diverticulitis with perforation and a resulting abscess presenting as a strangulated inguinal hernia. The features demonstrated were not due to strangulation of the contents of the hernia but rather pus tracking into the hernia sac from the peritoneal cavity. The patient underwent sigmoid resection and drainage of retroperitoneal and pericolonic abscesses. Radiological and laboratory studies augment in reaching a diagnosis. The differential diagnosis of inguinal swellings is discussed. Key Words: Diverticulitis, diverticular perforation, diverticular abscess, inguinal hernia INTRODUCTION The association of complicated inguinal hernia and diverticulitis is rare1. Diverticulitis can present as left iliac fossa pain, rectal bleeding, fistulas, perforation, bowel obstruction and abscesses. Our patient presented with a diverticular perforation resulting in an abscess tracking into the inguinal canal and clinically masquerading as a Fig 2. CT scan showing inflammatory changes with strangulated inguinal hernia. The management warranted an stranding of the subcutaneous fat in the left groin and a exploratory laparotomy and drainage of pus. large bowel diverticulum CASE REPORT On admission, she had a tachycardia (pulse 102 beats/min) and a temperature of 37.5OC. -

A Case Report of Fibro-Stenotic Crohn's Disease in the Middle
DOI: https://doi.org/10.22516/25007440.185 Case report A Case Report of Fibro-Stenotic Crohn’s Disease in the Middle Ileum as the Initial Manifestation Adriana Margarita Rey,1 Gustavo Reyes,1 Fernando Sierra,1 Rafael García-Duperly,2 Rocío López,3 Leidy Paola Prada.4 1 Gastroenterologist in the Gastroenterology and Abstract Hepatology Service of the Hospital Universitario Fundación Santa Fe de Bogotá in Bogotá, Colombia Crohn’s disease (CD) is an inflammatory bowel disease that can affect the entire gastrointestinal tract. The small 2 Colon and Rectum Surgeon in the Department of intestine is affected in about 50% of patients among whom the terminal ileum is the area most commonly affected. Surgery of the Hospital Universitario Fundación Intestinal stenosis is a common complication in CD and approximately 30% to 50% of patients present Santa Fe de Bogotá in Bogotá, Colombia 3 Pathologist at of the Hospital Universitario Fundación stenosis or penetrating lesions at the time of diagnosis. Because conventional endoscopic techniques do not Santa Fe de Bogotá and Professor at Universidad de allow evaluation of small bowel lesions, techniques such as enteroscopy and endoscopic video-capsule were los Andes in Bogotá, Colombia developed. Each has advantages and indications. 4 Third Year Internal Medicine Resident at the Hospital Universitario Fundación Santa Fe de Bogotá in We present the case of a patient with CD with localized fibrostenosis in the middle ileum which is not a Bogotá, Colombia frequent site for this type of lesion. Author for correspondence: Adriana Margarita Rey. Bogotá D.C. Colombia [email protected] Keywords ........................................ -

Adult Intussusception
1 Adult Intussusception Saulius Paskauskas and Dainius Pavalkis Lithuanian University of Health Sciences Kaunas Lithuania 1. Introduction Intussusception is defined as the invagination of one segment of the gastrointestinal tract and its mesentery (intussusceptum) into the lumen of an adjacent distal segment of the gastrointestinal tract (intussuscipiens). Sliding within the bowel is propelled by intestinal peristalsis and may lead to intestinal obstruction and ischemia. Adult intussusception is a rare condition wich can occur in any site of gastrointestinal tract from stomach to rectum. It represents only about 5% of all intussusceptions (Agha, 1986) and causes 1-5% of all cases of intestinal obstructions (Begos et al., 1997; Eisen et al., 1999). Intussusception accounts for 0.003–0.02% of all hospital admissions (Weilbaecher et al., 1971). The mean age for intussusception in adults is 50 years, and and the male-to-female ratio is 1:1.3 (Rathore et. al., 2006). The child to adult ratio is more than 20:1. The condition is found in less than 1 in 1300 abdominal operations and 1 in 100 patients operated for intestinal obstruction. Intussusception in adults occurs less frequently in the colon than in the small bowel (Zubaidi et al., 2006; Wang et al., 2007). Mortality for adult intussusceptions increases from 8.7% for the benign lesions to 52.4% for the malignant variety (Azar & Berger, 1997) 2. Etiology of adult intussusception Unlike children where most cases are idiopathic, intussusception in adults has an identifiable etiology in 80- 90% of cases. The etiology of intussusception of the stomach, small bowel and the colon is quite different (Table 1). -

Clinical Acute Abdominal Pain in Children
Clinical Acute Abdominal Pain in Children Urgent message: This article will guide you through the differential diagnosis, management and disposition of pediatric patients present- ing with acute abdominal pain. KAYLEENE E. PAGÁN CORREA, MD, FAAP Introduction y tummy hurts.” That is a simple statement that shows a common complaint from children who seek “M 1 care in an urgent care or emergency department. But the diagnosis in such patients can be challenging for a clinician because of the diverse etiologies. Acute abdominal pain is commonly caused by self-limiting con- ditions but also may herald serious medical or surgical emergencies, such as appendicitis. Making a timely diag- nosis is important to reduce the rate of complications but it can be challenging, particularly in infants and young children. Excellent history-taking skills accompanied by a careful, thorough physical exam are key to making the diagnosis or at least making a reasonable conclusion about a patient’s care.2 This article discusses the differential diagnosis for acute abdominal pain in children and offers guidance for initial evaluation and management of pediatric patients presenting with this complaint. © Getty Images Contrary to visceral pain, somatoparietal pain is well Pathophysiology localized, intense (sharp), and associated with one side Abdominal pain localization is confounded by the or the other because the nerves associated are numerous, nature of the pain receptors involved and may be clas- myelinated and transmit to a specific dorsal root ganglia. sified as visceral, somatoparietal, or referred pain. Vis- Somatoparietal pain receptors are principally located in ceral pain is not well localized because the afferent the parietal peritoneum, muscle and skin and usually nerves have fewer endings in the gut, are not myeli- respond to stretching, tearing or inflammation. -
Recognizing-Consitpation-And-Bowel
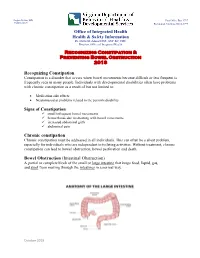
Hughes Melton, MD Post Office Box 1797 Commissioner Richmond, Virginia 23218-1797 Office of Integrated Health Health & Safety Information Dr. Dawn M. Adams DNP, ANP-BC, CHC Director, Office of Integrated Health Recognizing Constipation & Preventing Bowel Obstruction 2018 Recognizing Constipation Constipation is a disorder that occurs when bowel movements become difficult or less frequent is frequently seen in many people. Individuals with developmental disabilities often have problems with chronic constipation as a result of but not limited to: Medication side effects Neuromuscular problems related to the person's disability Signs of Constipation small infrequent bowel movements hemorrhoids due to straining with bowel movements increased abdominal girth abdominal pain Chronic constipation Chronic constipation must be addressed in all individuals. This can often be a silent problem, especially for individuals who are independent in toileting activities. Without treatment, chronic constipation can lead to bowel obstruction, bowel perforation and death. Bowel Obstruction (Intestinal Obstruction) A partial or complete block of the small or large intestine that keeps food, liquid, gas, and stool from moving through the intestines in a normal way. October 2018 Hughes Melton, MD Post Office Box 1797 Commissioner Richmond, Virginia 23218-1797 Bowel obstructions may be caused by a twist in the intestines. Intestines are called the gut. The large intestine includes the appendix, cecum, colon, and rectum and is 5 feet long. It absorbs water from stool and changes it from a liquid to a solid form. The small intestine is where most digestion occurs. It measures about 20 feet and includes the duodenum, jejunum, and ileum. o Digestion is the process of breaking down food into substances the body can use for energy, tissue growth, and repair. -

Incarcerated Gallbladder in Inguinal Hernia: a Case Report and Literature
Tajti Jr. et al. BMC Gastroenterol (2020) 20:425 https://doi.org/10.1186/s12876-020-01569-5 CASE REPORT Open Access Incarcerated gallbladder in inguinal hernia: a case report and literature review János Tajti Jr., József Pieler, Szabolcs Ábrahám, Zsolt Simonka, Attila Paszt and György Lázár* Abstract Background: Treating hernias is one of the oldest challenges in surgery. The gallbladder as content in the case of abdominal hernias has only been reported in a few cases in the current literature. Cholecyst has only been described in the content of an inguinofemoral hernia in one case to date. Case presentation: A 73-year-old female patient was admitted to the Emergency Department due to complaints in the right inguinal area, which had started 1 day earlier. The patient complained of cramp-like abdominal pain and nausea. Physical examination confrmed an apple-sized, irreducible hernia in the right inguinal region. Abdominal ultrasound confrmed an oedematous intestinal loop in a 70-mm-long hernial sac, with no circulation detected. Abdominal X-ray showed no signs of passage disorder. White blood cell count and C-reactive protein level were elevated, and hepatic enzymes were normal in the laboratory fndings. Exploration was performed via an inguinal incision on the right side, an uncertain cystic structure was found in the hernial sac, and several small abnormal masses were palpated there. The abdominal cavity was explored from the middle midline laparotomy. During the exploration, the content of the hernial sac was found to be the fundus of the signifcantly ptotic, large gallbladder. Cholecystectomy and Bassini’s repair of the inguinal hernia were performed safely. -

Pediatric Hernia
Pediatric Surgery Pediatric Hernia Pediatric Hernias: Definitions, Diagnosis and Treatment Hernia repair is among the most common type of general surgical procedure performed in children each year. The two most common types of congenital hernias in children are umbilical and inguinal hernias. The infor- mation below offers information on symptoms, diagnosis and treatment of these medical conditions. Umbilical Hernia Umbilical hernias are fairly common among newborns and infants younger than 6 months. Caused when the umbilical ring fails to close after birth, umbilical hernias present as an outward bulging in the abdominal area at the umbilicus. Umbilical hernias can vary in width from less than 1 cm to more than 5 cm and may seem to expand when the child cries or strains. Although the exact incidence of umbilical hernias in children is unknown, they are reported slightly more often in African Americans. Symptoms and Diagnosis • Present as a soft swelling at the navel that bulges when the baby or child sits up, cries or strains and usually disappears when the baby or child lies flat. • Usually painless. • Often detected on physical exam, without the need for additional testing. Treatment • Often closes by 1 or 2 years of age. • Surgery needed when hernia has not closed by 2 to 4 years of age. • Emergency surgery required if intestinal blood supply is cut off (strangulation). Inguinal Hernias There are two types of inguinal hernias — direct and indirect. Direct inguinal hernias are very rare in children and are caused by a weakness in the abdominal wall that allows intestines to protrude through. -

Patient Selection Criteria
M∙ACS MACS Patient Selection Criteria The objective is to screen, on a daily basis, the Acute Care Surgical service “touches” at your hospital to identify patients who meet criteria for further data entry. The specific patient diseases/conditions that we are interested in capturing for emergent general surgery (EGS) are: 1. Acute Appendicitis 2. Acute Gallbladder Disease a. Acute Cholecystitis b. Choledocholithiasis c. Cholangitis d. Gallstone Pancreatitis 3. Small Bowel Obstruction a. Adhesive b. Hernia 4. Emergent Exploratory Laparotomy (Refer to the ex-lap algorithm under the Diseases or Conditions section below for inclusion/exclusion criteria.) The daily census for patients admitted to the Acute Care Surgery Service or seen as a consult will have to be screened. There may be other sources to accomplish this screening such as IT and we are interested in learning about these sources from you. From this census, a list can be compiled of patients with the aforementioned diseases/conditions. The first level of data entry involves capture and entry of the patient into the MACS Qualtrics database. All patients with the identified diseases/conditions will have data entered regardless of whether or not they received an operation during admission/ED visit. The second level of data entry takes place if an existing MACS patient returns to the hospital (ED or admission) or has outcome events identified within the 30-day post-operative time frame if the patient had surgery, or within 30 days from discharge for the non-operative patients. You will see that we are capturing diagnostic, interventional, and therapeutic data that extend beyond what is typically captured for MSQC patients. -

Management of Incidental Amyand Hernia with a Case Report
CASE REPORT East J Med 24(4): 551-553, 2019 DOI: 10.5505/ejm.2019.82787 Management of Incidental Amyand Hernia With A Case Report Tolga Kalayci*, Ümit Haluk Iliklerden Department of General Surgery,Yuzuncu Yil University Faculty of Medicine,Van,Turkey ABSTRACT The presence of appendix vermiformis in inguinal hernia is known as Amyand hernia. Amyand hernia is a rare condition estimated to account for approximately 1% of all inguinal hernias. In our case we want to show our approach to incidental Amyand hernia. An 80-year-old male patient was received at urology service at Van Yuzuncu Yil University Department of Medicine because of prostatic symptoms. There were comorbid factors like hypertension,chronic obstructive lung disease and geriatric age. On surgery with spinal anesthesia, surgeons invited us to evaluate his left inguinal hernia. We evaluated hernia and saw distal ileal segments, proximal right colonic segments and inflamme appendix at hernia defect. Because of appendix inflammation we performed appendectomy. Hernia was repaired with mesh. We put a drain at surgery area. At postoperative first day, the patient discharged with drain. The fifth day of post-surgery, the drain was pulled out. At the time of 1st and 3rd month check of the patient, there was no problem about surgery. Amyand hernia is one of the rare conditions encountered by the surgeon during hernia surgery. The surgeon must know the Rosanoff and Bassoon Classification of Amyand Hernia to successfully manage Amyand hernia surgery. The surgeon also must know the situation in which case an appendectomy should be performed and in which case the mesh should be used. -

Small Bowel Obstruction Following Appendectomy: a Retrospective Study
New Indian Journal of Surgery21 Original Article January - March 2012, Volume 3 Number 1 Small Bowel Obstruction Following Appendectomy: A Retrospective Study Jyothi S Karegoudar*, Prabhakar PJ**, Rajashri S Patil***, VIjayanath V**** *Asso. Prof in General Surgery, ** Prof & HOD in General Surgery, ***Asst. Prof (biostatistician), S. S. I. M. S & R. C., Davangere, Karnataka State, ****MD, DNB, MNAMS, Associate Professor, Department of Forensic Medicine & Toxicology, Vinayaka Mission’s Kirupananda Variyar Medical College & Hospital, Salem,Tamil Nadu, India. Abstract appendectomy adhesive small bowel The incidence of post-operative small bowel obstruction occurs in 1 to 1.5% of all patients obstruction after standard, open appendectomy was within 14 years of the operation.[1] calculated during five year duration at S. S. Institute Appendectomy is one of the most frequently and Research Centre, Davangere, Karnataka State. performed emergency surgery, and it is Post-operative small bowel obstruction is one of associated with various short and long term the adverse effects of appendectomy but its frequency morbidities. Postoperative small bowel varies from centre to centre. The incidence of small obstruction is recognized as long term adverse bowel obstruction is significantly high in perforated effect of appendectomy.[2] appendicitis, midline incisions, and chronic appendicular pathology. The midline incision has The frequency of this complication is not increased the frequency of post-operative adhesions. well known but the reported risk ranges from This study was conducted to determine the 0.2- 10.7%.[3] The post-operative adhesions incidence of this complication among our patients are a significant problem after colorectal who had open appendectomy and identify the factors surgery. -

Colonic Ischemia 9/21/14, 9:02 PM
Colonic ischemia 9/21/14, 9:02 PM Official reprint from UpToDate® www.uptodate.com ©2014 UpToDate® Colonic ischemia Authors Section Editors Deputy Editor Peter Grubel, MD John F Eidt, MD Kathryn A Collins, MD, PhD, FACS J Thomas Lamont, MD Joseph L Mills, Sr, MD Martin Weiser, MD All topics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Aug 2014. | This topic last updated: Aug 25, 2014. INTRODUCTION — Intestinal ischemia is caused by a reduction in blood flow, which can be related to acute arterial occlusion (embolic, thrombotic), venous thrombosis, or hypoperfusion of the mesenteric vasculature causing nonocclusive ischemia. Colonic ischemia is the most frequent form of intestinal ischemia, most often affecting the elderly [1]. Approximately 15 percent of patients with colonic ischemia develop gangrene, the consequences of which can be life-threatening, making rapid diagnosis and treatment imperative. The remainder develops nongangrenous ischemia, which is usually transient and resolves without sequelae [2]. However, some of these patients will have a more prolonged course or develop long-term complications, such as stricture or chronic ischemic colitis. The diagnosis and treatment of patients can be challenging since colonic ischemia often occurs in patients who are debilitated and have multiple medical problems. The clinical features, diagnosis, and treatment of ischemia affecting the colon and rectum will be reviewed here. Acute and chronic intestinal ischemia of the small intestine are discussed separately. (See "Acute mesenteric ischemia" and "Chronic mesenteric ischemia".) BLOOD SUPPLY OF THE COLON — The circulation to the large intestine and rectum is derived from the superior mesenteric artery (SMA), inferior mesenteric artery (IMA), and internal iliac arteries (figure 1).