Table 1 NBIA Disorders Disease Gene Inheritance Clinical Presentation MRI
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Formation of Lipofuscin-Like Autofluorescent Granules in the Retinal Pigment Epithelium Requires Lysosome Dysfunction
Retinal Cell Biology Formation of Lipofuscin-Like Autofluorescent Granules in the Retinal Pigment Epithelium Requires Lysosome Dysfunction Cristina Escrevente,1 Ana S. Falcão,1 Michael J. Hall,2 Mafalda Lopes-da-Silva,1 Pedro Antas,1 Miguel M. Mesquita,1 Inês S. Ferreira,1 M. Helena Cardoso,1 Daniela Oliveira,1 Ana C. Fradinho,1 Thomas Ciossek,3 Paul Nicklin,3 Clare E. Futter,2 Sandra Tenreiro,1 and Miguel C. Seabra1,2 1iNOVA4Health, CEDOC – Chronic Diseases Research Center, NOVA Medical School, Universidade Nova de Lisboa, Lisboa, Portugal 2UCL Institute of Ophthalmology, London, United Kingdom 3Research Beyond Borders, Boehringer Ingelheim, Biberach, Germany Correspondence: Miguel C. Seabra, PURPOSE. We aim to characterize the pathways required for autofluorescent granule (AFG) CEDOC - NOVA Medical School, formation by RPE cells using cultured monolayers. Universidade Nova de Lisboa, 1169-056 Lisboa, Portugal; METHODS. We fed RPE monolayers in culture with a single pulse of photoreceptor outer [email protected]. segments (POS). After 24 hours the cells started accumulating AFGs that were compa- rable to lipofuscin in vivo. Using this model, we used a variety of light and electron Received: January 24, 2021 microscopical techniques, flow cytometry and Western blot to analyze the formation of Accepted: June 29, 2021 Published: July 27, 2021 AFGs. We also generated a mutant RPE line lacking cathepsin D by gene editing. Citation: Escrevente C, Falcão AS, RESULTS. AFGs seem to derive from incompletely digested POS-containing phagosomes Hall MJ, et al. Formation of and after 3 days are surrounded by a single membrane positive for lysosome markers. We lipofuscin-like autofluorescent show by various methods that lysosome-phagosome fusion is required for AFG formation, granules in the retinal pigment and that impairment of lysosomal pH or catalytic activity, particularly cathepsin D activity, epithelium requires lysosome enhances AF accumulation. -

Mini-Review on Lipofuscin and Aging: Focusing on the Molecular Interface, the Biological Recycling Mechanism, Oxidative Stress, and the Gut-Brain Axis Functionality
medicina Review Mini-Review on Lipofuscin and Aging: Focusing on The Molecular Interface, The Biological Recycling Mechanism, Oxidative Stress, and The Gut-Brain Axis Functionality Ovidiu-Dumitru Ilie 1,* , Alin Ciobica 1,2,*, Sorin Riga 2, Nitasha Dhunna 3, Jack McKenna 4, Ioannis Mavroudis 5,6, Bogdan Doroftei 7 , Adela-Magdalena Ciobanu 8 and Dan Riga 2 1 Department of Biology, Faculty of Biology, “Alexandru Ioan Cuza” University, Carol I Avenue, no 20A, 700505 Iasi, Romania 2 Academy of Romanian Scientists, Splaiul Independentei, no. 54, sector 5, 050094 Bucharest, Romania; [email protected] (S.R.); [email protected] (D.R.) 3 Mid Yorkshire Hospitals NHS Trust, Pinderfields Hospital, Wakefield WF1 4DG, UK; [email protected] 4 York Hospital, Wigginton road Clifton, York YO31 8HE, UK; [email protected] 5 Leeds Teaching Hospitals NHS Trust, Great George St, Leeds LS1 3EX, UK; [email protected] 6 Laboratory of Neuropathology and Electron Microscopy, School of Medicine, Aristotle University of Thessaloniki, 541 24 Thessaloniki, Greece 7 Faculty of Medicine, University of Medicine and Pharmacy “Grigore T. Popa”, University Street, no 16, 700115 Iasi, Romania; [email protected] 8 Discipline of Psychiatry, Faculty of Medicine, “Carol Davila” University of Medicine and Pharmacy, Dionisie Lupu Street, no 37, 020021 Bucharest, Romania; [email protected] * Correspondence: [email protected] (O.-D.I.); [email protected] (A.C.) Received: 17 September 2020; Accepted: 17 November 2020; Published: 19 November 2020 Abstract: Intra-lysosomal accumulation of the autofluorescent “residue” known as lipofuscin, which is found within postmitotic cells, remains controversial. Although it was considered a harmless hallmark of aging, its presence is detrimental as it continually accumulates. -

NCL Description for Cocker Spaniels
NCL Description for Cocker Spaniels Age of onset of clinical signs: 1.5 - 6 years Age of death or euthanasia: 1.5 - 6 years Abnormalities often observed by the owner: Mental changes: Aggression, irritability, dementia Changes in gait and posture: progressive difficulty walking; weakness and uncoordinated movement. Visual abnormalities: blindness may be present in some cases Seizures/convulsions: reported in some cases Other changes: Jaw champing, head tremors, emaciation Abnormalities observed upon clinical examinations: Clinical neurologic changes: Gait abnormalities, weakness, uncoordinated movement (hypermetric ataxia, proprioceptive deficits, exaggerated spinal reflexes) Clinical ophthalmic changes: ophthalmic changes have been reported Visual abnormalities: blindness has been reported Retinal changes: retinal atrophy has been reported Electroretinography (ERG): not described in reported cases Other clinical findings: none reported Histopathology Brain: Yellow-brown granules were present in neuronal cytoplasm of some neurons in the brain and spinal cord. Storage granules were most abundant in the spinal cord and cerebellum. Cells in the cerebral cortex, brain stem, and Purkinje cells were less affected. Affected neurons were swollen, and often had an eccentric nucleus due to displacement by accumulation of granules. These granules exhibited yellow-green autofluorescence and staining patterns consistent with ceroid and lipofuscin. Degenerative changes within the CNS were also described (neuronal necrosis, Wallerian degeneration, and axonal dystrophy). Eyes: mild irregular loss of photoreceptor cells; massive accumulation of fluorescent material in the retinal pigmented epithelium. Other organs and structures: Storage product also accumulated within the smooth muscle cells of the intestines, pancreas, urinary bladder, and walls of small arteries. Mode of inheritance: Autosomal recessive inheritance is suspected. -
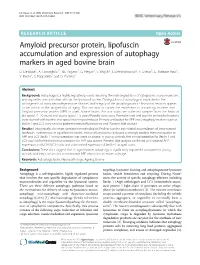
Amyloid Precursor Protein, Lipofuscin Accumulation and Expression of Autophagy Markers in Aged Bovine Brain D
De Biase et al. BMC Veterinary Research (2017) 13:102 DOI 10.1186/s12917-017-1028-1 RESEARCH ARTICLE Open Access Amyloid precursor protein, lipofuscin accumulation and expression of autophagy markers in aged bovine brain D. De Biase1, A. Costagliola1*, T.B. Pagano1, G. Piegari1, S. Wojcik2, J. Dziewiątkowski2, E. Grieco3, G. Mattace Raso4, V. Russo1, S. Papparella1 and O. Paciello1 Abstract Background: Autophagy is a highly regulated process involving the bulk degradation of cytoplasmic macromolecules and organelles in mammalian cells via the lysosomal system. Dysregulation of autophagy is implicated in the pathogenesis of many neurodegenerative diseases and integrity of the autophagosomal - lysosomal network appears to be critical in the progression of aging. Our aim was to survey the expression of autophagy markers and Amyloid precursor protein (APP) in aged bovine brains. For our study, we collected samples from the brain of old (aged 11–20 years) and young (aged 1–5 years) Podolic dairy cows. Formalin-fixed and paraffin embedded sections were stained with routine and special staining techniques. Primary antibodies for APP and autophagy markers such as Beclin-1 and LC3 were used to perform immunofluorescence and Western blot analysis. Results: Histologically, the most consistent morphological finding was the age-related accumulation of intraneuronal lipofuscin. Furthermore, in aged bovine brains, immunofluorescence detected a strongly positive immunoreaction to APP and LC3. Beclin-1 immunoreaction was weak or absent. In young controls, the immunoreaction for Beclin-1 and LC3 was mild while the immunoreaction for APP was absent. Western blot analysis confirmed an increased APP expression and LC3-II/LC3-I ratio and a decreased expression of Beclin-1 in aged cows. -

Immune Clearance of Senescent Cells to Combat Ageing and Chronic Diseases
cells Review Immune Clearance of Senescent Cells to Combat Ageing and Chronic Diseases Ping Song * , Junqing An and Ming-Hui Zou Center for Molecular and Translational Medicine, Georgia State University, 157 Decatur Street SE, Atlanta, GA 30303, USA; [email protected] (J.A.); [email protected] (M.-H.Z.) * Correspondence: [email protected]; Tel.: +1-404-413-6636 Received: 29 January 2020; Accepted: 5 March 2020; Published: 10 March 2020 Abstract: Senescent cells are generally characterized by permanent cell cycle arrest, metabolic alteration and activation, and apoptotic resistance in multiple organs due to various stressors. Excessive accumulation of senescent cells in numerous tissues leads to multiple chronic diseases, tissue dysfunction, age-related diseases and organ ageing. Immune cells can remove senescent cells. Immunaging or impaired innate and adaptive immune responses by senescent cells result in persistent accumulation of various senescent cells. Although senolytics—drugs that selectively remove senescent cells by inducing their apoptosis—are recent hot topics and are making significant research progress, senescence immunotherapies using immune cell-mediated clearance of senescent cells are emerging and promising strategies to fight ageing and multiple chronic diseases. This short review provides an overview of the research progress to date concerning senescent cell-caused chronic diseases and tissue ageing, as well as the regulation of senescence by small-molecule drugs in clinical trials and different roles and regulation of immune cells in the elimination of senescent cells. Mounting evidence indicates that immunotherapy targeting senescent cells combats ageing and chronic diseases and subsequently extends the healthy lifespan. Keywords: cellular senescence; senescence immunotherapy; ageing; chronic disease; ageing markers 1. -

Gait Mechanics in Patients with Chronic Obstructive Pulmonary Disease Jenna M
University of Nebraska at Omaha DigitalCommons@UNO Journal Articles Department of Biomechanics 2-2015 Gait mechanics in patients with chronic obstructive pulmonary disease Jenna M. Yentes University of Nebraska at Omaha, [email protected] Kendra K. Schmid University of Nebraska Medical Center Daniel Blanke University of Nebraska at Omaha, [email protected] Debra J. Romberger University of Nebraska Medical Center Stephen I. Rennard University of Nebraska Medical Center See next page for additional authors Follow this and additional works at: https://digitalcommons.unomaha.edu/biomechanicsarticles Part of the Biomechanics Commons Recommended Citation Yentes, Jenna M.; Schmid, Kendra K.; Blanke, Daniel; Romberger, Debra J.; Rennard, Stephen I.; and Stergiou, Nicholas, "Gait mechanics in patients with chronic obstructive pulmonary disease" (2015). Journal Articles. 128. https://digitalcommons.unomaha.edu/biomechanicsarticles/128 This Article is brought to you for free and open access by the Department of Biomechanics at DigitalCommons@UNO. It has been accepted for inclusion in Journal Articles by an authorized administrator of DigitalCommons@UNO. For more information, please contact [email protected]. Authors Jenna M. Yentes, Kendra K. Schmid, Daniel Blanke, Debra J. Romberger, Stephen I. Rennard, and Nicholas Stergiou This article is available at DigitalCommons@UNO: https://digitalcommons.unomaha.edu/biomechanicsarticles/128 Yentes et al. Respiratory Research (2015) 16:31 DOI 10.1186/s12931-015-0187-5 RESEARCH Open Access Gait mechanics in patients with chronic obstructive pulmonary disease Jennifer M Yentes1*, Kendra K Schmid2, Daniel Blanke1, Debra J Romberger3,4, Stephen I Rennard4 and Nicholas Stergiou1,2 Abstract Background: Chronic obstructive pulmonary disease (COPD) is characterized by the frequent association of disease outside the lung. -

Complement Activation by Photooxidation Products of A2E, a Lipofuscin Constituent of the Retinal Pigment Epithelium
Complement activation by photooxidation products of A2E, a lipofuscin constituent of the retinal pigment epithelium Jilin Zhou*, Young Pyo Jang*, So Ra Kim*, and Janet R. Sparrow*†‡ Departments of *Ophthalmology and †Pathology and Cell Biology, Columbia University, New York, NY 10032 Edited by Nicholas J. Turro, Columbia University, New York, NY, and approved September 19, 2006 (received for review May 23, 2006) Recent studies have implicated local inflammation and activation responsible for activating complement and local inflammatory of complement amongst the processes involved in the pathogen- events are not known, but infectious agents and sequela related esis of age-related macular degeneration (AMD). Several lines of to oxidative processes have been suggested (13, 15). investigation also indicate that bis-retinoid pigments, such as A2E, The complement cascade is an effector system that, upon that accumulate as lipofuscin in retinal pigment epithelial (RPE) activation, generates a number of bioactive products, some of cells, contribute to the disease process. In an investigation of a which including the complement cleavage products C3a and potential trigger for complement activation in AMD, we explored C5a, trigger inflammatory responses (16–18). Activation of the notion that the complex mixture of products resulting from complement can occur by three different pathways, two of photooxidation of A2E might include a range of fragments that these being the classical and alternative pathways. In the could be recognized by the complement system as ‘‘foreign’’ and classical pathway, activation is initiated by binding of protein that could serve to activate the complement system, leading to C1q, the recognition subunit of the C1 complex, to an acti- low-grade inflammation. -

Materials, Methods & Technologies ISSN 1314-7269, Volume 10, 2016
Materials, Methods & Technologies Journal of International Scientific Publications ISSN 1314-7269, Volume 10, 2016 www.scientific-publications.net A RAPID PLATFORM TO GENERATE LIPOFUSCIN AND SCREEN THERAPEUTIC DRUGS FOR EFFICACY IN LIPOFUSCIN REMOVAL Jason Gaspar, Jacques Mathieu, Pedro J. J. Alvarez Rice University Dept. of Civil and Environmental Engineering, Houston, Texas, 77005 Abstract Lipofuscin is a brown-yellow, autofluorescent polymeric material that accumulates in a ceroid manner within postmitotic cells during aging. Lipofuscin accumulation impairs proteosome and lysosome pathways critical to cell health and homeostasis. Therefore, the ability to quickly generate lipofuscin in vitro, and identify drugs that mitigate the accumulation or clear lipofuscin would be of great benefit to aging research. Here, we present a platform to quickly create lipofuscin-loaded (but otherwise healthy) cells and screen drugs for efficacy in lipofuscin removal. The combination of leupeptin, iron (III) chloride and hydrogen peroxide generates significant amounts of lipofuscin within cells while eliminating the need for a 40% hyperoxic chamber. Alternative methods which load fibroblasts with “artificial” lipofuscin obtained via UV-peroxidation of mitochondrial fragments are much more labor-intensive. 7KLVPHWKRGLVIDVWHU GD\V WKDQPRVWSURWRFROVWRJHQHUDWHOLSRIXVFLQDQGDVVHVV its removal, which typically require 2 to 4 weeks or longer to complete. Key words: lipofuscin, flow cytometry, Fenton chemistry, autofluorescence, fluorescent microscopy 1. INTRODUCTION Lipofuscin accumulation has an inverse relationship with lifespan and is a well-documented hallmark of aging. (Nakano et al., 1995; Terman and Brunk, 2004) Many age-related disease states including Alzheimer’s (Moreira et al., 2007), Parkinson’s (Meredith et al., 2002), and age-related macular degeneration (Sparrow et al., 2000) show increased lipofuscin accumulation. -

Implication of Dietary Iron-Chelating Bioactive Compounds in Molecular Mechanisms of Oxidative Stress-Induced Cell Ageing
antioxidants Review Implication of Dietary Iron-Chelating Bioactive Compounds in Molecular Mechanisms of Oxidative Stress-Induced Cell Ageing Alexandra Barbouti 1,* , Nefeli Lagopati 2, Dimitris Veroutis 2, Vlasios Goulas 3 , Konstantinos Evangelou 2, Panagiotis Kanavaros 1, Vassilis G. Gorgoulis 2,4,5,6 and Dimitrios Galaris 7 1 Department of Anatomy-Histology-Embryology, Faculty of Medicine, School of Health Sciences, University of Ioannina, 45110 Ioannina, Greece; [email protected] 2 Laboratory of Histology-Embryology, Molecular Carcinogenesis Group, Faculty of Medicine, School of Health Science, National and Kapodistrian University of Athens, 75, Mikras Asias Str., Goudi, 11527 Athens, Greece; [email protected] (N.L.); [email protected] (D.V.); [email protected] (K.E.); [email protected] (V.G.G.) 3 Department of Agricultural Sciences, Biotechnology and Food Science, Cyprus University of Technology, 3036 Lemesos, Cyprus; [email protected] 4 Biomedical Research Foundation Academy of Athens, 11527 Athens, Greece 5 Faculty of Biology, Medicine and Health Manchester Cancer Research Centre, Manchester Academic Health Sciences Centre, University of Manchester, Manchester M13 9PL, UK 6 Center for New Biotechnologies and Precision Medicine, Medical School, National and Kapodistrian University of Athens, 11527 Athens, Greece 7 Laboratory of Biological Chemistry, Faculty of Medicine, School of Health Sciences, University of Ioannina, 45110 Ioannina, Greece; [email protected] Citation: Barbouti, A.; Lagopati, N.; * Correspondence: [email protected]; Tel.: +30-2651007613 Veroutis, D.; Goulas, V.; Evangelou, K.; Kanavaros, P.; Gorgoulis, V.G.; Abstract: One of the prevailing perceptions regarding the ageing of cells and organisms is the Galaris, D. Implication of Dietary intracellular gradual accumulation of oxidatively damaged macromolecules, leading to the decline of Iron-Chelating Bioactive Compounds cell and organ function (free radical theory of ageing). -
Autofluorescence: Causes and Cures
Autofluorescence: Causes and Cures Table of contents 1 Introduction.....................................................................................................................................2 2 Natural Fluorescence.....................................................................................................................3 2.1 Lipofuscins ............................................................................................................................................... 3 2.1.1 Protocols for reducing Lipofuscin fluorescence ........................................................................ 3 2.2 Elastin and Collagen ................................................................................................................................ 4 2.2.1 Protocol for reducing Elastin fluorescence ............................................................................... 4 3 Fixative-induced fluorescence......................................................................................................5 3.1 Protocols for reducing fixative-induced fluorescence.......................................................................... 5 3.1.1 Sodium Borohydride ................................................................................................................ 5 3.1.2 Trypan Blue treatment ............................................................................................................. 6 3.1.3 Avoiding Aldehyde fixatives .................................................................................................... -

Lipofuscinosis of the Gastrointestinal Tract in Man
J Clin Pathol: first published as 10.1136/jcp.20.6.806 on 1 November 1967. Downloaded from J. clin. Path. (1967), 20, 806 Lipofuscinosis of the gastrointestinal tract in man BERNARD FOX From the Department of Morbid Anatomy, Charing Cross Hospital Medical School, London SYNOPSIS Three illustrative cases of lipofuscinosis of the gastrointestinal tract are presented. The nature and significance of this condition are discussed. When the pigment is found in surgical biopsy material steatorrhoea, hypoalbuminaemia, and vitamin E deficiency should be excluded. It is probable that this type of lipofuscinosis is a manifestation of vitamin E deficiency in man. Brown pigmentation (lipofuscinosis) of the bowel This paper describes three cases of lipofuscin was first recorded in necropsy material from patients pigmentation of the gastrointestinal tract discovered dying from a variety of diseases (Blaschko, 1883; in surgical biopsy material, describes in detail the Scheimpflug, 1885). The pigmentation was described histological distribution and staining characteristics as being mainly in the small intestine and was of the pigment, discusses the significance of the thought to be a degenerative change. Pappenheimer finding, and emphasises its diagnostic value in the and Victor (1946) reported pigmentation in the malabsorption syndrome, hypoproteinaemia, and smooth muscle of the oesophagus, stomach, and vitamin E deficiency. small intestine in necropsy material from patients with the malabsorption syndrome. This observation CASE REPORTS copyright. has been confirmed in idiopathic steatorrhoea CASE 1 A 61-year-old man was admitted to hospital (Adlersberg and Schein, 1947; Ansanelli and Lane, in 1963 for investigation of indigestion and recent loss 1957; Gresham, Cruickshank, and Valentine, 1958; of 13 kg. -

Formation of Lipofuscin-Like Autofluorescent Granules
bioRxiv preprint doi: https://doi.org/10.1101/2021.02.23.432539; this version posted February 23, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-ND 4.0 International license. FORMATION OF LIPOFUSCIN-LIKE AUTOFLUORESCENT GRANULES IN THE RETINAL PIGMENT EPITHELIUM REQUIRES LYSOSOME DYSFUNCTION Cristina Escrevente1, Ana S. Falcão1, Michael J. Hall2, Mafalda Lopes-da- Silva1, Pedro Antas1, Miguel M. Mesquita1, Inês S. Ferreira1, M. Helena Cardoso1, Ana C. Fradinho1, Clare E. Futter2, Sandra Tenreiro1 and Miguel C. Seabra1,2 1 iNOVA4Health, CEDOC - Chronic Diseases Research Center, NOVA Medical School, Universidade Nova de Lisboa, 1169-056 Lisboa, Portugal 2 UCL Institute of Ophthalmology, London, UK. Correspondence: Miguel C. Seabra, CEDOC - NOVA Medical School, Universidade Nova de Lisboa, 1169-056 Lisboa, Portugal Short Title: Lysosome Dysfunction and Autofluorescent Granules Keywords: retinal pigmented epithelium; photoreceptor outer segments; autofluorescent granules; lipofuscin; lysosome dysfunction Grant Support: 1 bioRxiv preprint doi: https://doi.org/10.1101/2021.02.23.432539; this version posted February 23, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-ND 4.0 International license. This work was supported by Fundação para a Ciência e Tecnologia (FCT) – Portugal co-funded by FEDER under the PT2020 Partnership Agreement (to MCS, including project PTDC/MED-PAT/30385/2017, iNOVA4Health- UIDB/04462/2020, research infrastructure PPBI-POCI-01-0145-FEDER-022122, M-ERA.NET 2/0005/2016), Boehringer Ingelheim (to MCS), Fight for Sight UK (to MCS), Wellcome Trust grant number 212216/Z/18/Z/ (to CEF).